
Abstract
Reducing the cost of care while enhancing its quality and experience are essential components to success in value-based care. Because emergency department (ED) and hospital settings represent high-cost environments, the authors sought to reduce their unnecessary use by deploying a novel care delivery service that offers mobile, on-demand care for high-acuity conditions in patient homes. This study is a retrospective quality improvement evaluation of the initial year of the mobile acute care model in a health system with a substantial penetration of value-based care. Although all patients were eligible for mobile services as clinically indicated, those in accountable care organizations were prioritized by the care management teams. A variety of operational, clinical, and financial metrics were assessed to determine the program's performance and value. There were 3436 patient encounters during the study period, a utilization rate of 71% that trended upward throughout the year. Of these visits, 44% involved patients in value-based payment models; 80% of these represented patients in Medicare risk agreements. Throughout the year, progressively improving operational and clinical performance were observed, as were consistently high patient satisfaction scores. An estimated 63.8% of total mobile visits resulted in ED avoidance; 21.6% were emergency medical transport avoidant; 14.1% led to avoided hospital observation or inpatient stays. Patients were highly satisfied with the service. In-home mobile care for high-acuity illness can prevent unnecessary ED and hospital use for some patients and is associated with high patient satisfaction. Acute mobile care is a useful component of a value-based care strategy.
Introduction
Successful value-based health care hinges on the premise that high-quality care should be provided in the most appropriate, lowest cost environment. 1 Hospitals and emergency departments (EDs) are high-cost settings; reducing their unnecessary use is important for accountable care organizations (ACOs) and other risk-bearing entities. 2 As health care in the United States continues its inexorable transition toward a value rather than a volume basis, novel care delivery models that promote improved outcomes, experience, and lower costs are critical.
Annual ED visits continue to increase at a significantly greater rate than would be expected based on population growth in the United States. 3 As many as 30% of ED visits may be non-emergent 4 and thus, likely could be safely managed in urgent or conventional ambulatory care settings. Several factors have been cited as contributing to this overuse of ED resources, including limited access to primary care and behavioral health services, gaps in patient perception and understanding, and social determinants that adversely affect health. 5 Overuse of the ED engenders higher facility (ie, hospital) costs and also is associated with inappropriate use and the related costs of emergency medical transport services (EMS), 6 high ED revisit rates, 7 suboptimal patient experiences, 8 and contributes to overcrowding and delays in patient care. 9 One promising approach to reduce unnecessary ED use and improve value is the delivery of acute care in the patient's home or residence.
The concept that care in the home could successfully address a patient's acute needs – practiced by earlier generations of physicians in the form of house calls 10 – received renewed attention several years ago with the development of “hospital at home” programs. This innovation, focusing on identifying patients with acute conditions that otherwise would require hospital admission who could be managed safely at home, results in improved patient outcomes, satisfaction, and lower costs as compared with traditional hospital care. 11,12 Extending this concept to develop alternatives to the care that patients traditionally seek through the ED, the research team sought to reduce utilization by deploying a novel care delivery service that offers mobile, acute, on-demand, high-acuity diagnostic and therapeutic interventions in patient homes. This article reports the results of the first year of the program.
Methods
Study design
The research team conducted a retrospective quality improvement (QI) evaluation assessing a mobile in-home health care delivery service. This QI work was subject to an Institutional Review Board waiver. This study adheres to SQUIRE 2.0 reporting guidelines.
Study setting
Baystate Health (BH), an integrated delivery system anchored in metropolitan Springfield and serving a population of more than 850,000 people in western Massachusetts, comprises 4 acute care hospitals and an employed, academic provider group of more than 750 physicians and 340 advanced practice providers (APPs). BH operates 2 accountable care organizations (ACOs), one serving 50,000 Medicare beneficiaries and the other serving 38,000 individuals who are insured through the state's Medicaid program. Another 70,000 patients receive their care through other forms of risk-based contracts. Greater Springfield represents one of the poorest areas of Massachusetts; more than 90% of public school students are eligible for reduced or free school lunches, and more than 21% of residents live in poverty. 13
Mobile acute care model
BH partnered with DispatchHealth (Denver, CO) to provide on-demand, high-acuity, in-home medical care to BH patients older than 6 months of age with prioritization given to members of the 2 ACOs and those in other risk contracts. The program launched on November 1, 2018, with 2 vehicles in service 10 hours per day, 7 days per week, servicing the area of metropolitan Springfield, MA with its population of approximately 700,000. The services are designed to substitute for evaluations in the ED and thereby reduce unnecessary ED use, EMS transport, and in some cases, observation and inpatient hospitalizations. The team that arrives in the home comprises an APP and a medical technician and is supported by a board-certified emergency medicine physician available via telemedicine. Vehicles are equipped with a Clinical Laboratory Improvement Amendment-certified point-of-care laboratory, an electrocardiogram, a wide assortment of intravenous (IV) and oral medications, as well as the ability to perform selected procedures such as laceration repair, catheter placement, IV fluid infusion, and incision and drainage of abscesses. Each home visit includes a focused history and exam, a home safety evaluation, and an interview assessment of social determinants that potentially affect the patient's health.
Mobile acute care services can be activated through referrals from ACO care managers – who focus their efforts on high-risk populations that include patients with chronic diseases, primary care teams, home health providers, or senior housing clinicians. Patients are prioritized for the service through a predictive modeling software algorithm that uses a combination of claims, diagnoses, and ED/hospital utilization history to assign them an overall risk score. After referral, the patient is contacted to undergo a triage process, which includes an assessment of medical appropriateness, insurance eligibility, and visit consent. A proprietary triage tool uses retrospective and prospective data to determine whether the patient has a time-sensitive medical complaint. If a determination is made that the patient's condition warrants a mobile visit, the patient is assigned an acuity score that informs her/his priority relative to others in the queue; if triage indicates the patient warrants evaluation in an ED, he/she is navigated to that site of care.
After the mobile visit, the team sends an electronic message to the primary care physician (PCP) or ACO care manager through a secure texting network, allowing for timely follow-up. Additionally, the mobile care team often will call a patient's PCP or care management team while on scene to seek or convey vital historical or clinical information. While on scene, mobile teams are equipped to assist with connecting patients to a PCP if they do not have one. Mobile care teams perform an observation and a structured interview assessment of social factors that affect health at every visit. Within 24 hours of a mobile visit, patient records are shared electronically with the primary care team either through direct secure transfer of clinical notes between electronic health records (EHRs) or through an intermediary such as a local Health Information Exchange. Immediately after the completion of a visit, patients receive a personalized link to a satisfaction survey and also are contacted 3 days later to review their experience and ensure that the care plan is progressing as intended. Providers may request that the 3-day outreach occurs earlier based on clinical concerns or recognition of social challenges that could impede adherence.
Some patients are found to require a higher level of care during on-scene evaluation. In those instances, providers follow internally developed escalation protocols. Based on the severity of the underlying condition, they facilitate transfer of the patient to the ED either by private automobile, non-emergent transport, or rarely, EMS. Providers remain on scene with the patient until the transportation handoff is made. Providers also call ahead to the receiving facility and relay pertinent information from their in-home evaluation.
Based on previous experiences of the mobile service provider, the maximum capacity of visits is 8 patients during a 10-hour shift per vehicle. To account for a ramp-up period influenced by the patient selection strategy, a goal of 65% service utilization, approximately 10 patient visits per day for 2 cars, was set for the initial year of operations.
An executive steering committee, comprising several senior leaders from the health system and from the mobile care partner, provides program oversight and monitors the advancement of its strategy goals on a quarterly basis. A joint operating committee (JOC), comprising operational leaders from both enterprises, is responsible for continuous monitoring of clinical, quality, and financial performance of the program and meets monthly to review all aspects of operations.
Analysis
Several operational, clinical, and financial performance indicators were evaluated to assess the program (Table 1). Service utilization rate refers to the number of completed visits as a proportion of the total vehicle capacity. Wait times represent the total length of time patients waited to receive care after speaking to the call center; on-scene times represent the duration of the actual patient encounter. Documentation rate describes the percentage of visits in which encounter records are conveyed electronically to the primary care team.
Key Performance Indicators Used to Assess the Mobile Acute Care at Home Program
ED, emergency department; EMS, emergency medical transport services.
Escalation rates are defined as the percentage of patients escalated to the ED. Escalation can occur at the time of telephone triage by the mobile care team or at the time of the visit. Revisit rate, defined as the proportion of patients who sought ED-level of care 3, 14, and 30 days after a mobile visit for the same or a related complaint, was determined from reviews of the EHR and direct outreach for every patient. Net Promoter Score (NPS) is a widely used measure of consumer loyalty and, in health care, is a surrogate for patient satisfaction. 14 Patients seen by the mobile care teams are surveyed after the visit to determine their likelihood of recommending the service to others using a scale of 0 to 10. Scores of 9 or 10 are considered promoters and scores of 6 or below are considered detractors. Scores of 7 or 8 are considered neutral and included in the total number of survey responses. NPS is the difference between the percentage of promoters (based on the total number of survey responses) and the percentage of detractors and is reported as a whole number in the range between -100 (if all respondents were detractors) to 100 (if all were promoters). Regional rates of social determinants that affect health were compared to national ones using Z-tests.
A multivariable model was used to estimate the likelihood that a home visit prevented higher levels of utilization. Variables used in the model include place of service (eg, home, skilled nursing facility, senior community), time of call, homebound status, disease severity, procedures performed, vitals on scene, and the results of a self-reported patient or family survey indicating where care would have been sought in the absence of the in-home visit. The model predicted the number of patients treated in the home who avoided EMS transport, an ED visit, hospital observation, or inpatient admission. The number of patients for each avoidance type was stratified by payer population and then multiplied by the average cost for the respective level of care that was avoided. Cost data were provided by the BH ACOs, based on an analysis of historical claims data for each of their value-based programs. Revisit patients were removed from the estimated savings model. Total medical cost savings represents the weighted average of each diversion type across all relevant payer populations.
Results
Overall, there were 3436 patient encounters between November 1, 2018, and October 31, 2019. Based on a maximum daily utilization of 16 visits for 2 vehicles, this equated to a utilization level of 71% during the study period, trending upward every quarter (Fig. 1) and exceeding the first-year goal. Most requests for mobile care occurred on Mondays and Fridays; weekend use tended to be 20%-30% lower than during the week, although this increased in the fourth quarter because of focused efforts to enhance weekend use. Visit requests tended to peak between 1000–1200 hours each day and declined after 1400 hours.
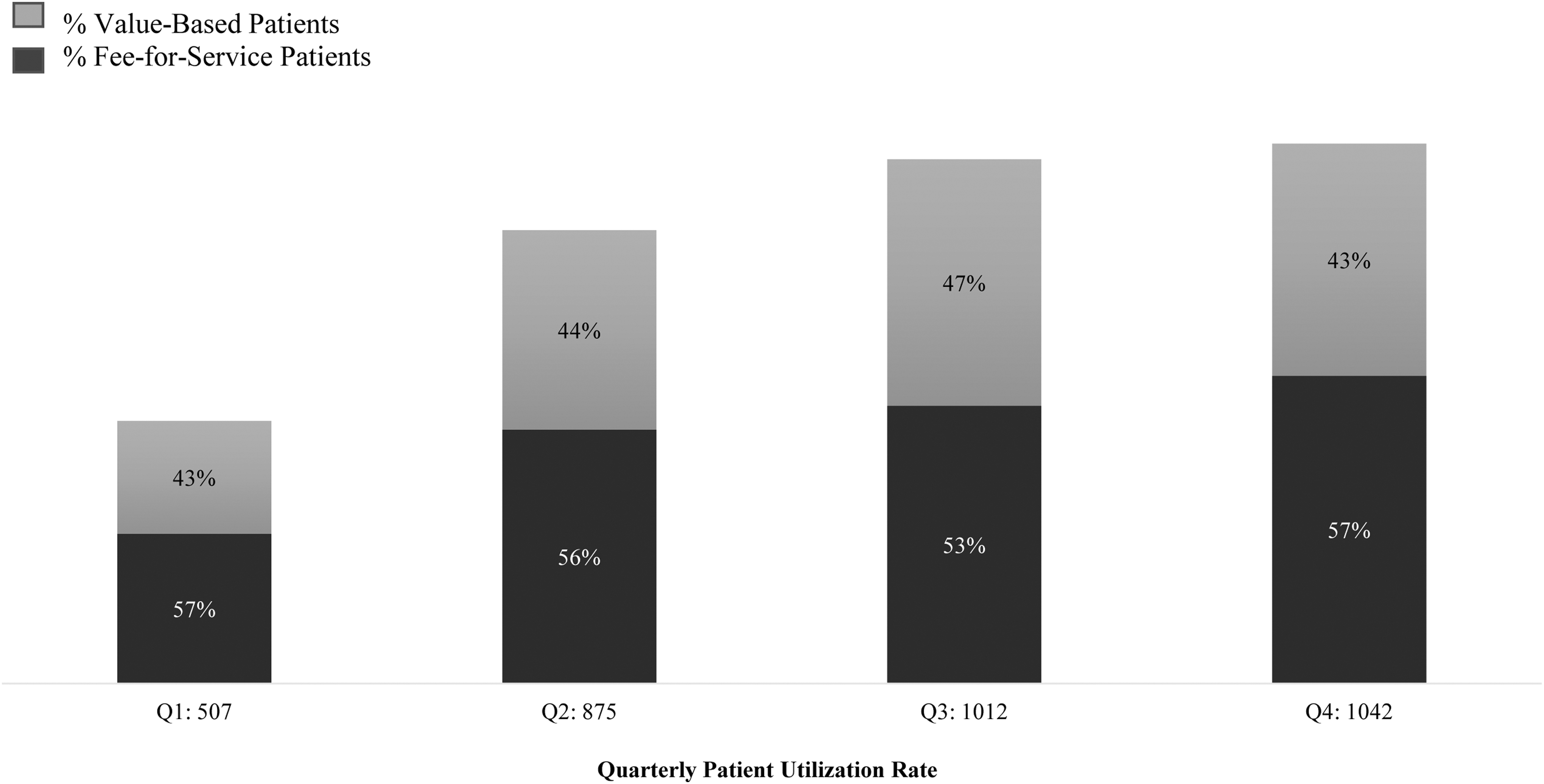
Acute mobile care service patient volumes and proportion of those in value-based payment agreements.
Forty-four percent of patient encounters were patients in value-based payment programs (Figure 1); approximately 80% of those, or 35% of the total visits, were participants in either Medicare Next-Generation ACO or Medicare Advantage plans. Nearly two thirds of the remaining visits (representing 35% of the total mobile visits) involved patients covered by a traditional Medicare plan. The other, non-Medicare patients in risk-based arrangements who received mobile visits were participants in commercial risk contracts or in the Medicaid ACO. During the first part of the launch year, most referrals for service came from 3 distinct sources: members of the primary care team, ACO care managers, or senior care facilities. As care management teams educated patients, greater numbers of clinically high-risk patients or their families subsequently requested mobile care directly. Throughout the year, on-scene times declined from 56.6 minutes to 39.5 minutes. However, wait times increased from 115.8 minutes in the first quarter of the year to 204.5 minutes in the final quarter, an increase of 88.7 minutes. NPS was 94.5 for all patients and 96 for those in value-based programs.
The conditions encountered most frequently are shown in Table 2, with urinary tract infection, cellulitis, and acute respiratory infections, including pneumonia, accounting for more than half (54%) of the diagnoses. Acute exacerbations of chronic obstructive pulmonary disease (7%) and systolic heart failure (9%) accounted for 16% of the referrals in the first year of the program. More than 75% of the procedures performed by mobile care teams in the first year of service represented laboratory testing; another 15% were therapeutic interventions, including infusions of IV fluids or antimicrobials.
Breakdown of Mobile Visit Diagnoses
For patients in value-based programs with established PCPs, mobile visit records were shared with the patient's care team 95.1% of the time; the rate was 80.7% for the entire population of mobile visits. Escalation rates were 11% at initial phone triage and 8.7% on scene. In surveying for social determinants that affect health, nearly 30% of patients lacked access to transportation, patients averaged more than 11 prescription medications, and nearly 5% of patients said they could not afford their medications. Revisit rates for all mobile acute care patients were 6.6% at day 3; 11.9% at day 14; and 13% at day 30. Rates for patients in value-based programs were similar to those of the entire group.
The research team estimates that the mobile acute care service realized 2192 ED diversions, equivalent to 63.8% of all completed home visits during its initial year. Additionally, 21.6% of all visits were categorized as an avoidance of EMS transport and its associated cost. Through deployment of mobile acute care in the home, 399 (11.6%) and 86 (2.5%) patient visits were considered an avoided observation or inpatient hospitalization, respectively. When evaluating only services provided to members in a value-based program, 330 patients (21.8%) avoided EMS transport, 1058 (70%) avoided an ED visit, 178 (11.8%) avoided an observation stay, and 40 (2.6%) avoided an inpatient admission.
Discussion
This study reports on a novel intervention aimed at reducing ED and hospital use by providing mobile acute care in patient homes. Analysis of the first year of the program demonstrates the intervention to be feasible, highly satisfying to patients, and to have achieved its goals with respect to providing value to patients and the health system.
BH health system, an integrated delivery network comprising hospitals, a home health agency, a network of employed and community providers, and a fully owned health plan, has been active in value-based care with multiple shared risk contracts for more than a decade. Despite the relative success of the population health programs in promoting value, BH recognized gaps in the acute care needs of the highest risk patients. Because of their high prevalence of medical complexity, frailty, decreased mobility, social isolation, and transportation limitations, members of the BH Medicare population with acute needs often seek care in the ED in the absence of more accessible alternatives. Thus, delivering clinical services to them through mobile acute care in their homes filled an unmet need in the BH value-based delivery system, as evidenced by the high utilization rate in this population: 70% of the total visits were made to Medicare patients, divided nearly evenly among patients in value-based and in traditional fee-for-service plans.
Creating a culture of collaborative, clinical integration between the provider teams of the health system and those of the mobile acute care service was critical to the success of the program. To nurture trust among the teams, mobile care clinicians spent time on-site prior to implementation, reviewing organizational performance data, conducting stakeholder (ie, PCPs, specialty providers, care managers, home health team members) interviews and shadowing. Mobile care workflows, supporting materials, and stakeholder education were designed subsequently with a focus on integrating the service into the health system's extant practices to optimize value. Primary care and care management teams introduced the concept of mobile acute care to their high-risk patients as a practice extension, which helped patients and their families feel more comfortable allowing these new providers into their homes.
Pre-implementation collaborative efforts facilitated a relatively seamless clinical integration of mobile acute care services into the delivery model, allowing those clinicians who often were in daily contact with the highest risk patients to connect them with these services and ensured both the most appropriate use of mobile care and the optimal transition back to the longitudinal care teams following a visit. Real-time communication between the mobile and longitudinal care teams was reliable, with >95% of mobile visit clinical notes conveyed to the patient's EHR within 24 hours of the visit. To ensure that the mobile integrated acute care service optimized value and to limit its use for patients who could be better managed in lower acuity settings (eg, urgent care, primary care), marketing was limited to high-risk patients (ie, medically complex, in value-based management, those with mobility or transportation issues), PCP and specialty providers, care managers, home health agencies, and preferred assisted living facilities, instead of a broader, consumer-directed marketing initiative.
The research team believes that the rapid ramp-up of use of the mobile acute care service to more than 70% in the initial year affirms several themes: the service addressed an unmet need in the population; patients enthusiastically embraced the model of care delivery; and the implementation strategy was successful. Use continued to rise over the course of the year, and weekend use improved. Nearly three quarters of mobile visits were for serious, acute clinical issues or for acute exacerbations of chronic medical illnesses. Patient satisfaction was nearly universal. NPS of >95 overall compares quite favorably with a recently cited NPS industry standard for health care providers of 9. 14 The 30% decline in on-scene visit times over the course of the year likely was a function of mobile provider team maturation and growing comfort with the integrated workflows developed with all stakeholder teams. However, as demand for mobile services rose steadily throughout the year and delivery capacity remained fixed based on 2 vehicles, a 76% increase in wait times was observed. Increasing capacity is expected as the program evolves.
Escalation rates in the BH market were found to be higher than others nationally: 11% vs. 9.5% for phone escalation (P < 0.002), and 8.7% vs. 6% for escalation on scene (P < 0.00001). The team believes these differences can largely be explained by the medical and social complexity of these patients in a highly vulnerable region, 13 and this is supported by the results of screening for social determinants affecting health during the mobile encounter. Nearly 30% of BH patients, as compared with 9.3% nationally, lacked access to transportation (P < 0.00001). Additionally, BH patients averaged more than 11 prescription medications each, placing them in the top half of other mobile acute care markets, and nearly 5% of patients said they could not afford their medications compared with 1.3% of those nationally (P < 0.00001).
Overall, the first year of the mobile acute care program achieved its intended objectives of managing high-risk patients in a lower cost setting. Based on more than 1500 encounters for patients in value-based programs, the net cost savings for year 1 of the mobile acute care at home program was estimated to be $968,542. This is based on an estimated savings of $1729 per visit, using the aforementioned methodology, with costs applied across each avoidance type (ie, ED, EMS, hospitalization) based on risk contracts. The net savings represents a return on investment of 1.58.
Several challenges were encountered in the implementation and operations of mobile acute care services. Because the focus was on treating medically and socially complex patients in the home, the number of daily mobile visits varied, based on both patient acuity level and logistics, such as the drive time between visit locations. These factors may impact efficiency levels, which must be weighed against the program's strategic goals. The choice was made to sacrifice some level of operational efficiency to reduce unnecessary, high-cost ED, EMS transport, and/or hospital utilization, especially in those patients in value-based care models. In a pure fee-for-service payment model, the cost/benefit calculus may be different. Integrating the primary care and mobile provider EHR was an ongoing challenge throughout the initial program year. Mobile care providers placed an emphasis on secure texting platforms during this transition period to ensure timely communication of clinical data. Finally, because the mobile care service was prioritized for patients in value-based plans, daily capacity challenges progressively affected operations as the demand increased over the course of the year among all patient groups. These issues were able to be managed successfully to a degree through the telephone triage process but will require expanding capacity as the program evolves.
Adding mobile acute care services to the BH portfolio of population health management tools appears to have achieved the goals of reducing unnecessary utilization, medical cost reduction, and demonstrating exceptional patient satisfaction. As the program matures, the organization continues to seek ways to improve operational and financial performance and to increase capacity and geographic reach of the service. Planning also is underway to expand mobile care initiatives to other patient populations in the community, such as hospice, behavioral health, rural communities, and COVID-19-infected individuals as BH continually seeks to optimize value.
Footnotes
Authors' Contributions
Dr. Artenstein: conceptualization, investigation, writing–original draft, supervision. Mr. Stanaway: methodology, investigation, writing–review and editing, project administration. Ms. Roy: methodology, investigation, writing–review and editing. Dr. Westafer: methodology, writing–review and editing. Dr. Lindenauer: methodology, writing–review and editing. Dr. Seiler: methodology, investigation, writing–review and editing. Ms. Coelho: formal analysis, writing–review and editing. Dr. Prather: conceptualization, methodology, writing–review and editing, supervision.
Author Disclosure Statement
Dr. Prather reports an ownership interest in DispatchHealth. The remaining authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.