
Abstract
Patient navigation has been proposed to combat cancer disparities in vulnerable populations. Vulnerable populations often have poorer cancer outcomes and lower levels of screening, adherence, and treatment. Navigation has been studied in various cancers, but few studies have assessed navigation in lung cancer. Additionally, there is a lack of consistency in metrics to assess the quality of navigation programs. The authors conducted a systematic review of published cancer screening studies to identify quality metrics used in navigation programs, as well as to recommend standardized metrics to define excellence in lung cancer navigation. The authors included 26 studies evaluating navigation metrics in breast, cervical, colorectal, prostate, and lung cancer. After reviewing the literature, the authors propose the following navigation metrics for lung cancer screening programs: (1) screening rate, (2) compliance with follow-up, (3) time to treatment initiation, (4) patient satisfaction, (5) quality of life, (6) biopsy complications, and (7) cultural competency.
Introduction
Vulnerable populations experience disparities in health care and health outcomes. Vulnerable populations are defined as a disadvantaged subset of the community. Although traditionally these subsets have included racial or ethnic minorities, socioeconomically disadvantaged individuals, uninsured/underinsured persons, children, and the elderly, more recent literature recognizes previously overlooked groups such as veterans, immigrants, prisoners, residents of rural communities, and trans/gender nonconforming persons. 1,2
These vulnerable populations experience disparate health care access and health outcomes because of inequalities in social determinants of health. 1,2 In terms of outcomes in cancer care, disparities in time to diagnosis, curative treatment, and cancer-specific and overall mortality have been noted among black, Hispanic, and Asian patients with nearly every tumor type. 3 Despite some racial groups being at high risk, it is important to note that not every individual in a racial minority is vulnerable. Social disadvantage is determined by whether the group as a whole is less advantaged than whites. 4 For example, indices of low socioeconomic status and low health literacy have been associated with increased cancer incidence and cancer mortality. 5,6
Ongoing efforts to reduce cancer disparities in vulnerable populations include both large-scale changes in health care policy, as well as changes at the individual hospital system level as exemplified by the transitioning to a patient-centered service delivery model through the use of patient navigation. This review will focus on identifying metrics that measure the impact of patient navigation on improving care, specifically for patients at risk for or who are diagnosed with lung cancer.
Patient navigators have been proposed as a mechanism to maximize compliance with complex screening programs for cancer. Although navigation has been discussed in the literature frequently, there is a lack of consistency regarding the definition and role of navigators. Merriam-Webster's dictionary defines navigation as “mak[ing] one's way through.” 7 Navigation aims to guide patients through the cancer care continuum to survivorship with preserved health. One literature review states that a navigator is “someone who helps assist patients overcome barriers to care.” 8,9 A navigator's goal is to help cancer patients prevail over hurdles to early and effective diagnosis and treatment. 9,10
In order to guide patients through early cancer detection and the cancer care continuum, patient navigation consists of 3 main phases: (1) navigation to screening, (2) navigation to diagnostic evaluation, and (3) navigation to treatment. Patient navigators should provide culturally competent care and aim to boost patient satisfaction throughout all 3 phases of navigation (Figure 1 illustrates the process steps).
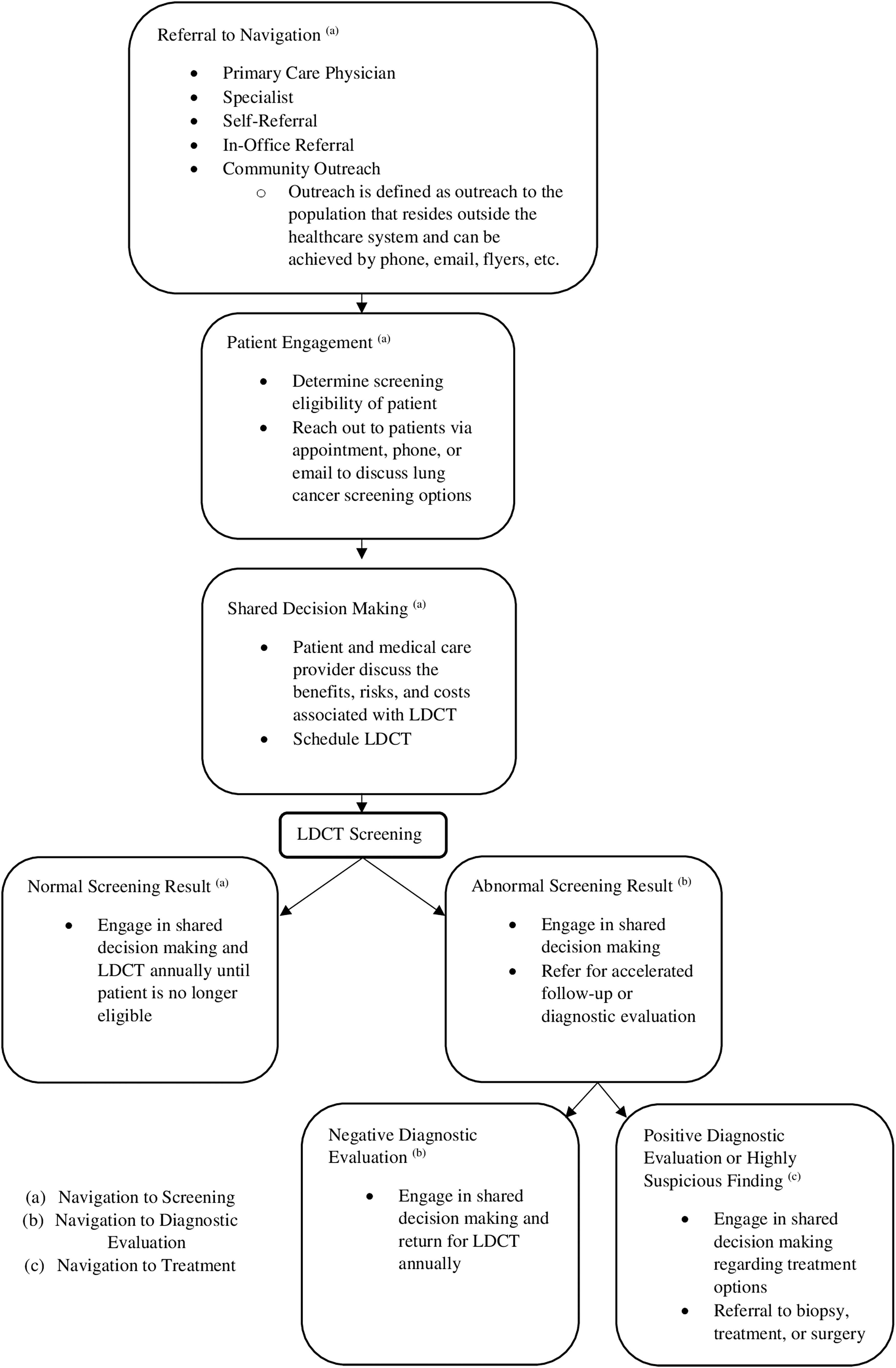
A flowchart illustrating the 3 phases of the navigation process. LDCT, low-dose computed tomography.
Patient navigation in cancer was championed initially at Harlem Hospital in 1990 by Harold P. Freeman, MD, a prominent New York-based oncologist, in response to disproportionately high breast cancer incidence and mortality rates in the black community. The program provided low-income and underinsured women with breast cancer screening. Navigators took on the role of advocates for patients with abnormal screenings. Navigated patients successfully had a biopsy within a shorter period of time and more often than non-navigated patients. 11 Moreover, the program increased the rate of early-stage cancer detection and increased 5-year survival by 31%. 12 Early detection of cancer does not reduce mortality rates alone; it must be followed by timely treatment. 13 Freeman attributed the reduced mortality in part to the process of navigation, which facilitated prompt diagnosis and treatment, as well as culturally appropriate community outreach and education. Freeman concluded the success of the program was primarily because of free and low-cost breast cancer screening and early diagnosis. 13,14
Patient Navigation in Cancer Screening, Diagnosis, and Management
The National Cancer Institute implemented the Patient Navigation Research Program (PNRP) 15 to address the need for standardization of navigation programs across health systems. Initiated in the era before publication of the National Lung Screening Trial (NLST), 16 the PNRP focused on eliminating disparities for screening, follow-up, and treatment in breast, cervical, prostate, and colorectal cancer in vulnerable populations at 9 project sites across the United States. The PNRP found navigation increased diagnostic resolution after an abnormal screening, decreased time to diagnostic resolution, and improved treatment initiation in patients who characteristically do not seek treatment within 90 days of diagnosis. Furthermore, navigated patients reported an increase in satisfaction and quality of life. 15 Navigation programs have been shown to increase rates of cancer screening by 10.8%–17.1% and to increase adherence to follow-up by 21%–29.2%, according to a literature review. 17 Patient navigation programs have been successful in the screening, diagnosis, and management of breast, colorectal, prostate, and cervical cancer in vulnerable populations. 11 –13,15
The Case for Patient Navigation in Lung Cancer Screening, Diagnosis, and Management
An estimated 154,050 Americans will die from lung cancer in 2018, making it the most preventable and leading cause of cancer mortality in the United States. 18,19 Most lung cancer patients are diagnosed at an advanced stage and have a 5-year survival rate of less than 30%. 20 Early diagnosis is crucial, as 5-year survival increases to 56% if lung cancer is found at a localized stage. However, currently, only 16% of lung cancer cases are diagnosed at an early stage. 19 Smoking accounts for 80% of lung cancer deaths in the United States, with the quantity and duration of smoking correlating closely with mortality risk. 19 The relative risk for developing lung cancer in smokers is 25. 19
In 2011, the landmark NLST investigated whether low-dose computed tomography (LDCT) or single-view poster-anterior chest radiography is more effective in reducing lung cancer mortality. NLST reported a 20% relative decrease in lung cancer mortality with annual LDCT compared with radiography. 16 In 2013, the United States Preventive Services Task Force recommended annual lung cancer screening using LDCT for persons ages 55 to 80 years who are in good health, have a 30 pack-year or more smoking history, and currently smoke or have quit within the past 15 years. 18 Subsequently, the Centers for Medicare & Medicaid Services approved lung cancer screening as an additional preventive service benefit. 18 Despite these and other recommendations issued by several professional organizations, uptake remains low. 18,19 The 2010 National Health Interview Survey found that only 2%−4% of high-risk smokers received LDCT. In 2015, 6.8 million smokers were eligible for LDCT but only 3.9% (262,700) underwent the procedure. 18
When a new screening test becomes available, racial and socioeconomic disparities emerge in test use, stage at diagnosis, and mortality. Over time these disparities tend to decline but endure. 21,22 LDCT, as a relatively new screening test, is no exception to this pattern. Blacks are more likely to have advanced disease, experience less definitive surgery, and have lower rates of lung cancer survival than whites. Black patients also are more likely to be unaware of screening, underinsured, and to have lower socioeconomic status – factors that contribute to decreased screening rates for lung cancer. 22 Ironically, recent data suggest that screening with LDCT reduces mortality in black patients more so than in white patients. 22 LDCT uptake is essential in blacks, but also is important across the spectrum of patients at risk for disparities in lung cancer screening. Applying the lessons of Freeman, it is reasonable to believe that the use of patient navigation in lung cancer screening and management has the potential to improve outcomes and reduce lung cancer mortality in blacks and other vulnerable populations.
Given the probable impact of patient navigation related to lung cancer screening and follow-up care, it is important to identify quality metrics that will maximize the benefit of these important initiatives. Despite the existing literature on patient navigation, there is a dearth of published data on navigation in lung cancer and no consistent metrics to measure the success of navigation in lung cancer care. In this paper the study team aims to: (1) conduct a systematic review of existing trials addressing the utilization of patient navigators for cancer care, (2) extrapolate and define quality metrics for patient navigation programs, and (3) propose a set of national metrics to define quality in patient navigation for lung cancer screening, with the ultimate goal of reducing morbidity and mortality from lung cancer in vulnerable populations.
Methods
The study team performed an independent search of the PubMed database in order to identify metrics used to assess the effectiveness of navigation. Using criteria for randomized controlled trials (RCTs), investigators searched for articles containing “nurse navigator” and “cancer,” “nurse navigation” and “cancer,” “oncology nurse navigator,” “patient navigation” and “cancer,” and “navigation” and “cancer” in May 2018. In order to better focus on lung cancer, search criteria were widened to any study design that investigated the impact of patient navigation on lung cancer. Search terms included “nurse navigator” and “lung cancer,” “nurse navigation” and “lung cancer,” “lung cancer screening nurse navigator,” “patient navigation” and “lung cancer,” and “navigation” and “lung cancer.” Inclusion criteria were peer-reviewed RCTs published in the last 15 years. Studies had to address the effectiveness of navigation in breast, colorectal, cervical, prostate, and lung cancer compared to usual care. Additionally, retrospective chart reviews on lung cancer navigation that were published in the last 15 years were considered. Other forms of navigation and other chronic diseases were excluded. Articles that did not address important outcome measures were excluded, such as protocols and studies that did not focus solely on navigation. Titles and abstracts were screened by 2 investigators (CSS, JAB). Articles that met the criteria were reviewed and summarized. Reference lists of included articles were reviewed for pertinent publications. Discrepancies were mitigated by discussion and consensus. Studies that met the inclusion criteria underwent a data extraction process that included author, year, study design, participants, recruitment strategy, intervention, and results. Extracted information was entered and stored in tables available to all investigators. Data extraction was completed by a single investigator (CSS) and audited by 2 additional investigators for accuracy (GCK, JAB). Investigators synthesized findings employing a narrative approach. Because of heterogeneity in the existing literature, results of this review were summarized descriptively.
Results
Characteristics of reviewed articles
The initial search yielded 368 papers published since 2005; of these 22 unique articles met all inclusion criteria. Upon concentrating search terms to focus exclusively on lung cancer navigation, an additional 413 abstracts were identified. Following review, an additional 4 were obtained for a total of 26 papers for analysis (Figure 2). The bulk of studies occurred in the United States, 1 took place in Denmark, 23 and 2 in Canada. 24,25 The smallest sample size was 21 participants 26 and the largest was 5240 participants. 24 The majority of studies focused on black, Latino, or broadly vulnerable populations. Only 1 study targeted Asian and Pacific Islander populations. 27 The 23 RCTs and 3 retrospective chart reviews varied in methodological quality. The 26 trials included in this review are summarized in Table 1; the 4 studies focusing solely on lung cancer are outlined in Table 2.
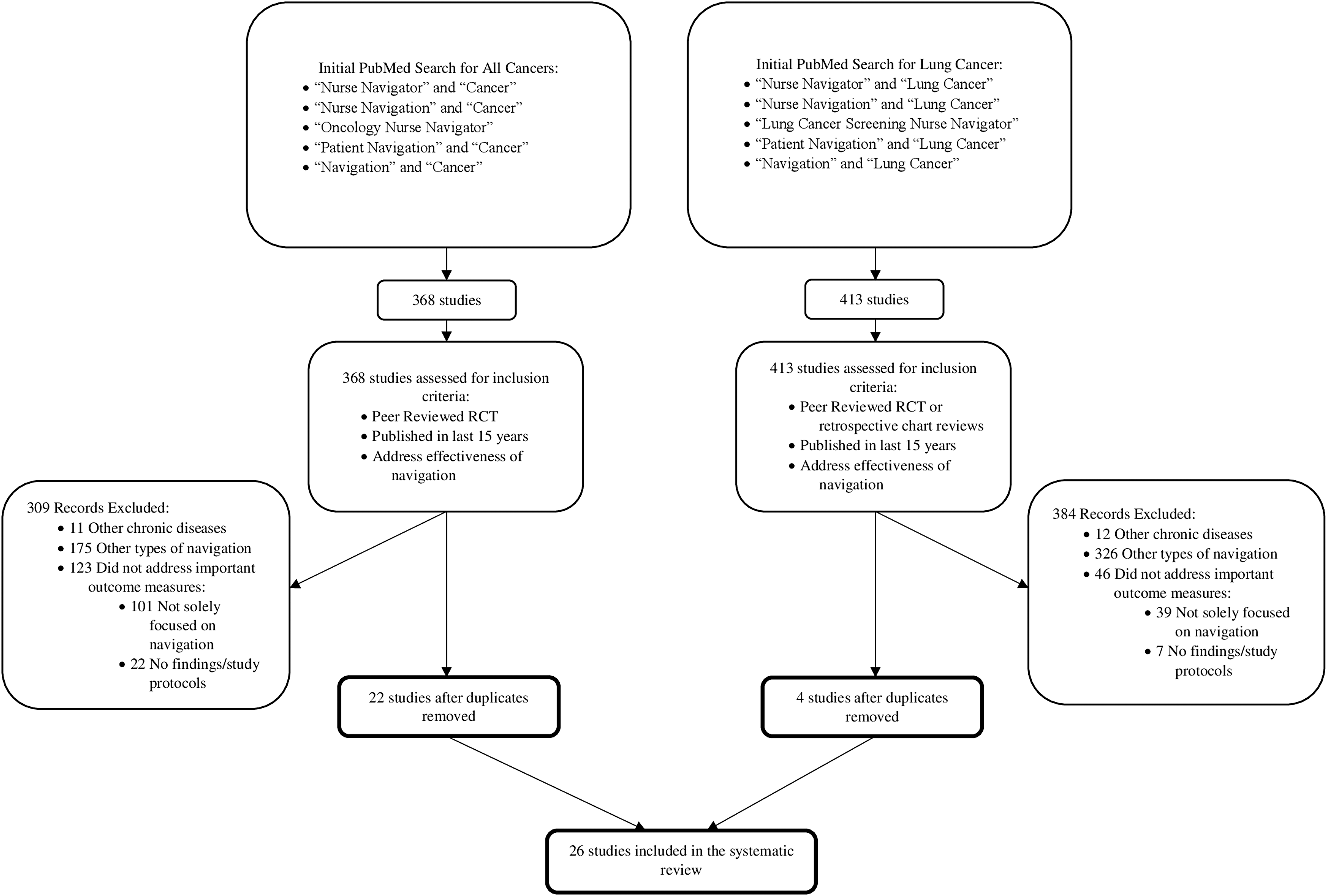
A flowchart of the literature search and study selection. RCT, randomized controlled trial.
Summary of Included Patient Navigation Studies
Randomized controlled trial.
Retrospective chart review.
Summary of Included Lung Cancer Patient Navigation Studies
Patient navigation metrics in cancer screening, diagnosis, and management
Five consistent metrics were found to be related to screening outcomes that are measured in cancer patient navigation studies. The metrics are: (1) screening rate, (2) compliance with follow-up, (3) time to treatment initiation, (4) patient satisfaction, and (5) quality of life. One study discussed cultural competency. No studies reported complication rates associated with completing diagnostic studies or results of screening findings and evaluation.
Screening rate
Screening rate is a fundamental metric of patient navigation. Navigation programs in vulnerable populations aim to improve screening uptake. Eight RCTs measured screening rate, 7 of which concentrated on vulnerable populations. In trials encompassing the general cancer patient population, navigated patients had higher uptake in colorectal and lung cancer screenings when compared to usual care patients. 24,28 Low-income and minority patients experienced a substantial increase in cervical, breast, and colorectal screening when navigated. 27,29 –33 In fact, one RCT found vulnerable patients have 1.5 times greater odds of completing a colonoscopy if they have a patient navigator. 30 Another trial offered culturally-tailored, language-concordant navigation and found that navigated patients were more than twice as likely to be screened for colon cancer when compared to usual care patients. 29
Compliance with follow-up
Compliance with follow-up is a key metric of patient navigation and encompasses follow-up after suspicious findings as well as continuing annual screenings. In the studies examined in this review, 7 measured compliance with screening. One RCT on colonoscopy completion after a positive sigmoidoscopy or fecal occult blood test found navigated patients had higher rates of completed colonoscopy than usual care patients, though differences were not statistically significant. 34 Trials focusing on vulnerable populations also found navigation to be effective in increasing compliance with screening programs and compliance through to diagnostic resolution in breast and colorectal cancer. 26,29,35 –38 One RCT on colonoscopy adherence among low-income minorities found that 54% of patients successfully completed colonoscopy compared to 13% of usual care patients. Additionally, 86% of navigated patients had excellent or very good colonoscopy prep. There was not a statistically significant difference between navigated and usual care patients, but compliance with screening preparation is worth noting. 26 One study that utilized culturally-trained patient navigators was successful in increasing compliance with annual and follow-up screenings. 29 No studies evaluated the impact of navigation on compliance with follow-up in lung cancer patients.
Time to treatment initiation
Time to treatment initiation is the umbrella metric for diagnostic and treatment timelines. Time to treatment initiation includes time from suspicious finding to active observation, chemotherapy, radiation, biopsy, or surgical intervention. Five RCTs measured time to treatment initiation, 4 of which focused on vulnerable populations. In vulnerable populations patient navigators shortened time to diagnosis and increased timely adherence with diagnostic evaluation in breast, colorectal, and prostate cancer. 35,39,40 A retrospective chart review evaluating the impact of patient navigation on time to treatment initiation in lung cancer patients found a significant decline in time from referral to primary consult, treatment, and radiation. 25 In comparison to usual care patients, navigated patients with lung cancer experienced an average reduction of 22 days from abnormal finding to treatment. 41,42 Navigated patients with abnormal breast, cervical, or colorectal screenings experienced significantly quicker times to diagnostic resolution at 6 months compared to usual care patients. The diagnostic resolution rate at 15 months was 65% higher in navigated patients. 43 The impact of navigation on time to diagnostic resolution in vulnerable populations may not be seen immediately; however, the impact is apparent and sustained over longer periods of follow-up. 44
Patient satisfaction
Patient satisfaction is a patient-reported metric and can be applied to satisfaction with navigation or with the entirety of care. Four reviewed RCTs measured patient satisfaction. Breast, colon, and lung cancer patients who had patient navigation reported significantly higher levels of satisfaction than usual care patients. 23,45 Among vulnerable populations, one RCT found navigated women with abnormal mammogram findings reported significantly higher patient satisfaction than usual care patients. 39 Another RCT evaluating the effectiveness of patient navigation assisting vulnerable populations overcome barriers to colorectal screening found that 100% of navigated patients were satisfied with navigation services. 26
Quality of life
Quality of life encompasses levels of anxiety, depression, and distress. Six RCTS measured quality of life. An RCT that involved recently diagnosed breast cancer patients found navigated patients had lower levels of distress, anxiety, and depression after 12 months. 23 In contrast, another trial found no difference in depression scores between navigated and non-navigated patients. 46 Four RCTs found navigated patients and usual care patients had no significant differences in quality of life. 23,45,47,48 Conversely, vulnerable women with abnormal mammogram results reported lower levels of anxiety in the navigation group than in the usual care group. 39
Discussion and Identifying Key Quality Metrics for Patient Navigation in Lung Cancer Screening
Patient navigation has been successfully implemented as a way to reduce cancer disparities in vulnerable populations. Thus far, navigation programs in breast, colon, cervical, and prostate cancer have been effective in eliminating some barriers vulnerable populations face when seeking cancer care. 15 In lung cancer, no studies investigated navigation's impact on compliance with follow-up and no studies focusing solely on lung cancer measured patient satisfaction or quality of life.
Because of the recent introduction of LDCT, history suggests disparities in lung cancer screening and mortality will rise, especially among vulnerable populations. 21,22 In order to address this, the study team proposes utilizing patient navigation programs with the implementation of key quality metrics that would allow full benefits for both patients and health care systems.
Based on this review of the literature, the team proposes the following metrics for lung cancer navigation programs – (1) screening rate, (2) compliance with follow-up, (3) time to treatment initiation, (4) patient satisfaction, and (5) quality of life – as well as adds 2 additional metrics: (6) biopsy complications and (7) cultural competency (Table 3).
Summary of Proposed Lung Cancer Patient Navigation Quality Metrics
Study including cultural competency evaluated the impact on screening rate and compliance with follow-up.
Screening rate
Screening rate is a core metric for vulnerable population navigation programs in lung cancer and can be measured objectively with medical records or through insurance claims data. 49 Increasing lung cancer screening rates in vulnerable populations through navigation may decrease disparities and lung cancer mortality. 28 LDCT is a newer screening test; thus, uptake is currently low. Fewer than 4% of eligible Americans get screened annually. Vulnerable populations are even less likely to be aware of the test. 22 Considering this lack of knowledge and the benefits of early detection, screening rates need to be increased. 19,22 Navigation programs have success with increasing general cancer detection rates and lung cancer screening uptake. 28 In vulnerable populations, patient navigation successfully increases the rate of cancer screenings. 29 –32
Compliance with follow-up
Patient navigation programs in lung cancer that are tailored for vulnerable populations should measure compliance with follow-up as a metric. Compliance can be measured quantitatively using medical records or insurance claims. 49 LDCT requires annual screening and follow-up, which highlights the need for navigation. Vulnerable populations, particularly blacks, may be more likely to be lost to follow-up. In fact, one study found that of 15 black patients with Lung-RADS 3 who required further imaging, 6 patients did not present for follow-up. 50 Patient navigation improves compliance with screening programs and compliance through to diagnostic resolution in vulnerable populations. 26,29,35,36
Time to treatment initiation
The metric time to treatment initiation should be measured in lung cancer navigation programs in order to maximize favorable outcomes and minimize cancer morbidity and mortality. Vulnerable patients experience treatment delays more than the general population. 3,51 Because lung cancer mortality is closely related to stage of presentation, it is imperative to get patients into treatment promptly after suspicious findings. 19 Time to treatment initiation can be measured with medical records or insurance claims. 49 Patient navigation for vulnerable populations shortens time to diagnosis. 39,40
Patient satisfaction
Medicare already emphasizes the importance of patient satisfaction through the Consumer Assessment of Healthcare Providers and Systems and Hospital Consumer Assessment of Healthcare Providers and Systems. 52 Therefore, patient satisfaction is a key metric for lung cancer navigation. Patient satisfaction can be measured as a self-reported metric with the Patient Satisfaction with Cancer-Related Care survey to look at satisfaction with care. 49,53 To address satisfaction with navigation, programs can use the Satisfaction with Patient Navigation-Interpersonal scale. 49,54 Navigation increases levels of patient satisfaction in vulnerable patients. 26,39
Quality of life
Quality of life is a patient-based self-reported metric for lung cancer navigation. This metric contains anxiety, depression, distress, and overall quality of life. Quality of life can be measured using the validated Functional Assessment of Cancer Therapy survey. 49,55 Anxiety, depression, and distress can be measured using surveys from the Patient-Reported Outcomes Measurement Information System, 49,56 the Hospital Anxiety and Depression Scale, 23,57 or the Zung Self Rating Anxiety Scale. 39,58 Navigated patients do not report a difference in quality of life 23,47 or depression. 46 However, navigation reduces anxiety in vulnerable populations. 39
Biopsy complications
Biopsy complications should be a metric for lung cancer navigation programs despite a lack of existing literature. Patient navigators are tasked with tracking patients over time to ensure completion of screening and treatment. Navigators also help coordinate follow-up, including timely follow-up of any complications. 17 The study team proposes that because patient navigators successfully improve rates of screening and compliance in vulnerable populations, they would help reduce biopsy complications by facilitating appropriate follow-up at all stages. The NLST found the rate of at least 1 complication from a diagnostic evaluation procedure after an abnormal screening test was lower in LDCT patients than in radiography patients. 16 Navigators may be able to reduce biopsy complications in vulnerable populations with timely follow-up, and perhaps reduce morbidity and mortality. The team recommends that biopsy complications be measured with medical records or insurance claims. 49 Future research is needed to investigate a patient navigator's impact on biopsy outcomes in lung cancer.
Cultural competency
Cultural competency is a vital metric for patient navigation in lung cancer. Cultural competency can be a patient-reported measure, recorded with the Perceived Similarity to Navigator Scale, which is adapted from the Perceived Similarity to Physician Scale. 49,59 Cultural competence encompasses language, shared decision making, respect, and discrimination. 49 These are important concepts for connecting with vulnerable populations. Black patients report an increase of medical mistrust and discrimination that prevents them from seeking care and contributes to advanced cancer stage presentation, and thus mortality disparities. 51 The PNRP found language interpretation is one of the main barriers to seeking cancer care in patients with abnormal screenings. 15 Shared decision making is a concept discussed by the National Cancer Society and should be part of annual lung cancer screening. 19 Culturally-trained navigators would also be able to assist vulnerable patients with increasing their health literacy and thus decrease disparities in care. 5 Freeman, the creator of patient navigation, felt navigation was successful in part because of culturally appropriate education and outreach. 13 When cultural competency is encompassed in navigation programs, screening rates and compliance increase among vulnerable populations. 29 However, no studies were identified that measured the cultural competency of navigators. Future studies should evaluate what is meant by cultural competency and the efficacy of culturally-competent patient navigators working with vulnerable populations in lung cancer programs.
Cost-effectiveness
Although cost-effectiveness is not a patient navigation metric included in this review, it is worth noting the importance of evaluating patient and system costs of patient navigation programs. Patient navigation programs must meet the standards of excellence set forth by the proposed metrics and should be cost-effective in order to justify centralized implementation in health systems and in other settings. Compared to usual care, patient navigation programs have been found to be cost-effective in cancer screening and along the continuum of care. 60,61 A cervical cancer screening patient navigation program tailored to vulnerable populations found navigation to be cost-effective compared to usual care. 62 A capitated payment lung cancer treatment patient navigation program for Medicare patients was cost-effective with an incremental cost-effectiveness ratio of $19,312 per quality-adjusted life year. 63 A patient navigation program at Henrico Doctors' Hospital found a navigation model assigning breast cancer patients to a navigator at time of suspicious finding through 12-months post diagnosis was effective in increasing revenue, standardizing care, and increasing patient retention throughout the care continuum. An unintended consequence was an increase in revenue, so that after 1 year, the program covered the costs of patient navigation. 64 Further research is needed to investigate both short-term and long-term cost-effectiveness of patient navigation programs in lung cancer screening aimed at vulnerable populations.
Phases of navigation
Patient navigation in cancer screening involves 3 main phases: (1) navigation to screening, (2) navigation to diagnostic evaluation, and (3) navigation to treatment. Navigation to screening consists of navigators reaching out to patients, identifying those who satisfy eligibility criteria, and offering navigation services, which may include education, shared decision making, and appointment scheduling for lung cancer screening. Navigation success is measured by the screening rate metric. The second phase, navigation to diagnostic evaluation, involves helping patients complete follow-up assessments after an abnormal screening test and facilitating annual screening. Among persons with suspicious findings, navigators would monitor follow-up after an abnormal LDCT result and help to resolve any complications that might result from diagnostic evaluation. Navigation to diagnostic evaluation is measured using the metric compliance with follow-up. The final stage of the navigation process, navigation to treatment, involves ensuring that diagnosed patients receive prompt treatment and helping patients receive care that can maximize the likelihood of recovery and quality of life. Specifically, in lung cancer, this would include following patients with a malignancy and ensuring they receive treatment quickly as well as providing advice, compassion, and further information about treatment options in an effort to reduce anxiety, distress, and depression. The metrics time to treatment initiation, quality of life, and biopsy complications measure navigation to diagnostic evaluation. Navigation to diagnostic evaluation also can measure survival rates of navigation programs and this metric should be followed, though meaningful results may take 2–5 years post treatment in order to have the greatest clarity of impact. Cultural competency and patient satisfaction metrics should be measured throughout the navigation process.
Navigation programs have been shown to increase screening rates, raise compliance with follow-up, shorten time to treatment initiation, and improve quality of life and patient satisfaction. 28,38,39,41,45 These factors, paired with a hypothesized reduction in biopsy complications, and culturally competent care focused on vulnerable patients who may distrust health care systems, lack health literacy, need interpretation services, and others who may fall through safety net programs, are hallmarks of patient navigation in lung cancer. Patient navigation programs that contain these key features will improve patient outcomes as well as increase patient retention in the health care system. An increase in patient retention can lead to an increase in net revenues as well as in downstream revenues, allowing patient navigation programs to be a cost-effective option for hospitals and payers. 64 In the final analysis, improvements in patient outcome should be the ultimate goal, but savings also might come from preventing late-stage cancers from developing.
In order to create a successful lung cancer screening patient navigation program aimed at vulnerable populations, an institution should be organized to meet the proposed quality metrics in a cost-effective manner. Patient navigation programs should aim to increase screening rates and compliance with follow-up, decrease time to treatment initiation and biopsy complications, improve quality of life, and provide culturally competent care that focuses on patient satisfaction and long-term survivorship of patients. If a navigation program contains these key components, the study team believes it will be successful in the ultimate goal of reducing morbidity and mortality from lung cancer in vulnerable populations.
Strengths and limitations
The strengths of this study include the meticulous nature of the literature search and the rigor of the inclusion criteria. The majority of vulnerable populations examined in included articles were based on socioeconomic status and race, leaving gaps in what is known about navigation in other vulnerable populations such as veterans, trans/gender nonconforming people, and residents of rural communities. Moreover, the majority of studies dealing with race involved blacks and Hispanics, with only 1 study examining Asians. Although there is limited representation of many vulnerable populations in the navigation literature, the study team believes that these metrics are generalizable and beneficial across the spectrum of those who are vulnerable to disparities in lung cancer screening. Further research is needed to fully investigate the efficacy of patient navigation programs focused on other facets of vulnerable populations, particularly because the definition of vulnerable populations encompasses a large portion of the population who are at risk for disparate health outcomes.
A lack of consistency in metrics provided a challenge for synthesizing trials. Numerous trials investigate dissimilar cancers and metrics. Heterogeneity in published literature made conclusive declarations about patient navigation quality metrics difficult. Despite the lack of quantitative findings, a qualitative review of trials provides a comprehensive overview of metrics measured in cancer navigation programs. The present review suggests quality metrics for future patient navigation programs focused on lung cancer in vulnerable populations.
Conclusion
This systematic review indicates that patient navigator programs can improve screening rates, compliance with follow-up, time to treatment initiation, patient satisfaction, and quality of life among vulnerable populations. Specifically, in lung cancer, navigated patients have demonstrated greater screening uptake and more rapid initiation of therapy, although gaps in knowledge related to program implementation and longer term outcomes remain.
Based on this analysis, the study team recommends that lung cancer screening programs aimed at vulnerable populations utilize patient navigation along with tracking the following metrics: (1) screening rate, (2) compliance with follow-up, (3) time to treatment initiation, (4) biopsy complications, (5) patient satisfaction, (6) quality of life, and (7) cultural competency.
Although this proposal identifies metrics that should be followed for any patient navigation program, the overall number of cancers detected, nodule characteristics, incidental findings, and patient outcomes should be followed and would be expected as part of the current American College of Radiology (ACR) Reporting and Data Systems (RADS). 65 ACR programs utilizing navigation must track and report RADS data in order to ensure compliance with follow-up and prompt treatment initiation in vulnerable patients. In addition, all navigated patients undergoing lung cancer screening must receive smoking cessation counseling in order to comply with the expectations of the program.
To implement a high-quality navigation program that succeeds in these areas, the study team proposes that patient navigators working within lung cancer screening programs aimed at vulnerable populations have a set of specific skills. Navigators must have an understanding of cancer biology and lung pathophysiology; knowledge of symptoms, side effects, and complications of treatments; the ability to advise both patients and their loved ones; an understanding of informed consent, patient confidentiality, and the Health Insurance Portability and Accountability Act; as well as strong familiarity with shared decision making and cultural competency. Funding for patient navigation programs across the United States should be based on the tracking and reporting of these core metrics. If programs are able to meet these criteria reliably, the program should receive funding and reimbursement from insurance payers. Future research should investigate how to negotiate and propose contracts for reimbursement in lung cancer patient navigation with the ultimate goals of enhancing patient-centered care and improving lung cancer mortality.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. This work was supported by a grant from the Bristol-Myers Squibb Foundation titled, “Engaging a Learning Community to Increase Lung Cancer Screening in Vulnerable Populations,” and by the Dreidink Scholarship.