
Abstract
Although several obesity clinical practice guidelines are available and relevant for primary care, a practical and effective medical model for treating obesity is necessary. The aim of this study was to develop and implement a holistic population health-based framework with components to support primary care-based obesity management in US health care organizations. The Obesity Care Model Collaborative (OCMC) was conducted with guidance and expertise of an advisory committee, which selected participating health care organizations based on prespecified criteria. A committee comprising obesity and quality improvement specialists and representatives from each organization developed and refined the obesity care framework for testing and implementing guideline-based practical interventions targeting obesity. These interventions were tracked over time, from an established baseline to 18 months post implementation. Ten geographically diverse organizations, treating patients with diverse demographics, insurance coverage, and health status, participated in the collaborative. The key interventions identified for managing obesity in primary care were applicable across the 4 OCMC framework domains: community, health care organization, care team, and patient/family. Care model components were developed within each domain to guide the primary care of obesity based on each organization's structure, resources, and culture. Key interventions included development of quality monitoring systems, training of leadership and staff, identifying clinical champions, patient education, electronic health record best practice alerts, and establishment of community partnerships, including the identification of external resources. This article describes the interventions developed based on the framework, with a focus on implementation of the model and lessons learned.
Introduction
In the United States, obesity rates have been increasing since 1999–2000, reaching 42.4% of adults in 2017–2018. 1 Obesity is known to increase the risk of chronic diseases such as type 2 diabetes, hypertension, and dyslipidemia. 2 It also is known that fat loss can ameliorate multiple obesity-related complications and improve quality of life, and also may reduce premature all-cause mortality. 3 Although weight maintenance can be challenging, effective lifestyle interventions delivered individually, in groups, or digitally, result in at least short-term weight loss. 4 Pharmacotherapy options also have proven to be safe and effective for greater and more sustained weight loss as adjuncts to lifestyle modification, 5,6 and metabolic/bariatric surgery has been refined for greater safety and efficacy. 5,6
The American Association of Clinical Endocrinologists (AACE) with the American College of Endocrinology, 4 the Endocrine Society, 7 the American Heart Association/American College of Cardiology/Obesity Society, 8 and other medical professional societies have issued comprehensive evidence-based recommendations to guide health care professionals in the treatment of patients with obesity. These guidelines highlight the importance of diagnosing and evaluating patients for weight-related complications and applying treatment approaches involving lifestyle changes and behavioral therapy, to be used in combination with pharmacotherapy or metabolic surgery, when indicated. The AACE guidelines, in particular, emphasize treatment intensification based on the risk, presence, and severity of obesity complications. 4 Given the chronic nature of obesity, patients should be followed up long term and periodically re-evaluated for weight regain and response to weight loss therapy.
Despite advances made in therapies and the existing guidelines, meaningful clinical improvements in treating obesity at a population level are not being achieved. Multiple causative factors include patient self-blame and stigmatizing attitudes, inaction by health care professionals related to time constraints, insufficient knowledge of pathophysiology, lack of reimbursement for diagnosing and/or counseling patients, 9 and restricted coverage of anti-obesity medications and bariatric surgery by health insurance plans. 10 Additionally, social stigma can have a negative effect on patients' physical and mental health and create a disinclination to seek care. 11
In recognition of the complex nature of obesity, patient-centered, multidisciplinary strategies providing individualized care are paramount 12,13 and may lead to improved clinical outcomes, patient adherence and satisfaction, and reduced health care costs and resource utilization. 14 Because the majority of interactions between patients and health care providers occur in the primary care setting, and an obesity diagnosis is known to be associated with weight loss, 15 the diagnosis should be considered as a first step in the treatment process. Thus, primary care providers (PCPs) are uniquely positioned to screen patients for obesity and provide access to effective treatment. 2 Collaboration between PCPs and other specialists in primary care-based models of health care delivery constitutes an effective approach to sustainable weight loss and maintenance. 16 However, <30% of patient visits in the primary care setting in 2008–2013 in the United States resulted in a diagnosis of obesity. 17
Provision of a care delivery model for practical use in the primary care setting that incorporates obesity treatment guidelines thus may improve the uptake and effectiveness of the current interventions for obesity. However, there is currently limited information in the literature on obesity care models that focus on primary care, and no holistic model of primary care has been developed specifically for health systems. AMGA (American Medical Group Association) is a nonprofit trade association that represents ∼440 of the nation's multispecialty medical groups and integrated delivery systems. AMGA provides support in the form of advocacy, education, quality performance improvement, research and analytics, and financial and operational assistance. Based on a survey developed by AMGA, which revealed that the majority of the responder health care organizations (HCOs) did not follow the current recommendations or any particular algorithms for obesity management, the research team identified gaps in knowledge in the organizations in order to develop a care model within a proposed framework, with the needed flexibility to make it contextually appropriate to health care systems. The goal of this initiative was to enable HCOs to determine optimal approaches for integrating the model into their own systems and, in turn, to develop individual care models. This article reports on the development and implementation of a population health-based care model to manage obesity in the primary care setting in the United States and describes key insights (ie, best practices) gathered from across the collaborative.
Methods
Concept and organization of the Obesity Care Model Collaborative
The Obesity Care Model Collaborative (OCMC) was a 35-month (from development to data analysis/publication) program development initiative, led by AMGA, that aimed to define, test, and evaluate a framework for obesity management for primary care in multispecialty medical groups, integrated health systems, and academic medical centers (Figure 1). The objective was to develop a model of care that could be tailored to the individual organizations according to their specific contexts. Ten AMGA-member HCOs were selected by a national advisory committee, based on their ability to contribute to the development of the framework and measures, and their commitment to implement an obesity program including a minimum required range of services, either within the HCO or through referral partnerships.
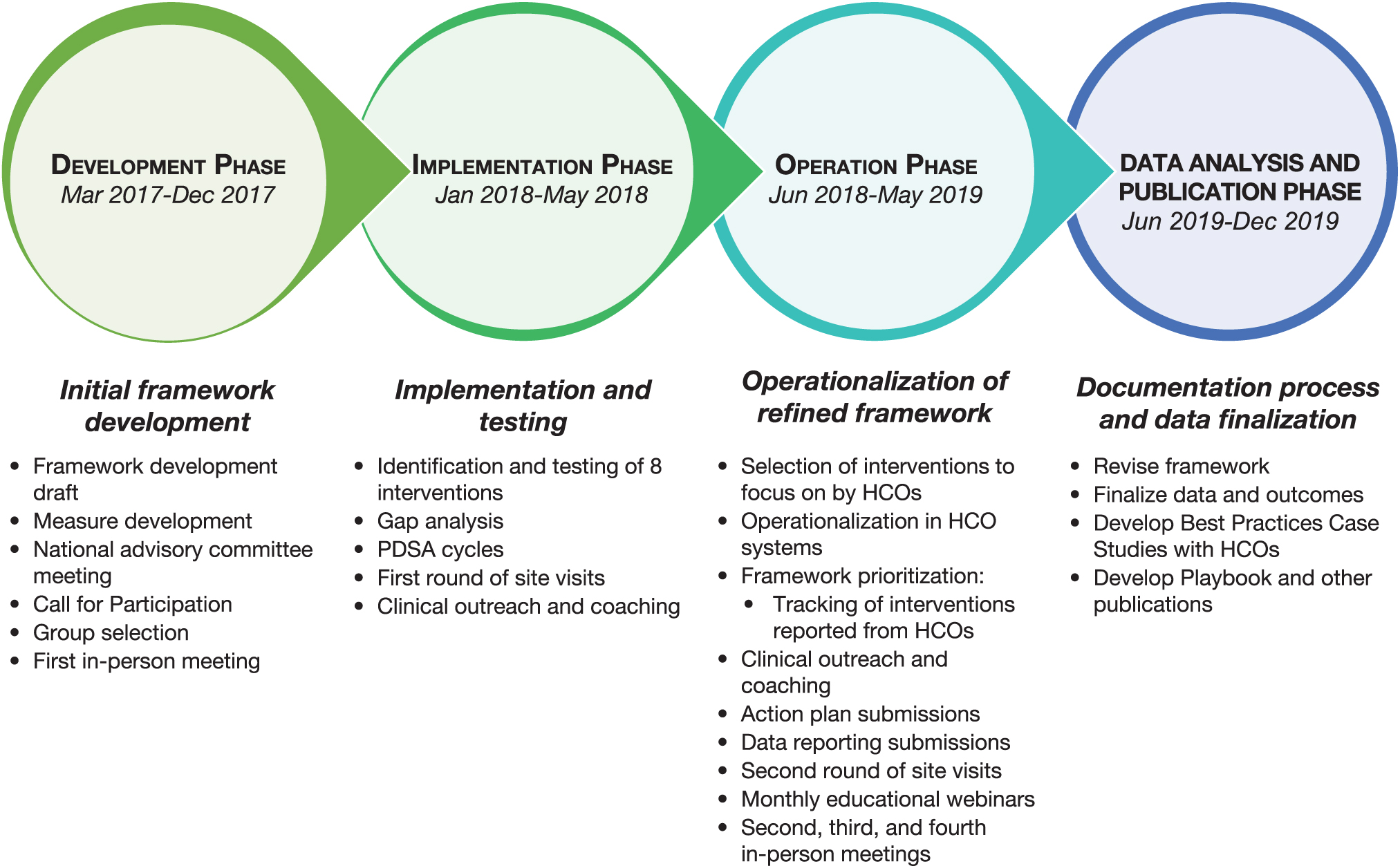
Flow diagram for the development and implementation of interventions under the collaborative. HCO, health care organization; PDSA, Plan-Do-Study-Act.
A primary care, population-based approach was applied to obesity management. Each HCO selected 1 representative to serve as an organization advisor and to participate in 1 of 2 committees dedicated to either framework development or measure design. The committees included medical and quality directors, program and project managers, professors/researchers, nurses, physicians, and specialists in internal medicine, endocrinology, or obesity medicine, and members of specialty and advocacy organizations. (Additional details on membership requirements and responsibilities are in Committee member selection and roles in the Supplementary Material, available with the article online).
The Framework Committee, which included 12 members, focused on the development of the obesity care model and its components (ie, interventions) to be tested and implemented by the participating HCOs (detailed information on processes during implementation are in Model development in the Supplementary Material). The Measures Committee, comprising 8 members, developed and refined operational and quality performance measures and their specifications (ie, diagnosis rates, assessment for complications and complication rates, weight change, use of anti-obesity medications, patient-reported outcomes) to be reported by each participating HCO. Results of the measure development work are reported elsewhere. 18 One of the measures developed in this collaborative, obesity diagnosis, went through a formal testing process to ultimately prepare it for endorsement by the National Quality Forum (S.L. Sampsel, personal communication).
Selection of participating centers and initiatives and development and implementation of the model
HCOs responded to a Call for Participation and underwent a robust selection process, which started with the submission of an application for consideration. Applications were ranked and, if the HCOs met the inclusion criteria, they were interviewed. HCOs were then selected by the national advisory committee according to predefined criteria (see Organization selection and inclusion criteria in the Supplementary Material).
AMGA researched the existing obesity models, frameworks, and algorithms focused on primary care and conducted a survey to determine the extent to which medical societies' recommendations were being followed by the HCOs. Several meetings were held to discuss the gaps identified, and 4 obesity care domains were developed. These domains, essential for any obesity management program, had to be translatable across all types of medical groups and health systems and able to be implemented in primary care using a population health approach. The 4 Care Model Domains are presented in Table 1. Interventions that were likely to lead to improved obesity care and feasible to implement were identified based on current practice guidelines, and were developed and tested by participating HCOs in the identified 4 Care Model Domains. (The specific steps followed are described in Domain definition and intervention identification in the Supplementary Material.)
Description of the Framework Domains
HCO, Health Care Organization.
Insights, successes, and challenges were shared among the member organizations during in-person meetings, monthly outreach calls, site visits, and monthly webinars. Topics of discussion and objectives of these meetings are described in detail under Model development in the Supplementary Material. Based on the data produced by the HCOs and their shared experiences, the care model and measures were modified by the Framework Committee and Measures Committee using an iterative process.
Interventions were implemented and tested using quality improvement tools such as gap analysis and Plan-Do-Study-Act cycles. The HCOs actively participated in 2 phases of the initiative: the implementation (6 months) and operation (12 months) phases. AMGA conducted the first round of site visits at each HCO during the 6-month implementation phase. For 12 months during the subsequent operation phase, the applied interventions and patient outcomes were tracked using action plans that were submitted quarterly; this phase included a second round of site visits (Figure 1). AMGA and the national advisory committee assisted with adapting and implementing the model and with translation of emergent best practices across the different participating groups.
For the period of 12 months of the operation phase, qualitative and quantitative data were collected for analysis. The interventions were tracked, by domain, using the Expert Recommendations for Implementation Science (ERIC) 19 for similarities across HCOs, and learnings were applied and compared with the original model developed at the beginning of the collaborative. Subsequently, an Obesity Care Model and Obesity Care Model Playbook 20 were developed to guide organizations treating patients with obesity in the primary care setting, and best practices were identified.
Results
Participating organizations
Ten diverse HCOs were selected from 20 final applicants to participate in the collaborative based on the inclusion criteria and in-depth interviews (Table 2). 21 –30 The sites were located in 10 states representing all regions of the United States (West, Northeast, South, Midwest), where primary care populations ranged from ∼44,000 to ∼600,000 active patients. The HCOs were located in urban and rural areas and served a broad range of patients in terms of demographics, insurance status, and health status. Two of the HCOs applied their program to their entire patient population, whereas the other 8 focused on a subset of their patient population (eg, selected primary care sites, dedicated obesity clinic).
Description of Participating Organizations
PCP, primary care physician.
The obesity management interventions across the different Care Model Domains that were identified by the participating HCOs were tested, and those that were successful were implemented by 1 or more organizations. (A complete list of all the interventions in the collaborative is in Interventions for participating organizations in the Supplementary Material.)
Obesity care model
The gaps and limitations identified by participating sites in the development phase helped inform the initiatives implemented during the collaborative. Based on the experiences of the collaborative participants, individual obesity programs were developed by the HCOs using the rubric of the 4 domains in the Framework (Figure 2), and key interventions were identified.
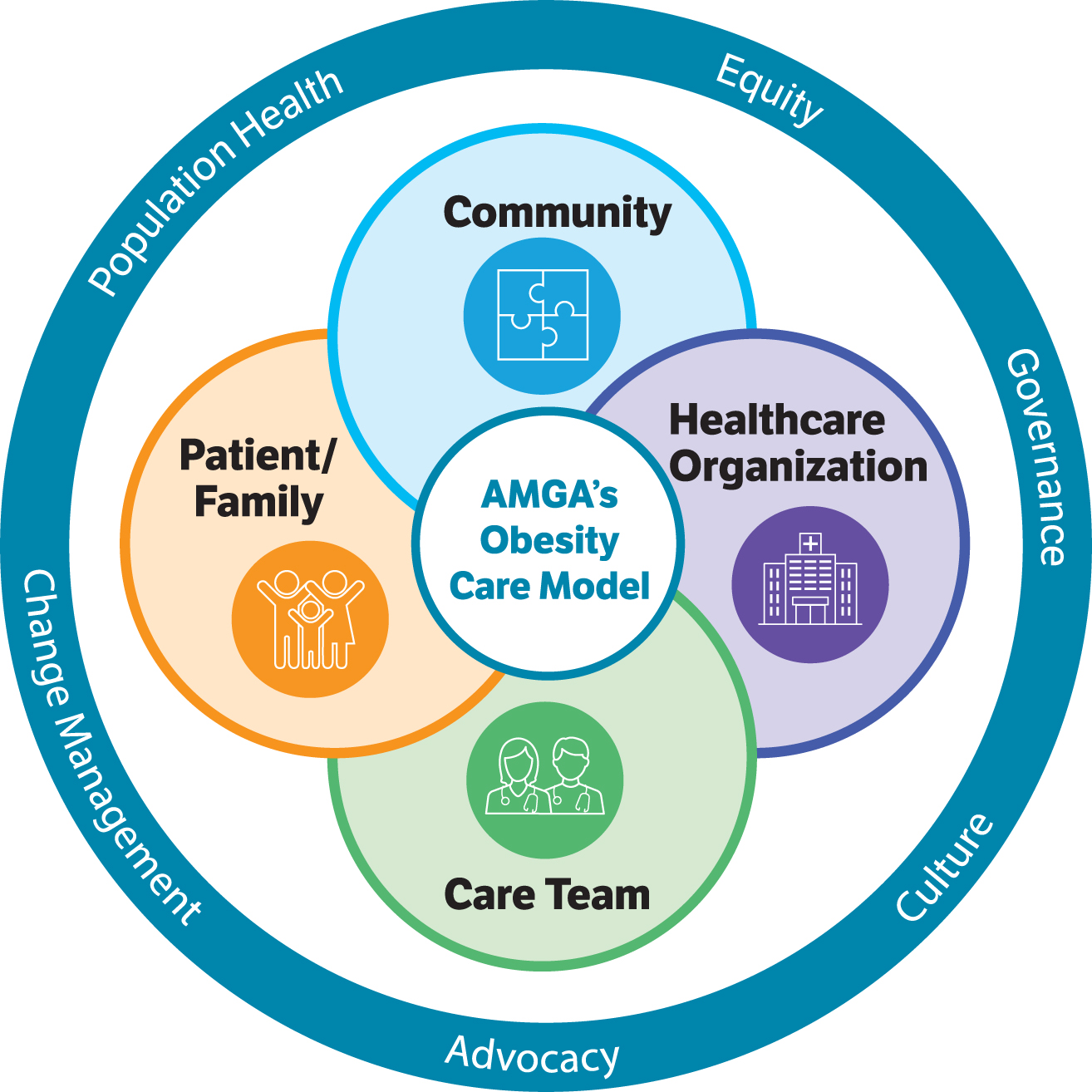
AMGA's Obesity Care Model Collaborative competencies. 20 AMGA, American Medical Group Association.
For the Community domain, 4 main interventions were: (1) to promote and disseminate local initiatives/resources beneficial to patients with obesity; (2) to establish collaborations with businesses and community organizations to increase awareness and healthy habits; (3) to create community partnerships for the remediation of the identified gaps; and (4) to identify “community champions” to facilitate these partnerships.
The 5 main goals within the Health Care Organization domain were: (1) to create system-wide weight management steering committees and designate “clinician champions” (eg, nurses, physician assistants) responsible for the assessment of readiness and the identification of barriers to the implementation of an obesity program; (2) to apply “train-the-trainer” strategies, implement training or continuing medical education initiatives, and develop documentation/assessment tools for PCPs and other staff members involved in the care of patients with obesity; (3) to improve diagnosis rates and treatment outcomes through the implementation of best practice alerts incorporated into electronic health records (EHRs), create patient registries, and implement effective documentation and/or monitoring processes such as dashboards to manage productivity; (4) to apply financial and nonfinancial incentives for provider performance and compensation; and (5) to develop patient education materials.
At the level of the Care Team domain, 3 key interventions included: (1) increasing awareness of obesity and weight management strategies consistent with professional national obesity guidelines (including pharmacotherapy) among providers; (2) implementing coaching/education initiatives on how to discuss obesity and its treatment with patients; and (3) supporting and integrating a multidisciplinary team into the workflow that is adequately equipped with tools and techniques to facilitate screening, evaluation, monitoring, and counseling.
Finally, in the Patient/Family domain, 3 key interventions involved: (1) assisting patients with identification of clinicians with expertise and/or genuine interest in weight management; (2) enlisting patient/family advocates or patient advisory groups to represent their perspectives on obesity programs, from planning to implementation stage, and to provide input into quality of care and the patient experience; and (3) providing educational materials to patients such as tools that inform patients about treatment plans, handouts, face-to-face and online classes, and use of social media.
In order to determine opportunities for improvement, HCOs first had to identify gaps and challenges in their respective systems. Gaps and challenges varied for each HCO, and different approaches were taken to address them within each domain. In the Community domain, many HCOs saw a gap in needs assessments to determine the adequate programs and resources needed for their systems. This provided a way for them to address their readiness and identify barriers to the development of initiatives. Others realized there were few community resources available for their patients and identified a need to conduct a community assessment and collaborate with the community to provide resources and services.
For the Health Care Organization domain, some of the gaps identified included lack of a formal business case (ie, written proposal providing the rationale for financial investment in a quality improvement program, with focus on direct financial, strategic, and internal organization) 31 and cultural sensitivity to treat obesity, and obesity not constituting an area of focus for the organization. Some HCOs were further along in the collaborative than their peers; therefore, starting from the top and obtaining buy-in from leadership was essential to a successful program. This meant that they were invested in the program and would provide the necessary resources and establish it as an organizational priority to ensure its success.
Training and education for the Care Team was insufficient in some HCOs. The ability to have conversations without bias and with knowledge of the disease is essential to organizations, and many HCOs focused on implementing provider and staff educational initiatives. For the Patient/Family domain, adequate education for patients around disease awareness and impact was a challenge for some of the HCOs. Therefore, many of them saw it as an opportunity to address this issue through patient education tools and classes. Finally, gathering patients' perspectives on their own care was both a gap and challenge. This information was essential to HCOs to measure how patients viewed their health and received care. While a few HCOs had some success with implementing Patient-Reported Outcomes Measures (PROMs), many experienced challenges with administering and collecting the surveys.
The gaps and challenges for each domain, as well as the recommendations derived from the interventions, are summarized in Table 3.
Gaps and Challenges, and Recommendations Derived from the Interventions in the Different Domains
ABOM, American Board of Obesity Medicine; BMI, body mass index; EHR, electronic health record; PROM, patient-reported outcome measure.
Discussion
Obesity is a chronic disease that requires long-term management by a multidisciplinary team. 32 PCPs are the first point of contact for most patients and play a key role in the diagnosis and evaluation of patients with obesity. In addition, they assess risk and determine the presence of obesity-related complications and decide on appropriate management or referral. 33 Despite the essential role of primary care teams in the treatment of patients with obesity and common weight-related complications, the increasing rates of the disease can pose a significant burden at the organizational level in providing evidence-based care because of insufficient resources and training. 2,13 Therefore, HCOs need to develop models for obesity management in the primary care setting.
Many of the gaps and/or challenges identified by the participating HCOs during the development stage were addressed with the primary care initiatives developed under the collaborative. The pragmatic and patient-centered approaches to obesity management that were implemented took into consideration the resources available locally and enabled the development of obesity programs encompassing all 4 care model domains in the framework at each HCO, based on the lessons learned and challenges faced at the individual participating sites. Challenges experienced by one organization do not necessarily apply to another; organizational structure, resources, and culture all can contribute toward the success or failure of an intervention.
OCMC was successful in using a framework and its components to develop a care model that was adapted for local use. Key interventions included the development and organization of quality monitoring systems, training of leadership and staff, and the establishment of community partnerships and effective use of the available resources. The designation of clinical/obesity care management champions and implementation of shared medical appointments (SMAs) were successful approaches that may be replicated effectively in other practices. Some of the physicians in the collaborative became certified through the American Board of Obesity Medicine. One HCO was able to introduce an EHR best practice alert and add obesity to the diagnosis list, and some organizations created effective referral processes to community services and embedded them in the EHRs to track usage.
Community domain
The community initiatives implemented under this collaborative were varied in nature, but commonly addressed nutrition and physical activity. One particularly useful strategy was to embed an HCO staff member on a community board or committee. That enabled alignment between community and health system activities and sharing of initiatives and efforts. To complement in-person activities, which sometimes suffered from low attendance, online activities may be implemented (eg, live cooking sessions broadcast on a social media platform to enable a much wider outreach). In addition to the successful interventions implemented, some groups experienced challenges. For example, one organization wanted to incorporate a list of community resources into the Epic software (Epic Systems, Verona, WI) in a SmartPhrase that could be embedded into the post-visit summary. However, their PCPs were opposed to the idea and preferred a booklet that they could give to the patients. Although the booklet was developed for distribution, substantial time and effort were spent trying to incorporate this material into Epic in terms of navigating institutional committees and securing appropriate approvals. Eventually, the process was defined by having an administrator on the team.
Health care organization domain
Although effective strategies to help patients lose and sustain weight are needed, these cannot be implemented without significant organizational restructuring and robust documentation and tracking systems to accurately measure their impact. Insufficient insurance coverage and difficulties dealing with coding and billing processes for office visits are often reported by providers as key obstacles in the active management and support for patients with obesity in primary care. 13 Some of the initiatives targeting PCPs in this collaborative focused on education about reimbursement options for obesity management, including billing and coding processes, documentation, and referral procedures. Although some organizations experienced success with health care provider education, another organization's initial attempts to engage providers, through multiple delivery methods (ie, written materials, video format, in person), to educate on weight bias, stigma, and effective patient-provider conversations were not as successful. Instead, organizing an in-person educational dinner event produced champions who were interested in obesity care management.
In addition, structural interventions also were beneficial, including outfitting the physical layout of outpatients' venue for patient care (eg, with scales that accommodate patients with severe obesity; reinforced chairs and couches; reinforced exam tables placed lower to the ground for access; private area for taking vital signs, weight, and waist circumference measurements; bathrooms with wide doors and floor-mounted toilets).
Care team domain
Obesity care can be improved by multiple approaches, beginning with staff training and proceeding to the development of tools that facilitate diagnosis and adequate follow-up treatment. 34 The research team observed that it is crucial to engage PCPs in developing and providing tools they consider helpful in the evaluation of patients with obesity in their practices. Both educational interventions for PCPs (in person or online, self-study or guided), 13 and the provision of structured tools for patient evaluation and counseling, 35 are known to significantly increase confidence and self-efficacy for obesity management. In addition, it is important that PCPs and staff engage patients in their treatments in an empathetic and respectful manner. At the care level, SMAs with health care professionals from different specialties, including counseling on nutrition, physical activity, and stress management, can be an effective strategy to address chronic diseases such as obesity. 32 Although an intervention of this type presents demands in terms of logistics and human resources, 32 this approach was followed by one of the HCOs participating in the collaborative, with positive results.
Patients also need to be educated on what constitutes realistic weight loss goals based on the therapeutic options. Information regarding the health benefits that accompany even moderate weight reductions is useful in engaging patient participation in the decision-making process. 32 The level and quality of interactions with PCPs also have an impact on patient participation and adherence to weight-management plans, and organizations should provide tools and clinical pathways to facilitate long-term support by providers. 13 Technological aids, such as electronic reminders that prompt PCPs to collect weight data, can increase documentation of a diagnosis of overweight or obesity, signaling the need for further counseling and evaluation. 13 In this collaborative specifically, the use of smart tools, including best practice alerts, incorporated into EHRs facilitated the diagnosis and process of referral to nutrition or lifestyle coaching and/or weight management services. Developing a multidisciplinary team was identified in the collaborative as an essential intervention in order to provide comprehensive obesity care management. Although some organizations were able to do this successfully, others were limited to 1 or 2 disciplines.
Patient/family domain
Weight bias and stigma can discourage patients from seeking help to manage their weight, hence contributing to reduced quality of life and poor care. 13,36 A considerable amount of bias and stigma were identified by the participating HCOs; mitigation strategies included education on obesity as a chronic disease, as well as sharing patient perspectives from the Obesity Action Coalition. Identifying “patient champions” at each HCO was challenging, but those organizations that did involve patients found the feedback to be invaluable. Additional efforts should be made to include patient and family input on the quality of the care they receive, including clinic design and flow (eg, having a patient walk through the clinic and comment on each step in the process of their care was suggested as way to elicit patient input). One group involved their patients in the development (design and workflow) of their SMAs. The collaborative's HCOs were asked to implement PROM surveys, and many had challenges with the implementation and data collection. For example, some groups experienced challenges with collecting completed surveys from the same patient at different visits; this was important information to gather in order to determine if there were any changes over time.
Strengths and limitations
Strengths of this program include participation from a geographically and structurally diverse group of HCOs serving culturally and demographically diverse patient populations. The organizations represented multispecialty medical groups, integrated delivery systems, and 1 academic medical center; this diversity strengthens the generalizability of the program. All participating HCOs developed interventions within a single predefined framework consisting of 4 domains, creating a consistent array of strategies, at the domain level, implemented across the 10 participating HCOs. The design of the collaborative, with 4 in-person meetings, monthly webinars, site visits, and other touch points, encouraged HCOs to collaborate with and learn from one another. A detailed data specification provided in advance of measure self-reporting ensured comparability of measure performance across HCOs.
One potential weakness of the program was that only very interested and motivated HCOs chose to participate; therefore, generalizability to other HCOs may be limited. Participating organizations were paid a stipend; therefore, while sustainability was encouraged, enthusiasm may have waned after the funding ended. However, all 10 HCOs reported the intention to continue their obesity care programs, and business cases were developed to support sustainability after the close of the collaborative.
Several challenges prevented HCOs from fully implementing many of the interventions recommended. Not all organizations had the resources to implement strategies such as SMAs for patients with obesity or to create a dedicated obesity clinic. HCOs had different relationships with their communities, which created site-specific challenges to coordinating interventions and care with community resources. HCOs also had different organizational structures (ie, some were physician owned), leading to varying levels of interest in a focus on a financial incentive to improved coding. National rates of prescribing anti-obesity medications are low because of cost, lack of coverage by health insurance plans, and other issues, 9,37 making it difficult for HCOs to increase these rates significantly. Overall, sites faced challenges in the recruitment of patients to participate as champions. Importantly, the context of each HCO needs to be considered when developing individual obesity programs at each participating site. Although AMGA provided a framework within which HCOs were expected to develop their programs, it did not dictate the specific interventions each HCO had to implement. Local context, including available resources, organizational structure and culture, and patient population, was the most important predictor of which interventions were successfully adapted and adopted at each HCO, and several interventions rose to the top as universally adopted (Table 3).
In summary, this study identified key aspects and features in the establishment of competent obesity care programs: commitment of the organization and health care professionals, need for resources and programs that enable empowered patients who understand the implications of the disease, and a prepared health care system, with operations and competent professionals to provide comprehensive care, coverage, and access to care, and availability at the organizations of all evidence-based treatment options as well as referral networks.
Conclusions
Obesity care is a challenge in the primary care setting, but with a few key practical interventions, many of which are described in this article, progress can be made to improve patient outcomes. The current evidence-based obesity guidelines recommend screening, and primary care is ideally suited to obtain weight and height measures for determining body mass index and diagnosing obesity, which can be entered into the medical record. The next step consists of the assessment of weight-related complications, and generally is addressed in primary care through the review of systems, the physical exam, and laboratory testing. Treatment for obesity includes choosing a healthy diet and increasing physical activity, which can be facilitated by community partnerships. Finally, use of pharmacotherapy and access to metabolic surgery also are important parts of a comprehensive care plan for patients with obesity.
Although specialty guidelines have been developed for the management of obesity, medical institutions are expected to translate them into real-world treatment strategies, which is not easily done in primary care. In this collaborative, the research team developed an obesity framework at the primary care level, identified important components of and key interventions for the management of obesity, described obesity programs based on these interventions, and translated them into real-world settings. Based on the experiences of the participating HCOs in the collaborative, coordinating care across organizations and specialties is of utmost importance to enable the integration, awareness, and accessibility of evidence-based treatment guidelines.
Footnotes
Authors' Contributions
Ms. Casanova drafted the manuscript and provided final approval for the manuscript. Ms. Casanova, Ms. Chambers, Ms. Leaver-Schmidt, and Dr. Kennedy led the collaborative programming, including content development and implementation, framework and advisory committee development and execution, literature research, planning, framework analysis and interpretation of the qualitative results, and provided critical review and approval for the manuscript. Dr. Ciemins led the measure development and advisory committee, data analysis and interpretation of results, and provided input into the literature research, collaborative programming and implementation, and critical review and approval for the manuscript. Drs. Kushner, Smolarz, and Garvey provided input into development of the framework and measurement approach and implementation, interpretation of the quantitative and qualitative data results, and critical review and approval for the manuscript.
Acknowledgments
The authors would like to thank Joe Nadglowski (Obesity Action Coalition), Deborah B. Horn (University of Texas), Kathleen Morton (Coastal Medical), Paula Burich (Sharp Rees-Stealy Center for Health Management), Doris Boutain (University of Washington School of Nursing), and Senait Temesgen (American Medical Group Association) for their contributions to the conception and design of the program, the care model analysis, and the interpretation of the intervention strategies.
Author Disclosure Statement
Ms. Casanova, Dr. Ciemins, Ms. Chambers, Ms. Leaver-Schmidt, and Dr. Kennedy are employees of the American Medical Group Association. Dr. Kushner is a member of the medical advisory board for Novo Nordisk, Inc., and has received research grants from Novo Nordisk, Inc. Dr. Smolarz is an employee and stockholder of Novo Nordisk, Inc. Dr. Garvey serves as principal investigator for clinical trials sponsored by the University of Alabama at Birmingham and funded by Lexicon Pharmaceuticals, Novo Nordisk, Inc., and Pfizer; and is a consultant to Boehringer Ingelheim, BOYDSense, Jazz Pharmaceuticals, Novo Nordisk, Inc., and the Milken Institute.
Funding Information
This collaborative was funded by Novo Nordisk, Inc. The authors received writing/editorial support provided by Patricia Fonseca, PhD, of Excerpta Medica, funded by Novo Nordisk, Inc.
Supplementary Material
Supplementary Material