
Abstract
Collaboration among diverse stakeholders involved in the value transformation of health care requires consistent use of terminology. The objective of this study was to reach consensus definitions for the terms value-based care, value-based payment, and population health. A modified Delphi process was conducted from February 2017 to July 2017. An in-person panel meeting was followed by 3 rounds of surveys. Panelists anonymously rated individual components of definitions and full definitions on a 9-point Likert scale. Definitions were modified in an iterative process based on results of each survey round. Participants were a panel of 18 national leaders representing population health, health care delivery, academic medicine, payers, patient advocacy, and health care foundations. Main measures were survey ratings of definition components and definitions. At the conclusion of round 3, consensus was reached on the following definition for value-based payment, with 13 of 18 panelists (72.2%) assigning a high rating (7– 9) and 1 of 18 (5.6%) assigning a low rating (1–3): “Value-based payment aligns reimbursement with achievement of value-based care (health outcomes/cost) in a defined population with providers held accountable for achieving financial goals and health outcomes. Value-based payment encourages optimal care delivery, including coordination across healthcare disciplines and between the health care system and community resources, to improve health outcomes, for both individuals and populations.” The iterative process elucidated specific areas of agreement and disagreement for value-based care and population health but did not reach consensus. Policy makers cannot assume uniform interpretation of other concepts underlying health care reform efforts.
Introduction
The 21st
This new orientation has been described variously as value in health care, 10 value-based programs, 7 value-based transformation, 11 and transformational shift from volume to value. 12 Terms such as value-based care and value-based payment (or purchasing) 7,13 have arisen as descriptors of the different roles stakeholders play. Achievement of the value-based transformation of health care requires a common understanding between practicing clinicians, health system leaders, and payers regarding how value is defined and measured for purposes of value-based reimbursement. Additionally, public health experts and policy makers must share a common understanding of these terms with those who deliver and pay for health care. The patient's perspective on value also is needed to create a common understanding among stakeholders. 14
The Institute of Medicine (IOM) Roundtable on Value & Science-Driven Health Care reported that value may be understood differently by different stakeholders. 15 Value in health care is often tied to the concept of population health, 7,9,13,16,17 which raises further uncertainty about terminology. The term population health now frequently has a broader meaning than it did in 2003 when Kindig and Stoddard proposed their well-known definition, “The health outcomes of a group of individuals including the distribution of such outcomes within the group.” 18 Kindig has written that the concept is now being applied to the health of patients receiving care in a particular health care organization and that related terms such as population health management and population medicine have thus emerged. 19 A 2014 IHI blog post differentiated population management (managing and paying for health care services for a defined population) from population health (which addresses broader determinants of health) and proposed the phrase population medicine as the best expression of how the resources of a health care system can be used to achieve the Triple Aim. 20 The IOM's Roundtable on Population Health explicitly acknowledges the lack of a commonly held definition of population health. 21 Without a common understanding of terminology, the risk of miscommunication and misaligned endeavors decreases the likelihood of effective transformation.
The Delphi process is a systematic, structured, consensus-forming method using recognized experts who represent different perspectives relevant to the question posed. 22 –24 This method has been used to develop medical appropriateness criteria, clinical guidelines, and to create taxonomies and definitions in the field of medicine. 25 –31 The objective of this study is to use a modified Delphi process to develop practical, broadly applicable definitions for the terms value-based care, value-based payment, population health, and population medicine.
Methods
Study design and population
A Delphi panel of national leaders was formed representing diversity in geographic location, sex, work setting, and professional perspective. An in-person meeting was followed by 3 rounds of structured surveys. A scoping review of definitions in the literature for the relevant terms was provided to the Delphi panel prior to the in-person meeting and informed the content of the first survey round (Supplementary Data). The goal of the in-person meeting was to provide a study overview and generate ideas for definitions and definition components. The discussion was audio-recorded and transcribed verbatim.
Survey content and measures
Each survey round included candidate definitions and definition components to be rated by the panelists. The Round 1 survey used definitions and components obtained from previously conducted scoping reviews (Table 1, Supplementary Table S1, Supplementary Materials Scoping Review). Definitions and components were modified in subsequent rounds based on survey responses. Panelists were asked (1) to rate how well statements defined each term on a scale from 1 (Not at all) to 9 (Extremely well), and (2) how essential components (words/phrases) would be in a definition, on a scale of 1 (Not at all) to 9 (Extremely essential), and to provide persuasive comments to support their ratings. Following Rounds 1 and 2, the panelists received a report with their individual ratings and aggregated ratings and comments from the panel. Panelists were encouraged to modify ratings in response to each summary report throughout the 3 survey rounds, with Round 3 considered to be the final results. The study was approved with exempt status by the University of Pennsylvania Institutional Review Board.
Delphi Survey Definitions and Ratings for Value-Based Care
Data management and statistical analysis
Survey data were managed using REDCap electronic data capture tools hosted at the University of Pennsylvania. 32 Drawing on Rand methodology, 22,23 the study team defined consensus on a definition or definition component a priori as selection by 70% or more of respondents with a rating of 7 to 9 and selection by less than 15% with a rating of 1 to 3. A rating of 7–9 by a panelist is considered an endorsement of the definition or definition component, regardless of the number of 1–3 ratings. Panelists were offered $2000 in compensation for their time at the completion of the study.
Role of funding source
The study was funded by Humana Inc. The Humana project team also provided feedback to investigators at the University of Pennsylvania on the study's design, conduct, and reporting.
Results
Panel participants
Of 21 persons invited, 3 declined, citing conflicts, and 18 either agreed or recommended another leader in their organization. The final panel included 18 leaders who represented diversity of geography, sex, professional perspective, and training (Figure 1). The rate of survey return for each of the 3 survey rounds was 100%.
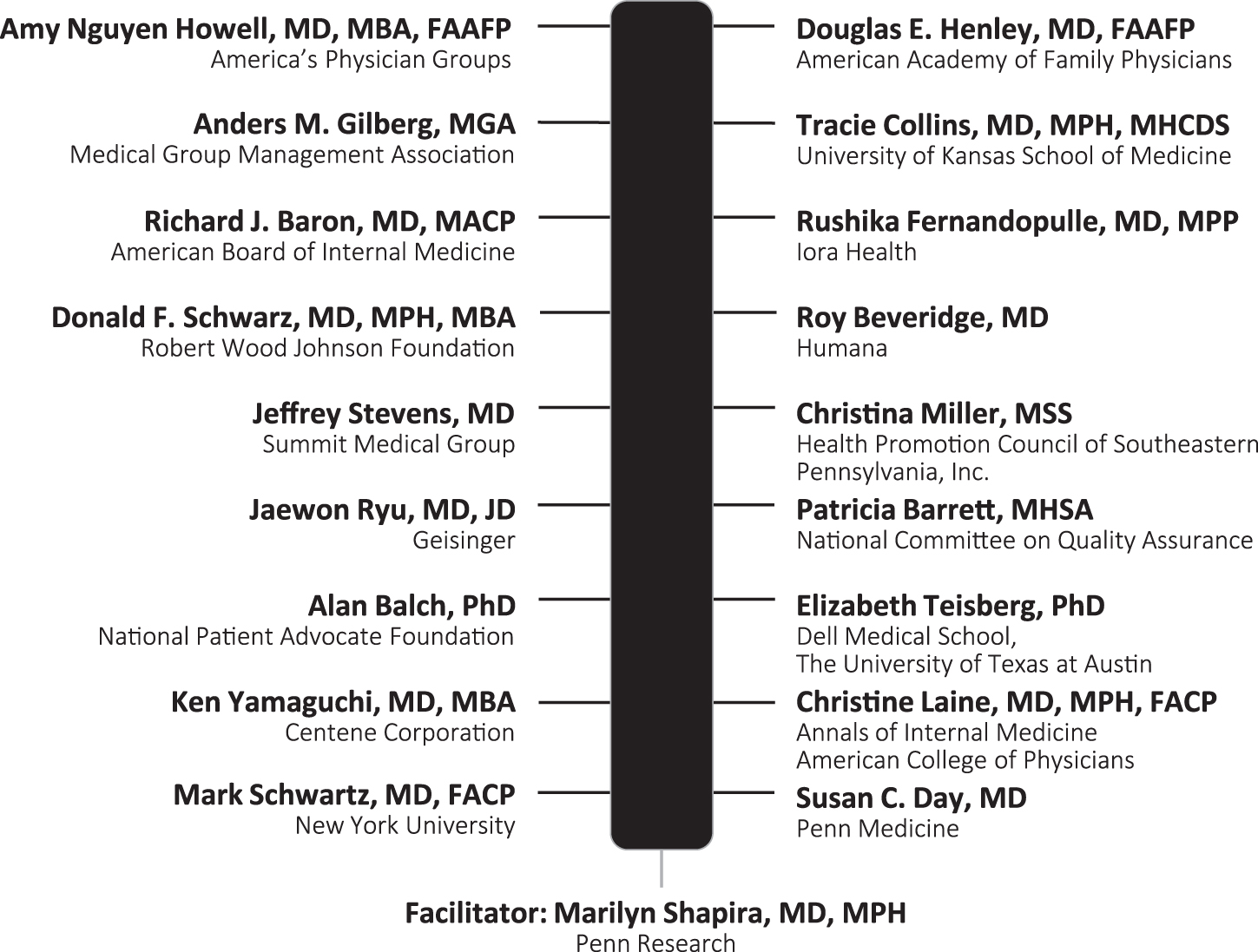
Names and affiliations of Delphi panelists.
Delphi process results for value-based care
At the in-person meeting, panelists agreed that value-based care should emphasize value for the patient and incorporate an aspirational goal of improving health. In Round 1, the following definition met a priori criteria for consensus with 13 of 18 (72.2%) panelists providing a rating of 7–9 and 0 panelists providing a rating of 1–3 (Table 1):
In value-based care, achieving high value for patients must become the overarching goal of health care delivery, with value defined as the health outcomes achieved per dollar spent.
In Round 2 this definition no longer met consensus criteria. Panelists commented that the focus of value-based care should expand to individuals (or patients) and populations with ratings for the components Improve the health of patients and Improving the health of individuals and populations meeting the consensus threshold for being essential to the definition of value-based care. The study team further evaluated components pertaining to the numerator and denominator of a value equation. Support was greater for health outcomes than for health benefits for use in the numerator of the value equation. Including the Patient experience, Preference-aligned patient decisions, or What matters most to patients failed to gain consensus support. The panelists preferred cost vs. dollars spent as the denominator of the value equation with some commenting on the importance of indirect costs such as lost work time, income loss, adverse outcomes, and emotional stress as important to the value equation (Supplementary Table S1).
The concept that value-based care occurs within the constraints of available resources emerged from the in-person meeting. However, when evaluated as a definition component in Rounds 2 and 3, the phrase had limited support. One panelist noted, “… including this phrase in the definition almost sounds like a cop-out.”
The inclusion of a time horizon over which value-based care is provided and measured was raised at the in-person meeting. However, consensus was not reached on components that conveyed this idea. Panelists commented that the reference to a time frame was too ambiguous and that value can be measured over various time frames.
At the end of Round 3, the 2 definitions with greatest support (endorsed by 50% of panelists) included the components Achieving (or improving) the health of both individuals and populations and Defining value as a measurable health outcome per (or relative to) cost of care (Table 1).
Delphi process results for value-based payment
At the in-person meeting, panelists indicated that a goal of value-based payment was to support and/or align with the provision of value-based care and reached consensus in Rounds 1 and 2 that a “definition of value” be embedded within the definition of value-based payment (Table 2, Supplementary Table S2). Ratings for the definition components of Accountability (Round 1) and Accountability of provider for goals/outcomes/metrics (Round 2) approached or met a priori criteria for consensus criteria. In contrast, there was limited support for the terms Reaching quality targets, Utilization measures, Performance measures, Financial incentives for health care providers, and Incorporating risk sharing.
Delphi Survey Definitions and Ratings for Value-Based Payment
In the in-person meeting, panelists voiced that a population health perspective was essential to the definition of value-based payment. In the surveys, panelists supported the definition components Focus on population health and Population-level outcomes with ratings that met or approached consensus criteria, respectively. In contrast, the terms Lowering costs per capita and Increasing capacity to care for more patients had limited support.
During the in-person meeting, panelists discussed the importance of coordinating across health care settings and partnering with organizations outside the health care system to achieving the goals of value-based payment. In Round 3, ratings for a component with the phrase “coordination across health care disciplines and between the health care system and community resources” approached consensus criteria with 7–9 ratings by 12 out of 18 (66.7%) panelists.
At the end of Round 3, the Delphi panel reached consensus (13 out of 18 [72.2%] rating 7–9 and only 1 [5.6%] rating 1–3) on the following definition of value-based payment:
Value-based payment aligns reimbursement with achievement of value-based care (health outcomes/cost) in a defined population with providers held accountable for achieving financial goals and health outcomes. Value-based payment encourages optimal care delivery, including coordination across health care disciplines and between the health care system and community resources, to improve health outcomes for both individuals and populations.
Comments in the Round 3 survey included suggestions to refine the consensus definition by shortening the definition and using the term payment in place of reimbursement.
Delphi process results for population health
The Delphi panel did not reach consensus on a definition of population health but results identified key areas of agreement and disagreement (Table 3, Supplementary Table S3). At the in-person meeting, panelists recognized that a population denominator can be determined in many ways and that health includes many measurable domains. However, the panel did not endorse including detail on these elements in the definition.
Delphi Survey Definitions and Ratings for Population Health
The panel endorsed the component, A range of determinants such as social determinants (education, housing, environmental safety, food), genetic makeup, health behaviors, and access to care as essential to the definition of population health. However, definitions with a reference to determinants of health did not receive consensus ratings. One panelist commented, “Social determinants too often means ‘Not my job.’” Other arguments centered on the appropriate scope of the definition; for example, “The determinants are ‘causes’ while the health outcomes are, to me, the thing itself.”
Ratings for the phrases Reducing disparities and Increasing equity of health approached consensus criteria in Round 1. However, definitions evaluated (Rounds 1 and 2) that included disparities as a measure of population health had limited support. One panelist commented that “To me, the reduction of health disparities is more appropriately included in a definition of population health management rather than a definition of population health.”
In comments from Round 3, a panelist noted the challenge of defining population health as a construct distinct from population health management stating, that “…‘Population Health’…typically has a modifier ‘Population Health Management’ or context (improving the health of the population) in which it is being asked about so trying to reach consensus on what it means alone is tough.”
A summary of areas of agreement and disagreement that emerged from the Delphi process across all 3 terms is presented in Table 4.
Summary of Areas of Agreement and Disagreement *
Reflects both the components that were explicitly rated and ideas that emerged in discussion or as written comments.
Discussion
The terms value-based care, value-based payment, and population health have gained resonance among stakeholders pursuing the goals articulated by the IHI and implicitly endorsed by CMS: improving the patient experience, controlling health care costs, and improving the health of populations. 7,9 Health policies and care delivery innovations designed around these concepts are changing the way we evaluate and pay for health care. However, despite their widespread use, the terms lack consensus definitions. The willingness of 18 high-level leaders to participate in this Delphi study is one indication of the widespread recognition of this risk. This study is the first to use a formal consensus process to attempt to create definitions for the related terms of value-based care, value-based payment, and population health.
Through a modified Delphi process the panel came to consensus on a definition for value-based payment but not for value-base care or population health. Collective ratings and comments show where there is a common understanding across stakeholders and where issues of controversy and confusion remain. The panel agreed that a definition of value-based care should reflect the aspirational goal of improving health in patients and among populations.
The panelists differed on whether the definition should reflect the patient perspective on outcomes. Although panelists agreed on the goal of value to patients, they recognized that what patients identify as important may differ from the clinician perspective or from evidence-based practice measures, as reflected broadly in discussions on value-base care. 14,29,33 The panel was divided on using phrases such as patient experience and patient-centered outcomes in the definition. Response to defining value-based care, as well as population health, in terms of functional status and quality of life were mixed. Patient-reported outcomes and values are not uniformly captured in electronic health records or included in insurance claims. 8,29 If the efforts of payers, clinicians, and other health care stakeholders are to be reoriented to broader measures of health, current data systems are not adequate. The denominator of value (cost) also was viewed by most panelists from a broad perspective. Public and private payers cannot assume that the direct costs of health care are all that matter to other stakeholders.
Finally, lack of agreement on the time frame of value measurement hindered consensus on a definition of value-based care. Objections stemmed from difficulties in describing this component unambiguously and differences of opinion on the most appropriate measurement interval. If those who provide and pay for health care do not have the same time frame in mind, efforts to improve care at the delivery level will not be consistent with policies.
In contrast to the results for value-based care, consensus on the related term of value-based payment was achieved, with broad agreement that value-based payment must align with the achievement of value-based care. Support for the phrase Coordination across health care disciplines and between the health care system and community resources is a key finding. Some panelists commented that addressing social determinants of health was not the direct responsibility of health care providers but the panel's endorsement of language about partnerships recognizes that modifiable upstream causes of disparities in health must ultimately be addressed for population health to improve. 34 It may be that consensus on value-based payment was easier than on value-based care because value-based-payment is a concrete, transactional term that describes more familiar experiences. Additionally, the health care system has moved more quickly in transforming payment arrangements than in transforming the way care is provided. 4,6,7,35,36
The obstacles to consensus for the term population health highlight the multiple uses of this term in today's health care policy discussions. 37,38 A particular challenge was reaching a balance between a concise definition and one that incorporates the complexities of the construct, a challenge that previous Delphi panels and other efforts to clarify definitions also have faced. 25,39,40 Panelists differed on whether the definition should include determinants and outcomes of health or focus on the measurement of health indicators in a population. Lack of a consensus definition may pose a barrier to value-based reform because population health is a central component of both value-based care and value-based payment initiatives. 10
The consensus definition used for value-based payment refers to the concepts of value-based care and population health in broadly agreed-upon terms. It is encouraging that the panel did agree on several aspects of value-based care and the core concept behind population health (see Table 4), although the panel was unable to agree on specific definitions for these 2 terms. The lack of consensus on definitions for value-based care and population health as stand-alone terms may reflect the need for definitions to be specific to a given context, considering the community, population, and health care setting in which health care is being delivered and the perspectives of the stakeholders involved. The goal of this Delphi process was to develop functional definitions that could be implemented operationally. The challenge remains to develop functional definitions that all stakeholders can agree on. If leaders can focus on the areas of agreement while keeping differences in mind, a common understanding of the terms may evolve over time. In the interim, it may be of value for organizations to develop internal definitions of value-based care and population health and to strive for more clarity in external partnerships. A related challenge is to craft definitions that are meaningful and clear to patients but also true to clinicians' and other stakeholders' knowledge about effective care. This will be an important process for policy makers to track; understanding the variety of perspectives on value-based care and population health appears critical.
This study has some limitations. First, the goals were to create concise and broadly applicable definitions. Yet these terms each reflected complex constructs and reaching agreement through such a structured process as the Delphi method felt too restrictive to some panelists. Second, the panel may not have captured all relevant stakeholders. Patients were not on the panel although patient and community advocacy organizations were represented. The panel also lacked participants from government because of potential conflicts of interest between government positions and the Delphi process, which asks for individual judgments based on the sum of an individual's professional experience. Strengths of the process included the diversity among panelists in geography and sex, incorporation of an in-person meeting and 3 rounds of ratings, a 100% participation rate on each survey round, and the use of strict a priori criteria for consensus.
In summary, this study was successful in developing a definition for value-based payment that had consensus among a group of experts representing multiple health care sectors. This definition incorporates concepts of value-based care and population health, which validates the goal of seeking definitions for all 3 terms in one study. The panel's inability to reach consensus for the terms value-based care and population health highlights the challenge of agreeing on practical yet sufficiently rich definitions that can further the cause of health care reform. Policy makers cannot assume that there is a uniform interpretation of the concepts behind value-based health care or population health. Efforts must continue to develop a shared understanding of the meaning of and relationship between these terms so that patients, clinicians, health care systems, payers, and other stakeholders actually achieve health care reform.
Footnotes
Acknowledgments
The authors wish to thank Laura Happe, PharmD, MPH for her conception of the Delphi method as a way to address the problem of unclear definitions. The authors also thank the Delphi Project Management Team (Courtney Brown, PharmD, Deborah Lawson, Teresa L. Rogstad, MPH) at Humana for execution of the scoping review for value-based care and value-based payment, for editorial and copyediting assistance, and for medical writer support. The contents of this manuscript do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Author Disclosure Statement
Additional affiliations for the authors are as follows. Dr.Meredith Williams works for the Southern Emergency Medical Specialists as an attending physician and is paid for the direct care of patients in an emergency department. Dr. Fernandopulle is a shareholder, co-founder and CEO of Iora Health, a value-based primary care group. Dr. Schapira is an investigator at the CMC VA Medical Center in Philadelphia, PA. The other authors declare no conflicts of interest.
Funding Information
Financial support for this work was received from Humana Inc.
Supplementary Materials
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.