
Abstract
Describe patient social needs in a large midwestern health care system. Health care systems are increasingly interested in addressing social needs in the clinical setting for improved health outcomes and lower costs. This retrospective cross-sectional analysis of health records data was a population health pilot project which tested a digital platform to screen and refer patients for social needs across three community hospitals serving Chicago and its South Suburbs. The analysis reports on social needs identified based on the referrals made. Electronic health record data were linked to the referral data to describe patient clinical and demographic characteristics. A total of 2909 patients had at least 1 social need identified. The mean age was 49 years ±21.7 and 65.7% were women. Only 33% of patients had 1 social need identified, indicating that if a social need is identified for patients, they most likely have social needs from other categories as well. Patients of color, specifically African American patients, were 14% more likely to have at least 3 social need categories identified (95% confidence interval of relative risk: 1.02–1.29). Financial stability was the most commonly reported social need (50.7%), followed by food and nutrition (43%). Transportation (22%) and housing (21%) were also commonly reported. This population health initiative reveals that many patients accessing health care have multiple social needs that can be identified at the point of care, and patterns of need-based referral vary by patient clinical and demographic characteristics.
Introduction
The United States,
In response to the overwhelming evidence showing that addressing social needs in the clinical setting results in improved health outcomes, and lowers health care resource utilization and costs, the National Academy of Medicine, Centers for Disease Control and Prevention, and Centers for Medicare & Medicaid Services have all called for evidence-based initiatives to better screen for and address these needs. 5 –7 Social determinants of health (SDOH) are defined as “the conditions in which people are born, grow, work, live, age, and the wider set of forces and systems shaping the conditions of daily life.” 8
Screening for any condition in isolation without the capacity to ensure referral and linkage to appropriate resources to address these needs is ineffective and, arguably, unethical. 7 Initiatives are being developed and tested in the health care setting to screen for social needs as well as provide referrals to community resources that can address identified needs. There are challenges to implementing these initiatives in the clinical setting largely because health care and social resources are provided in different locations. Health care resources are usually provided in a clinical setting, while social resources are usually provided in a community setting. 9
This has spurred the adoption of tools that integrate with electronic health records (EHRs) to help coordinate care beyond hospital walls. EHR tools can help facilitate data aggregation without additional administrative burden to physicians and identify individual risk factors and the need for referrals. 9 These tools have been implemented at different levels, and multiple barriers have been reported in identifying the best ways to integrate tools into existing workflow processes and ensuring that staff tasked with screening efforts receive adequate tool training, access, and the time to complete data collection. 10,11 There is also a lack of consensus on standards for collecting these data in EHR and insufficient evidence that once information is collected, social needs can be effectively addressed through referrals or other action tools. 12
Advocate Aurora Health (AAH), spanning Illinois and Wisconsin and the 10th largest not-for-profit health care systems in the United States, piloted a quality improvement initiative to electronically screen for SDOH within its integrated (inpatient and outpatient) care management program at 3 hospital sites located in south of Chicago, IL. This report describes the types of social needs identified by patients who participated in this pilot project.
Methods
Screening and referral workflow
This innovative population health pilot project included screening and referring patients for social needs using the NowPow, a Unite Us company, platform, which maintains a frequently updated inventory of community resources to help people stay well, meet basic needs, and manage illness and care for others. All resources are deeply indexed at the service level, with detail on service restrictions, eligibility requirements, language(s) spoken, and other critical access factors. 13 Information about the patients (eg, social need(s), age, address, gender, language) is matched with available resources, which are shared with the patients in their preferred language through text, e-mail, and/or print. 13
A modified version of the PRAPARE was also made available within the platform to support streamlined screening and referral workflows. 14 The pilot project was initiated at 3 community hospital service areas in the south side of Chicago, IL. Patients were screened using the survey and were provided with community resources as applicable during or after an encounter with the health system.
Clinical team members, including care managers and community health workers, ask screening questions about having adequate food, housing, transportation, or other needs, to create a picture of a patient's barriers to care referred to as social needs. Based on the patient's social data, the resource referral platform then queries its extensive database of >5500 organizations and offering >16,000 services in Cook County alone, across 22 service categories and >200 service types. 15 It links patients to services in their local neighborhood (eg, job training, housing assistance, help with transportation, meal sites, food banks, government resources).
For purposes of this analysis, authors identify and describe patient social needs based on the service category of referrals shared and not based on the screening itself, although some patients included did complete the PRAPARE tool most did not. Therefore, the patients included in this analysis had at least 1 social need identified. The frequency of these social needs and explore associations with patient clinical and demographic characteristics is described.
Data sources and patient population
Patients with at least 1 referral (made through the referral platform) between November 2018 and November 2020 were included in the analysis. Referrals were used to identify patient social needs using a list of 22 possible service categories in the resource directory taxonomy.
Patient demographic and clinical characteristics were extracted from hospital EHRs. Patient comorbidities were extracted using International Classification of Diseases, 10th Revision (ICD-10) codes. Race and ethnicity were identified from self-reported data in the EHR. Patients are asked to choose from a list of race options, including but not limited to Caucasian, African American, Hispanic, Asian or others (American Indian or Alaskan Native, Native Hawaiian or other Pacific Islander), or unknown. In this analysis, the small fraction of patients who reported race/ethnicity as Asian, American Indian or Alaskan Native, Native Hawaiian or other Pacific Islander, unknown, or declined to answer were grouped under “other.”
Patients were also asked to choose from a list of ethnicity options, including Hispanic/Latino or non-Hispanic/Latino. Race and ethnicity were combined, referred to hereon as race/ethnicity, and patients who reported to be Hispanic/Latino were categorized as Hispanic/Latino regardless of selected race.
Statistical analysis
Patient characteristics are presented with means and standard deviations or medians and interquartile ranges as applicable for continuous variables, and as proportions and absolute numbers for categorical variables. Adjusted logistic regression models were developed to explore characteristics of patients with 3 or more needs categories. Results are presented as relative risk (RR) and 95% confidence internals (CI) and were adjusted for age, gender, race/ethnicity, insurance, and comorbidities (hypertension, asthma/chronic obstructive pulmonary disease [COPD], atherosclerotic cardiovascular disease [ASCVD], diabetes, renal disease, and depression). Analyses were completed using SAS statistical package (release 9.4; SAS Institute, Inc., Cary, NC). This study was approved as non-human subject research by the Advocate Health Care Institutional Review Board.
Results
During the 2-year pilot study, 2909 patients who had at least 1 encounter at 1 of the 3 hospitals included in the pilot project and were referred to at least 1 community resource through the platform were included in this analysis (Table 1). The mean age was 49 years ±21.7 and 65.7% were women. Two thirds of the patients (66.5%) were African American and 15.7% were Hispanic/Latino.
Characteristics of Patients Referred to At Least 1 Community Resource (N = 2909)
ASCVD, atherosclerotic cardiovascular disease; COPD, chronic obstructive pulmonary disease; SD, standard deviation.
A third of the patients had Medicare (32.5%) and a third had Medicaid or Medicare/Medicaid (34.4%), the remaining patients had commercial insurance (19.1%) or were uninsured (14.1%). Over half of the patients (55.9%) had hypertension, 22.6% had diabetes, and 31.2% had history of ASCVD defined as documented history of myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, or atrial fibrillation.
A heat map was created to illustrate the geographic distribution of patient needs by median number of service categories per zip code across the serviced areas (Fig. 1). Only 33% of patients had 1 service category identified, 23% had 2 service categories identified, and 15% had 3 service categories identified (Fig. 2). The remaining patients had >3 service categories. Table 2 explores patient characteristics associated with having 3 or more service categories.

Patient-reported median number of identified needs by zip code in the Chicagoland area (N = 2909). Map reports data on all patient zipcodes excluding 13 patients without valid addresses or located outside this map's boundary.

Number of social need categories identified based on the type of community resources. Overall, 2909 patients had a total of 3243 social need categories identified based on their social needs screening.
Proportion and Relative Risk of Identifying 3 or More Social Need Categories (vs. 1–2) by Demographic Characteristics (N = 2909)
Estimated by log binomial regression, adjusted for age, gender, race/ethnicity, insurance, hypertension, asthma/chronic obstructive pulmonary disease, cardiovascular disease, diabetes, renal disease, and depression.
CI, confidence interval; RR, relative risk.
In adjusted analysis, African American patients (adjusted RR [aRR]: 1.14, 95% CI: 1.01–1.28) were more likely to have at least 3 service categories compared with patients who are Caucasian. Patients on Medicaid (aRR: 1.29, 95% CI: 1.15–1.46) were more likely to have at least 3 service categories compared with patients with commercial insurance. Similarly, patients who are uninsured (aRR: 1.34, 95% CI: 1.16–1.54) were more likely to have at least 3 service categories compared with patients with commercial insurance.
Figure 3 shows the service categories identified in this patient population ranked in frequencies. Financial stability was the most commonly reported service category (50.7%), followed by food and nutrition (43.0%), transportation (22.0%),and housing (21.0%). Supplementary Figure S1 shows the prevalence of community resource types within each service category. For example, under financial stability, patients were most commonly referred to resources to assist with utility payments (n = 1293 referrals) and rent and mortgage payments (n = 1209 referrals).
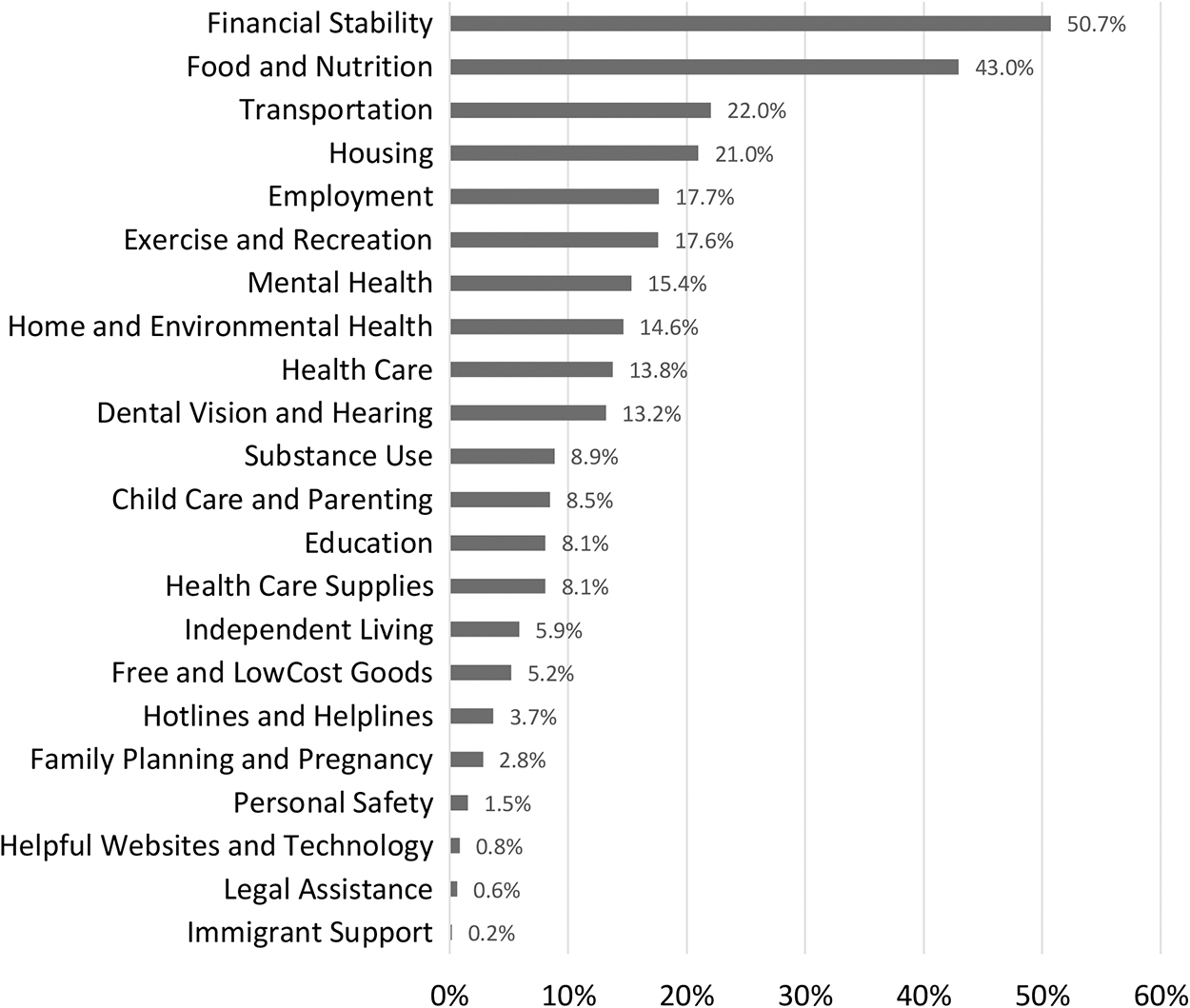
Proportion of referrals within each social need category. Patients may be included under multiple social need categories and, therefore, proportions add up to >100%.
Figure 4 presents the 5 most prevalent service categories by patient comorbidities. Trends indicate that financial stability-related service categories were most commonly reported in patients with asthma or COPD (51.8%). Food and nutrition service categories were most commonly reported in patients with diabetes (44.7%). Transportation service categories were most commonly reported in patients with cardiovascular disease (35.0%). Housing service categories were most commonly reported in patients with asthma/COPD (22.2%). Employment service categories were most commonly reported in patients with asthma/COPD (16.3%).
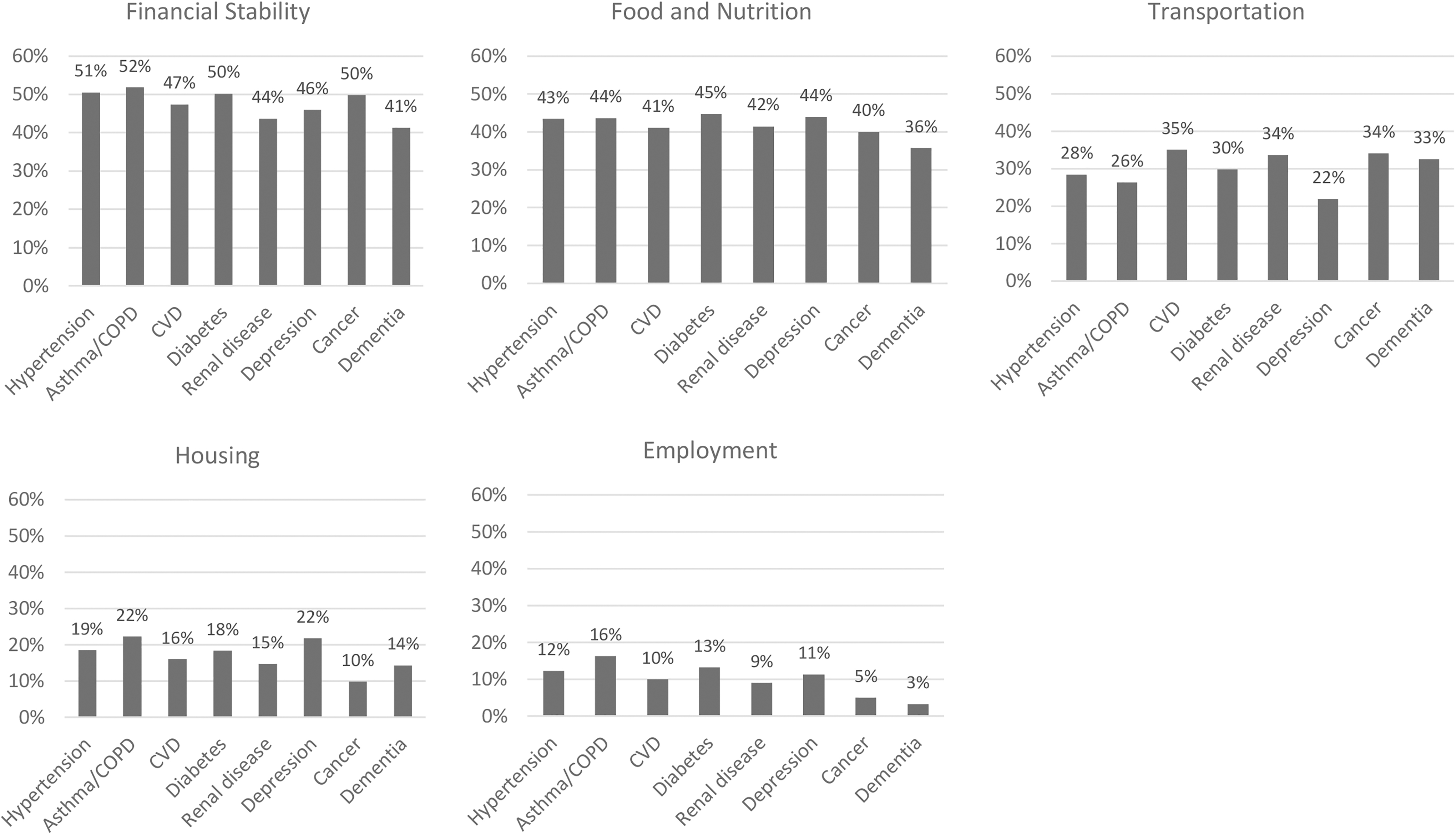
Percentage of patients with each of the 5 most commonly reported social need categories by patient comorbidities (N = 2909). COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease.
Discussion
Authors used data generated from a population health innovation pilot project implemented at 3 community hospitals in the south Chicagoland area to describe patient social needs. Results show that patients tend to have multiple needs based on service categories they were referred to, indicating that social needs aggregate within patients. Results also indicate that patients of color, specifically Black/African American patients, are more likely to have multiple social needs compared with Caucasian patients, even after adjusting for potential confounders.
There was a trend for variations in social needs based on patient comorbidities although it was hard to ascertain since chronic diseases tend to aggregate in patients. For example, food and nutrition needs were most commonly reported among patients with diabetes. Whereas transportation needs were most commonly reported among patients with history of ASCVD and renal disease.
Health care systems acknowledge the importance of identifying and addressing social needs in the clinical setting. 16,17 However, information on well-established programs that screen patients for social needs systematically refers patients to resources in the community, and receives feedback on attendance and on effectiveness, remains limited. 18 The literature includes a few pilot projects that evaluated some of these components in addressing social needs. For example, a pilot study screened 3048 patients in 3 family medicine clinics over a 90-day period in Albuquerque, New Mexico. 19
Results showed that 46% of patients screened positive for at least 1 area of social need, and 63% of those had multiple needs. Most of these needs were previously unknown to clinicians, highlighting the need to systematically screen patients. Qualitative data indicate satisfaction with programs evaluating and screening for social needs as well as patient-reported improvement in health outcomes and healthy behaviors 20 as well as increased confidence in finding resources for self-care. 15
There is a call to identify and address social needs in the clinical setting, yet implementation into the real world is challenging and as a result data describing social needs for patients attending health care are limited. That said, in this analysis, authors were able to describe social needs in a subset of close to 3000 patients attending 1 of 3 community hospitals in the Chicagoland area and results were linked to EHR data to explore how patient demographic and clinical characteristics may impact social needs. A few limitations to this analysis were noted. First, the analysis is based on a population health innovation initiative that did not include specific inclusion criteria, presenting possible bias in the study sample.
Therefore, it is difficult to generalize these results to a broader patient population. It is also difficult to report the prevalence of patients with social needs because a clear cohort or denominator is not identified. Second, authors used referral data instead of screening data to identify patient social needs. The results are consistent with the literature, indicating that among patients who report social needs, most report multiple needs and that financial insecurity-related needs tend to be the most common need. 19 Third, the data report on needs identified but do not address whether the patient was able to access the community resource, that is, closing the referral loop.
Furthermore, there is currently no information on how attending these community resources improves health outcomes. AAH is working with community collaboratives, including IMPACT Connect, to partner with other health systems to standardize the work and engage community-based organizations together. The system is also taking the next phase by working with engaged community partners to understand the referral closure rate to better understand the long-term impact.
In conclusion, the population health innovative initiative reveals that many patients visiting health systems have 1 or more social need that can be identified at the point of care, and patterns of need-based referral vary by patient clinical and demographic characteristics. The pilot project reinforces the feasibility of identifying social needs in the clinical setting and acting on results by referring patients to community resources to address these needs.
Footnotes
Acknowledgments
The authors thank Brian Riordan, Implementation Consultant, Value Based Programs, Advocate Aurora Health, for his ongoing feedback throughout the project on how NowPow, a Unite Us company, was operationalized on site. The authors also thank Mia Spitz, Account Manager, and Gillian Feldmeth, NowPow, a United Us company, for their constructive feedback on the article.
Authors' Contributions
Drs. Khatib, Li, and Siddiqi and Ms. Glowacki all contributed to writing, reviewing, and revising the manuscript. Drs. Khatib and Li performed all study design and data analyses.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.