
Abstract
The 30-day readmission rate is a common performance indicator for hospitals and accountable care entities. There is reason to question whether measuring readmissions as a function of hospital discharges is an appropriate measure of performance for initiatives that aim to improve overall cost and quality outcomes in a population. The objectives of this study were to compare trends in 30-day readmission rates per discharge to population-based measures of hospital admission and readmission frequency in a high-risk statewide Medicaid population over a 5-year period of quality improvement and care management intervention. Further, this study aimed to examine case-mix changes among hospitalized beneficiaries over time. This was a retrospective analysis of North Carolina Medicaid paid claims 2008 through 2012 for beneficiaries with multiple chronic or catastrophic conditions. Thirty-day readmission rates per discharge trended upward from 18.3% in 2008 to 18.7% in 2012. However, the rate of 30-day readmissions per 1000 beneficiaries declined from 123.3 to 110.7. Overall inpatient admissions per 1000 beneficiaries decreased from 579.4 to 518.5. The clinical complexity of hospitalized patients increased over the 5-year period. Although rates of hospital admissions and readmissions fell substantially in this high-risk population over 5 years, the 30-day readmission rate trend appeared unfavorable when measured as a percent of hospital discharges. This may be explained by more complex patients requiring hospitalization over time. The choice of metrics significantly affects the perceived effectiveness of improvement initiatives. Emphasis on readmission rates per discharge may be misguided for entities with a population health management focus. (Population Health Management 2015;18:351–357)
Introduction
H
As reducing hospital readmissions has been identified as a key health care improvement strategy, readmission measures are increasingly being integrated into policy frameworks and contractual performance standards. The Centers for Medicare & Medicaid Services (CMS) has been at the forefront of this effort, beginning in 2009 with the public reporting of readmission rates for most acute care hospitals in the United States, followed by payment reductions to hospitals with higher-than-expected readmission rates starting in October 2012. In these initiatives, the hospital discharge is the unit of analysis and the discharging hospital is held primarily accountable for risk-standardized readmission rates per discharge. 10 The all-cause readmission rate, measuring readmissions per discharge, has been further applied by CMS in the Community-based Care Transitions Program, in which participating community-based organizations aim to collaboratively reduce readmissions, 11 and as one of 33 performance measures for Accountable Care Organizations (ACOs) in the Medicare Shared Savings Program. Beyond these Medicare-specific programs, readmission rates calculated as a percent of hospital discharges have now been adopted as a Medicaid adult core quality measure, 12 as a health plan quality measure under the National Committee for Quality Assurance Healthcare Effectiveness Data and Information Set, 13,14 and into private sector initiatives including performance contracts with provider entities or ACOs. 15,16
Conceptually, the goal of reducing the rate at which hospital-discharged patients are readmitted may be in conflict with the broader goal of reducing avoidable hospital utilization in the population overall under an accountable care framework. Chronically ill beneficiaries, particularly those with multiple chronic conditions, account for 98% of Medicare readmissions. 17 Because these beneficiaries have a chronic, persistent risk of decompensation or acute exacerbation of chronic disease requiring hospitalization, interventions that improve access to primary care, quality of chronic disease care, and coordination among care providers should be expected to reduce the frequency of inpatient admissions in a well-managed population over time. Conceivably, that would lead to a shift in the inpatient demographics, with only the “sickest of the sick,” those at highest risk of readmission, requiring hospitalization. Is it possible, then, that improving the overall care of patients with chronic conditions will paradoxically increase the hospital readmission rate by altering the risk profile of those who require hospital admission in the first place?
The experience of the North Carolina (NC) Medicaid program provides a unique opportunity to examine this question. Beginning in late 2007, NC expanded statewide enrollment of elderly and disabled Medicaid beneficiaries into the Community Care of North Carolina (CCNC) enhanced medical home model of care. 18,19 Under CCNC management, which links recipients to a primary care medical home and provides community-based infrastructure for quality improvement and multidisciplinary care management for high-risk patients, NC saw a substantial decrease in inpatient utilization and total cost of care per beneficiary from 2007 to 2011. 20 CCNC's transitional care program, which expanded gradually since its inception in 2008 and currently provides care management support after hospital discharge to more than 2600 Medicaid recipients per month, is considered to be a key contributor to this success. 21 In a prior study, this transitional care program was shown to substantially increase time to first, second, and third readmission among patients with multiple chronic conditions, with much of the benefit realized beyond the first 30 days. 8
The present study aimed to examine 30-day all-cause readmission rate trends among NC Medicaid beneficiaries with multiple chronic conditions between 2008 and 2012. The study reports readmission rates measured as a function of hospital discharges, following the logic most commonly deployed in performance measurement nationally, as well as the population-based measures of 30-day readmission rate per beneficiary-month and overall inpatient rate per beneficiary-month. This study further aimed to describe case-mix trends and inherent readmission risk among hospitalized beneficiaries to test the hypothesis that the risk profile of hospitalized patients will increase over time in a managed population.
Methods
The data for this study came from paid Medicaid claims data during January 1, 2008, and December 31, 2012. Analyses were limited to all NC Medicaid recipients identified as having multiple chronic or catastrophic conditions (MCCs) as defined by 3M Health Information Systems Clinical Risk Group methodology. 22 Recipients dually eligible for Medicaid and Medicare were excluded because of lack of complete Medicare claims data. All inpatient visits were included for this population. Inpatient admissions that occurred within 30 days of a previous discharge were counted as a readmission, regardless of the reason for readmission; same-day hospital transfers were not counted as readmissions. The denominator for per beneficiary measures included all months in which recipients with MCCs were enrolled in NC Medicaid during the year.
To examine changes in case mix of hospitalized beneficiaries over time, hospital discharges were categorized according to the beneficiary's 3M Aggregated Clinical Risk Group (ACRG). To calculate benchmark readmission rates for each of these 18 clinical risk groups, the study team examined all hospitalizations from January 1, 2008, to December 31, 2012, dividing the number of readmissions within 30 days by the number of index discharges to compute an average readmission rate for the 5-year period.
Sensitivity analyses examined trends in 90-day readmission rates per discharge and 90-day readmissions per beneficiary-months. Findings were similar to the 30-day readmission results and not presented here for the sake of brevity.
Results
The number of individuals with MCCs covered under NC Medicaid increased from 127,951 in 2008 to 149,942 in December 2012. Total MCC beneficiary-months were 1,535,407 in 2008; 1,679,263 in 2009; 1,763,091 in 2010; 1,809,051 in 2011; and 1,799,298 in 2012. Total hospital discharges for MCC beneficiaries numbered 74,132 in 2008; 77,681 in 2009; 79,354 in 2010; 82,699 in 2011; and 77,744 in 2012. The rate of readmission within 30 days of discharge fluctuated widely on a month-to-month basis, with an overall upward trend between 18% and 19% over the 5-year period (Fig. 1).
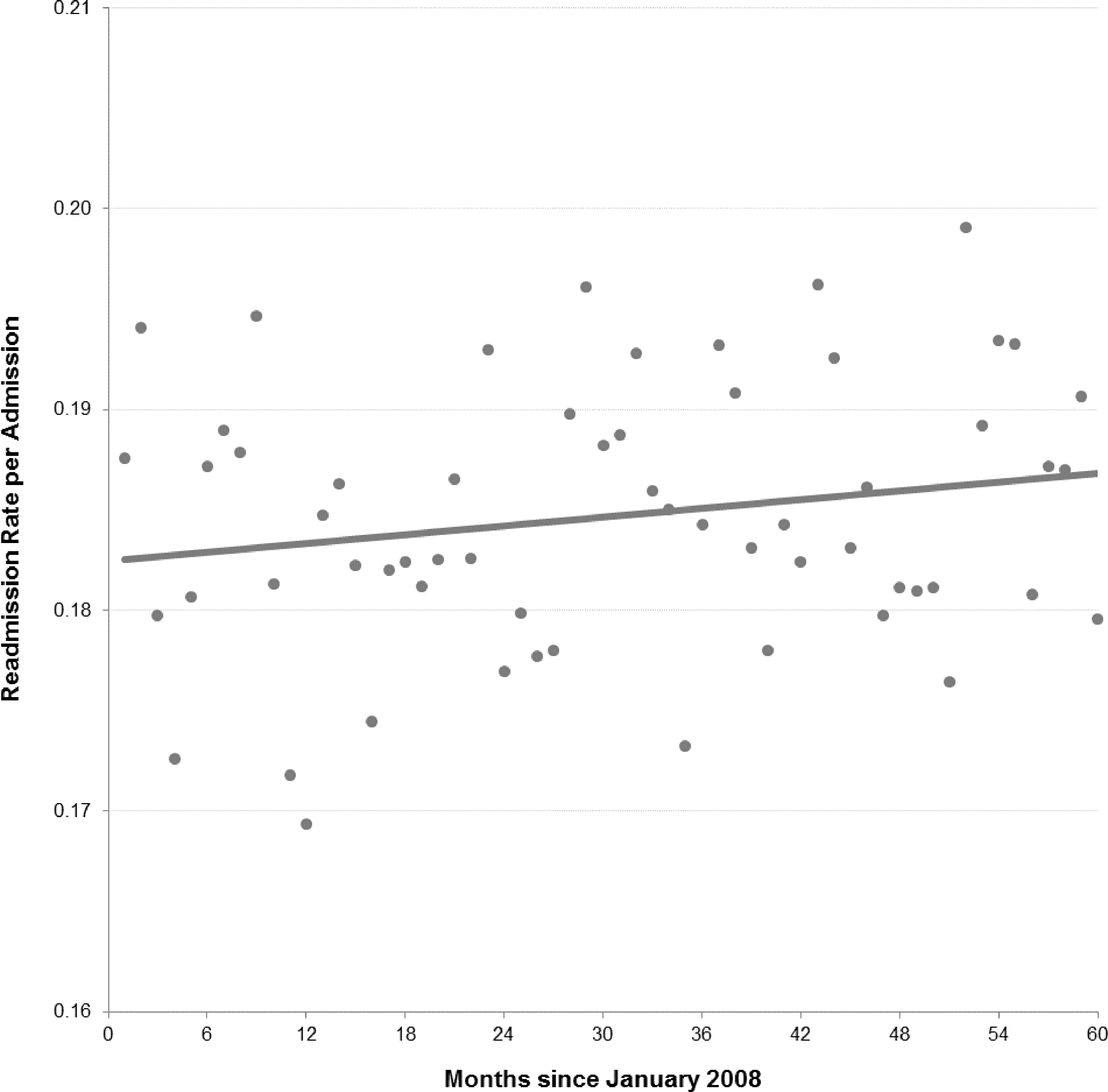
30-Day readmission rate per admission over time; North Carolina Medicaid beneficiaries with multiple chronic conditions.
On a per-beneficiary basis, the rate of 30-day readmissions trended in the opposite direction, declining from 123.3 to 110.7 readmissions per 1000 beneficiaries per year from 2008 to 2012 (Fig. 2). Overall inpatient admissions per 1000 beneficiaries similarly decreased, from 579.4 in 2008 to 518.5 in 2012 (Fig. 3).
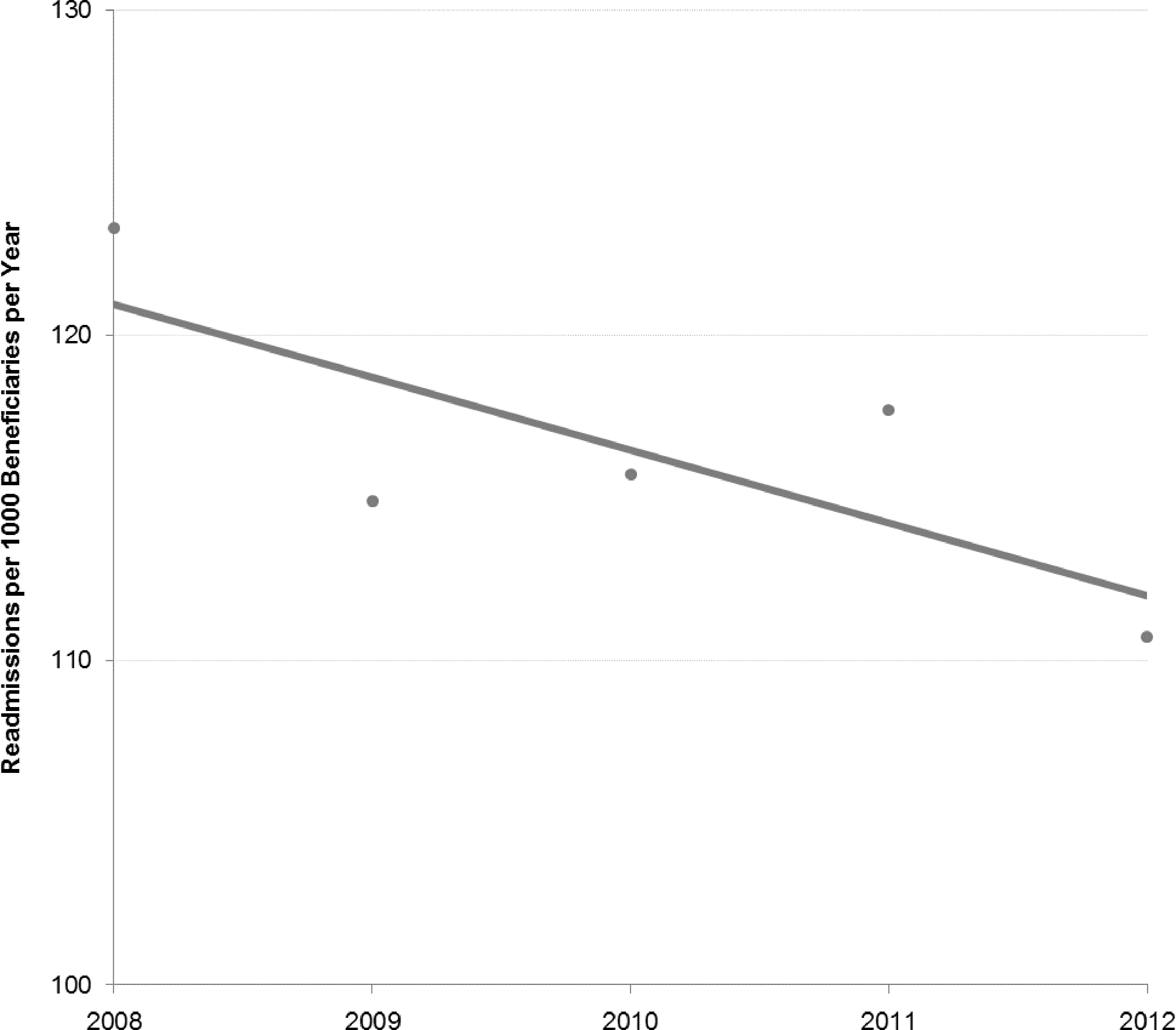
30-Day readmission rates per beneficiary over time; North Carolina Medicaid beneficiaries with multiple chronic conditions
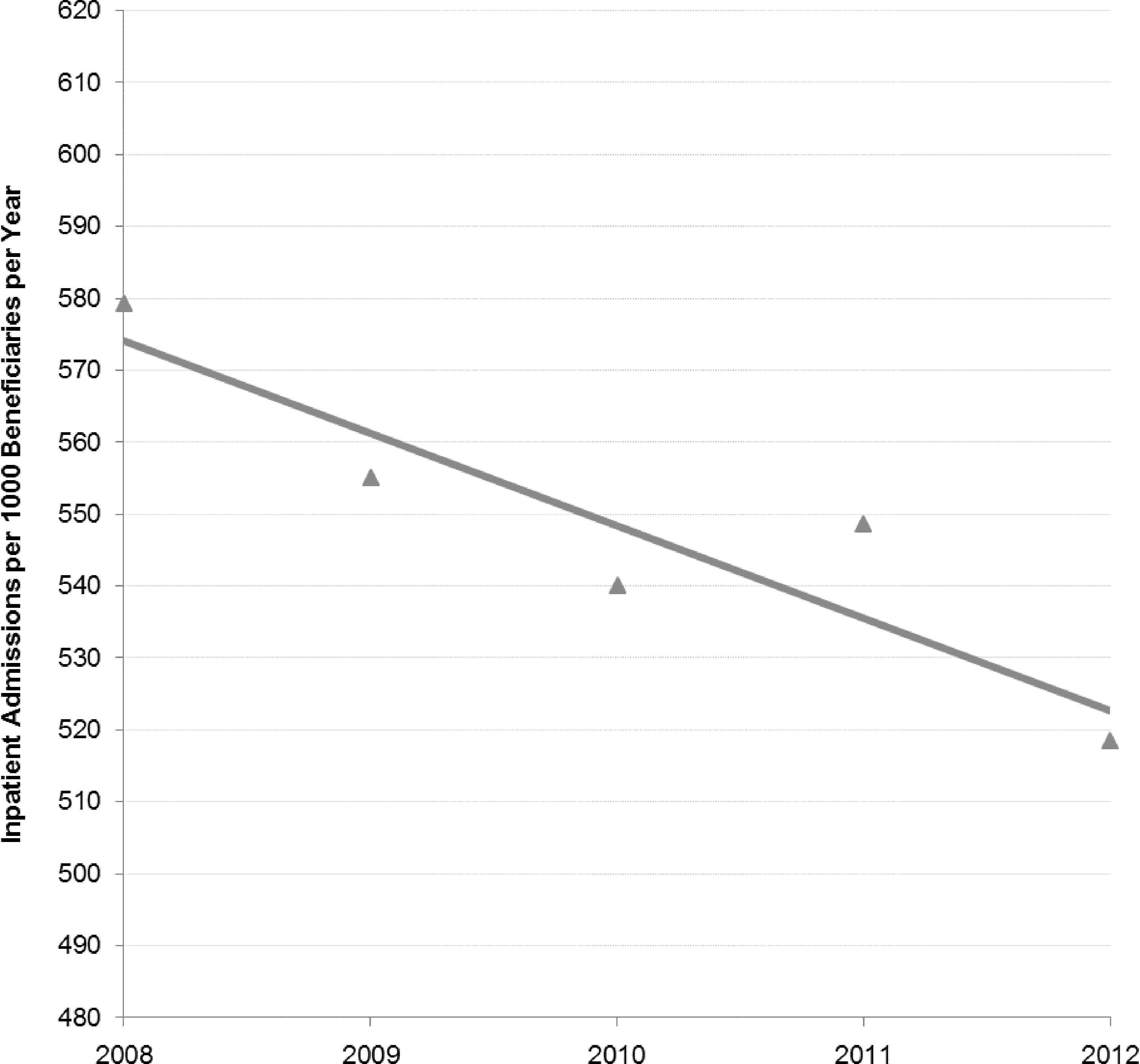
Inpatient admission rates per beneficiary over time; North Carolina Medicaid beneficiaries with multiple chronic conditions.
Benchmark readmission rates, based on the overall rate of readmission within 30 days of discharge for beneficiaries in each of 18 clinical risk groups over the 5-year period, ranged from 5.3% to 41.8% (Table 1). Between 2008 and 2012, the distribution of admissions shifted toward clinical risk groups with higher readmission risk. The proportion of admissions for patients in 10 risk groups with benchmark readmission rates <20% remained stable or declined, while the proportion of admissions for patients in 7 of 8 risk groups with benchmark readmission rates >20% increased. This resulted in an overall increase in expected readmission rate from 18.6% to 19.2%. Logistic regression analysis demonstrated a statistically significant increase in the risk of readmission for hospitalized patients over time (Wald statistic=11.56, P=.001) with the risk increasing an average of .15% each year.
3M Clinical Risk Groups assigned based on all paid Medicaid claims during the year.
Represents % of discharges followed by a readmission within 30 days for patients in this Clinical Risk Group, 2008–2012 combined
Expected readmission rate calculated by multiplying number of admissions within each Clinical Risk Group by the benchmark readmission rate.
Note that the study team additionally examined benchmark readmission rates as a function of the Diagnosis Related Group (DRG) of the index hospitalization, following the same methodology described for ACRGs, and found a similar trend of higher-risk DRGs making up a larger proportion of the total admissions during each subsequent year.
Discussion and Conclusions
This study compared 2 different approaches for measuring 30-day readmission rates—per discharge and per beneficiary—in the context of a large-scale population health management initiative for Medicaid beneficiaries with chronic conditions. From 2008 to 2012, the proportion of beneficiaries who experienced a 30-day readmission declined by 10.2%, from 123.3 to 110.7 readmissions per 1000 beneficiaries per year, concomitant with a 10.5% decline in overall inpatient admission rates from 579.4 to 518.5 per 1000 beneficiaries per year. When presented as a percent of hospital discharges, however, as commonly deployed in health system or health plan performance measurement, readmission rates trended in the opposite direction—increasing from an average of 18.3% in 2008 to 18.7% in 2012.
Analysis of the clinical complexity of hospitalized beneficiaries, which demonstrated a shift toward greater complexity and greater associated risk of readmission over the 5-year period, provides a possible explanation for these opposing trends. If improvements in access to care, chronic disease management, and care coordination successfully decrease hospitalization rates among chronically ill beneficiaries over time, it is reasonable to expect that those individuals who do require hospitalization will have greater clinical complexity or more advanced illness. The likelihood that hospitalized patients will require readmission within 30 days can be expected to rise accordingly.
Opposing trends in overall admission rates and 30-day readmissions per discharge have been observed in other population-based care improvement initiatives. In a recent evaluation of 14 Quality Improvement Organization-facilitated community-wide initiatives to improve care transitions for Medicare beneficiaries, declines in overall readmission and admission rates were reported in the target population, despite no change in the rate of all-cause 30-day readmissions as a percentage of hospital discharges. 4 A similar pattern was reported in the evaluation of the Medicare Physician Group Practice demonstration, Medicare's first pay-for-performance initiative to incentivize quality improvement and cost efficiency at the level of the physician group practice. Although the number of hospitalizations per beneficiary and share of beneficiaries with 1, 2, and 3 discharges fell over the 5-year performance period, there was a slight rise in the rate of 30-day readmissions per discharge. 23
The present study augments prior studies that have identified weak or inverse associations between the 30-day readmission rate and other measures of health system performance. The 30-day readmission rate has been shown to be weakly or inversely associated with the initial hospital length of stay, inpatient days over an episode of care, Medicare's Hospital Compare process quality measures, and mortality. 10,24,25,26 Alternative methodologies for measuring readmissions per discharge—such as the All-Cause Readmission rate index from United Health Group, CMS 30-day readmission rates from Hospital Compare, and the 3M Potentially Preventable Readmission Rate—also have been shown to correlate poorly with each other, leading to very different hospital performance rankings. 27,28 As health systems increasingly participate in financial arrangements that hold them more accountable for the totality of patient experience, costs, and outcomes for a population, this study's findings should raise additional concerns about the potential for a chosen measure to provide an incomplete or misleading picture of health system performance. When tracking readmissions per discharge, robust methods for risk adjustment must be incorporated to allow not only for cross-sectional comparisons to other entities, but for longitudinal observations within a target population.
NC's large-scale initiative to improve the care of chronically ill Medicaid beneficiaries provided a sizable high-risk population in which to observe admission and readmission trends over 5 years of intervention, but generalizability to non-Medicaid or lower risk populations may be limited. This study's observation that the clinical complexity of hospitalized beneficiaries increased over time was based on claims data, and it is possible that changes in provider coding behaviors to optimize billing may have contributed. However, a shift in case mix was not found within the study population as a whole, which suggests that any coding bias may be negligible.
The choice of health systems metrics and the resulting ratings or rankings of these entities can affect reimbursement levels, the reputation of an organization or system, and decisions about whether or not to continue or modify quality improvement and care coordination initiatives. For high-risk individuals with chronic care needs, who account for the vast majority of hospital readmissions, singular focus on short-term readmission rates would be misguided. To optimize care and outcomes in this population, it will be important to take the long view.
Footnotes
Author Disclosure Statement
Drs. DuBard, Vann, and Jackson declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received the following financial support: This work was supported in part by a grant from the North Carolina Healthcare Quality Alliance and the North Carolina Department of Health and Human Services, Office of Rural Health and Community Care.