
Abstract
Appropriately constructed health promotions can improve population health. The authors developed a practical model for designing, evaluating, and improving initiatives to provide optimal value. Three independent model dimensions (impact, engagement, and sustainability) and the resultant three-dimensional paradigm were described using hypothetical case studies, including a walking challenge, a health risk assessment survey, and an individual condition management program. The 3-dimensional model is illustrated and the dimensions are defined. Calculation of a 3-dimensional score for program comparisons, refinements, and measurement is explained. Program 1, the walking challenge, had high engagement and impact, but limited sustainability. Program 2, the health risk assessment survey, had high engagement and sustainability but limited impact. Program 3, the on-site condition management program, had measurable impact and sustainability but limited engagement, because of a lack of program capacity. Each initiative, though successful in 2 dimensions, lacked sufficient evolution along the third axis for optimal value. Calculation of a 3-dimensional score is useful for health promotion program development comparison and refinements, and overall measurement of program success. (Population Health Management 2013;16:291–295)
Introduction
Three Health Promotion Programs
A hypothetical organization of 5000 individuals sponsors 3 programs designed to reduce risk and manage illness. These initiatives are as follows:
Program 1
In response to a measured prevalence of overweight, sedentary behavior, and high stress, the organization's wellness coordinator creates a walking challenge. A robust communications scheme and provision of free pedometers facilitates recruitment of 1670 members (33%). Participants receive instructions on pedometer use and are assigned to 1 of 3 teams, with a team prize offered for the most steps during the challenge. For the 6-week program duration, the participant pool averages nearly 10,000 steps per day.
Program 2
The organization licenses an online wellness portal that includes an annual health risk assessment (HRA) survey. Employing effective communications and a participation incentive, 2500 people (50%) complete the HRA in the first year. Aggregate data show that the organization's health status is similar to that of the US population. Specific tools for improvement are available to participants through the HRA Web site.
Program 3
The organization sponsors a one-on-one cardiovascular condition management program, because face-to-face consultations are more effective than traditional telephone-based condition management. 1 A nurse educator recruits individuals with cardiometabolic syndrome to meet with her monthly; duration of initial consultations and follow-up meetings are 60 and 15 minutes, respectively. Risk reduction strategies, such as diet and regular exercise, are discussed, the need for cardiovascular medication compliance is reinforced, and recommendations for additional health care are provided. Most of the 24 program participants progress in their condition management. Program costs are offset by medical care savings, and the program receives long-term support.
Will these programs improve the overall population's health? These programs may be well conceived, but is it possible that each has a distinct shortcoming with critical opportunities for improvement?
Health Promotion in Three Dimensions
Multiple models exist for the planning and evaluation of health promotions, with the shared goal of effective population change. The RE-AIM framework identified 5 criteria for success 2 ; reach, efficacy, adoption, implementation, and maintenance. However, this comprehensive type of approach may be unwieldy for project development or evaluation, and an intuitive, practical, and functional model is needed.
The model that follows is not entirely new. Hawe and collaborators postulated that health outcomes are the product of 3 factors: (1) the size of the intervention's effect, (2) the penetration of an intervention into a population, and (3) the effect's sustainability. 3 These parameters facilitate discussion on capacity building as critical to sustaining health promotion benefits, but did not elaborate on effect size or sustainability. Subsequently, the Work Health Promotion Capacity Instrument was developed, which evaluates worksite capacity for programs by measuring the organization's willingness and ability to systematically implement health promotion activities. 4 The goal of this paper is to advance Hawe's concept of 3-dimensional health promotion and offer a practical, measurable approach toward its application.
Progression from the Hawe outline first requires clear definition of the dimensions of effective health and wellness programming. In order to be successful and valuable, programs must be impactful, leading to real reductions in primary, secondary, or tertiary risk. They need to fully engage enough members to effect measurable change to 1 or more health metrics. Finally, health improvements must be sustainable long term to drive a clinically important difference. These axes can be visualized as a health cube, within which the effectiveness of programs can be positioned (Fig. 1). Ideal programs score well in all 3 dimensions. When the program examples described earlier are considered in the context of the wellness cube, limitations become apparent, as depicted in Figure 2. This model is useful in a full range of 10 and 20 prevention initiatives, and may be used as an adjunct to condition management programs. It is very useful for reducing the burden of highly prevalent health risks such as obesity, uncontrolled hypertension, sedentary behavior, and stress.
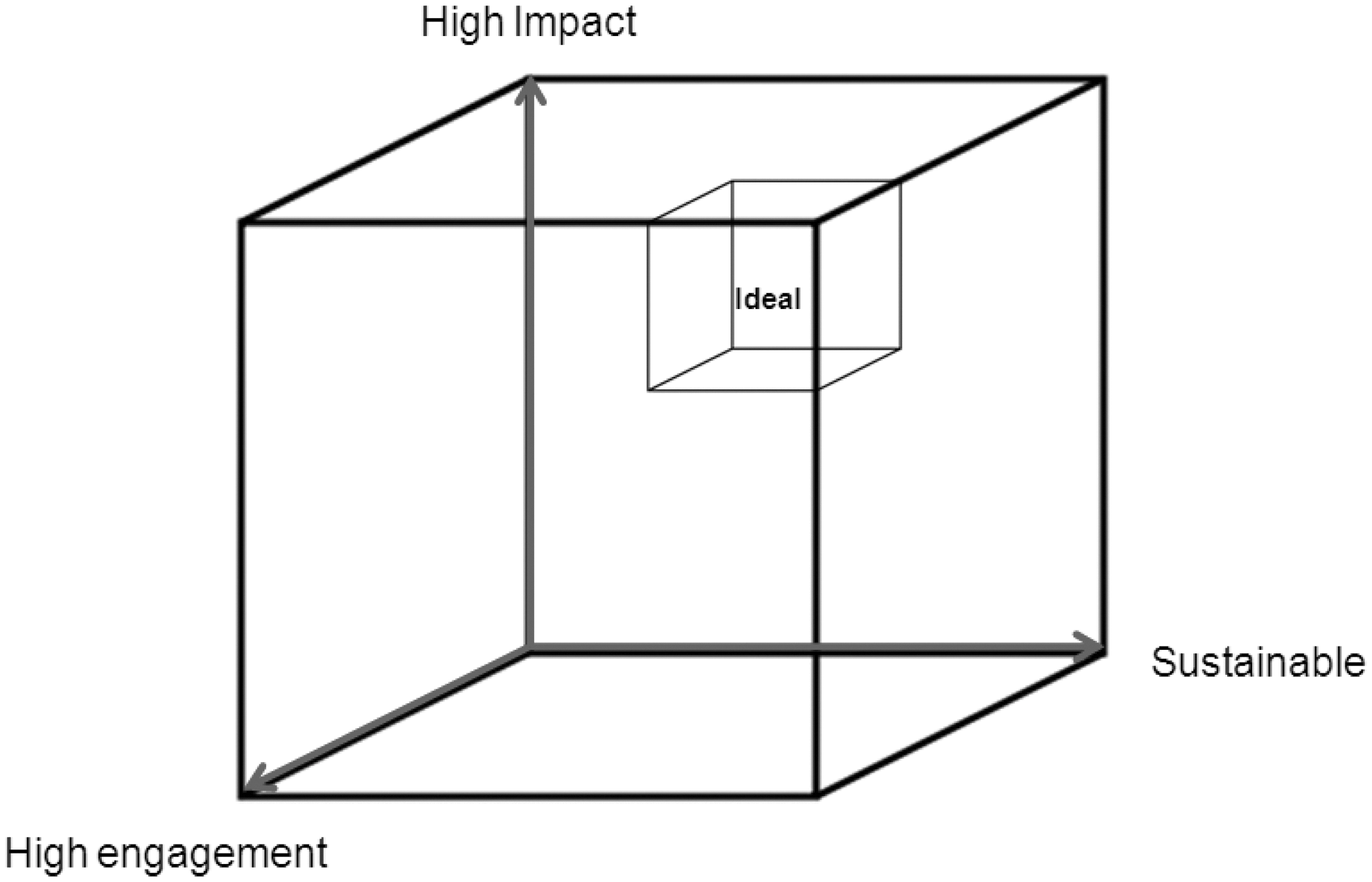
Three-dimensional “health cube” and its application to 3 hypothetical employer health and wellness programs. The “health cube” is used to illustrate the concept that ideal health and wellness programs should be maximally impactful, engaging, and sustainable.
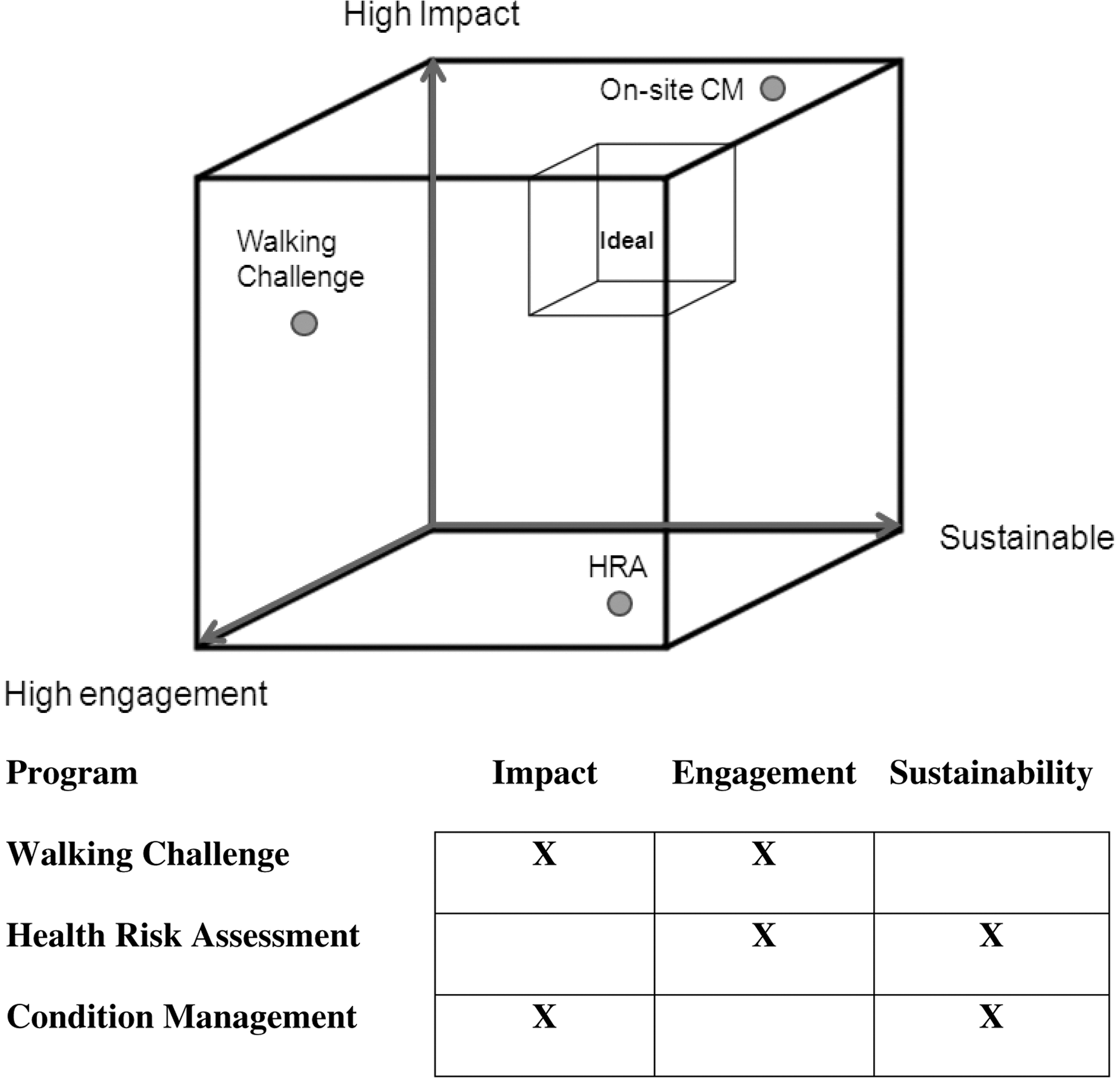
Three hypothetical wellness programs positioned in the wellness cube. The 3 hypothetical case studies described in the text are quantified using the impact, engagement, and sustainability criteria depicted in the 3-dimensional wellness cube. The walking challenge achieved good impact and engagement, but was not sustained. The HRA was reasonably engaging and sustainable, but not impactful. The condition management program was maximally impactful and sustainable, but inadequately engaging.
The walking challenge increased physical activity, thus addressing a primary risk for coronary artery disease, and might also be preventative for other chronic conditions such as diabetes, osteoporosis, obesity, depression, and cancers of the breast and colon. 5 –7 However, primary prevention is associated with habitual activity. 6 The long-term benefit of nonhabitual exercise is unclear. Measurable benefits of weight, lipids, and blood pressure may regress after cessation of regular physical activity. Despite this program's high engagement rate, there was no plan for sustainability and thus the value of this initiative may be questionable.
In the second case, the organization's population was provided with a tool to gauge health and health risk. Engagement rates were high, and the incentivized survey was continued beyond the first year. However, a strategy to translate survey results into practicable tactics at the individual action was absent, as no tactics or incentives effectively linked the HRA with available risk modification tools.
Program 3 had measurable impact and sustainability and high perceived participant benefit, but low capacity and engagement. In 2006, the prevalence of cardiometabolic syndrome in the US population was approximately 23% 7 ; thus, an estimated 1135 individuals from this demographically-equivalent population may be eligible for the program. Recruitment of only 24 would not measurably improve the health of the organization.
In the context of these limitations, the value of these programs may be conceptualized as shown in Figure 2.
These example programs should not be considered failures, as each was successful in 2 dimensions, but lacked sufficient evolution along the third axis for optimal value. In program 1, for example, the discrete challenge might have served as a springboard to a walking club that would continue to recruit and incentivize members, thereby evolving the program along the sustainability axis. In program 2, the HRA incentive could have been used to motivate participant engagement in risk reduction activities. In the third program, nurse educator hours might have been expanded to service the unmet need.
Individual health and wellness initiatives do not need to perform on all axes if an integrated wellness strategy drives comprehensive success, as a well-designed suite of programs may exist within the “ideal” corner of the cube even though individual programs are not 3-dimensionally complete.
Creating program attributes
Impact
A program must lead to measurable improvement in overall population health or a reduction in risk. In program 2, the HRA aids in risk reduction but would not by itself improve the health of respondents. In fact, a recent study of HRA impact showed only a 3% change in medical office visits and a 4% increase in prescription fills among participants. 8 Impact also requires health or risk improvement for both the individual and the population. For example, a program that improves the rate of medication adherence from 49% to 51% may not be meaningfully impactful. From an individual perspective, change that is not sufficient to alter risk stratum should not improve impact scoring.
Engagement
A sufficient number of individuals must participate to produce a measurable health improvement signal. Valuable programs must have targeted appeal to at-risk individuals. Health promotion engagement theories abound, including the Health Belief Model, the Stages of Change Model, the Theory of Planned Behavior, and others. 9 Each offers a strategy for leveraging an individual's perceptions, enthusiasm, and anxiety about illness and health risk. Social network focus has shown the potential to reduce the prevalence of obesity and smoking, and should receive consideration as part of a health promotion engagement strategy. 10,11 Program developers should use these theories to help overcome participation barriers. Designers also must consider the complex nature of human environments and factor social ecology into their initiatives. 12
Although wellness programs can effectively keep low-risk individuals from changing strata, the greater opportunity likely exists within the moderate-, high-, and extreme-risk groups. Research suggests that wellness program participants tend to be healthier and more concerned with fitness and health matters than nonparticipants. 13 Promotions must be engaging for those with greatest need. Meaningful participation is also critical. Enrollment without commitment to a health or wellness goal cannot be considered successful engagement.
Sustainability
This dimension refers to the persistence of the target health effect. For interventions that lead to durable improvements, program longevity might not be critical. 14 Frequently, however, chronic disease management requires continuation of an effective program. Long-term planning recognizes the likelihood of control rather than cure for chronic health issues, as well as the contextual circumstances that lead to high rates of relapse and recidivism. 15
Sustainability is critical beyond maintenance of gains. A lack of continued progress within a population can lead to regression toward high-risk behaviors. When smoking cessation campaigns lose engagement or impact, for example, the prevalence of tobacco use rises. This dynamic was evident among teens in America from 1991–1997, when the prevalence of cigarette use increased from 24.8% to 27.5%. 16,17
Given the dynamics of an organization's population and the delivery of health and wellness services, achievement on this axis may be the most challenging. Sustainability implies the organization's commitment to propagate a program through continued support. Beyond continuance, however, are other essential sustainability elements. Programs must recruit new participants to succeed long term, and must remain appealing to sustain engagement. In 2007, Novartis Pharmaceuticals Corporation launched a cardiometabolic intervention program called Mission Health. During the initial study period, 217 at-risk participants experienced a significant improvement in blood pressure control, 18 meeting reasonable expectations for impact and engagement. Mission Health continued and the program settled near the “ideal” corner of the wellness cube. By 2010, however, the program's value had waned because of a lack of continued recruitment, innovation, and freshness, which reduced the program's sustainability.
Health promotions and health amenities
Not every health or wellness initiative must exist in the ideal corner of the health cube. Programs that do not excel by 3-dimensional criteria may provide value to an organization. These health amenities can educate, activate, or promote engagement in other health promotions. Their visibility may be an asset to the organization even if they do not directly impact the health or wellness of the population in any measurable way. Amenities could even have an impact on member or employee retention. They may be used to generate a “culture of health.” They may also be important initial steps toward strategically linked programs that achieve success in 3-dimensional terms.
Strategic program integration
Individual health promotion programs do not need to score well in all 3 dimensions if they are part of a strategic bundle. As an example, consider an organization committed to reducing the disease burden of asthma through school-based programs. The organization garners approval for student self-administration of short-acting β-agonist inhalers, and partners with the local physician community to ensure access to care for young asthmatics. School property smoking bans are promoted, and funding is provided for school nurses trained in asthma management. Though each component may not generate a measurable impact, the strategic program linkage may have enormous impact. This scenario is the essence of the Centers for Disease Control's National Asthma Control Program, 19 which demonstrated a 14% decline in childhood asthma hospitalizations during 2000–2007 and 4.2 million fewer missed school days in 2008. 20
The 3-dimensional health matrix may be used when integrating multiple health amenities into single complex health promotions. In that setting, the tool can help identify specific gaps in impact, engagement, or sustainability that could be filled by adding 1 or more customized programs.
Three-dimensional scoring
A quantitative step may be applied to the 3-dimensional model to estimate the program's value and provide a basis to identify opportunities for improvement. Key attributes (as suggested in Table 1) may be valued and scored. In the example provided in Table 2, attributes are weighted, such that the impact, engagement, and sustainability dimensions provide equal input. This assessment format is similar to the quality function deployment tool essential to Six Sigma project management. 21 In Table 2, use of the scoring matrix exposes and quantifies the relative shortcomings of each hypothetical initiative. The on-site condition management program scores highest because of its impact on participants, recruitment success, and the organization's program commitment.
Total scores are calculated as the sum of the attribute cell value x adjusted weight. Note that the strength of association values are provided for illustrative purposes only.
CM, condition management; HRA, health risk assessment; QFD, quality function deployment.
Limitations of the three-dimensional model
The 3-dimensional wellness model presented in this article does not factor program cost into overall value. It also cannot estimate return on investment for health promotions. Nonetheless, 2 basic applications can be easily deduced. First, it is reasonable to select a lower cost program over a more expensive initiative with the same 3-dimensional score. Because scores for the walking challenge and HRA were close, cost is an obvious discriminator. In the former program, the prime expense was the cost of the pedometers. At $5.00 per device, and adding cost for prizes, this program should have been completed for under $10,000, in contrast to the latter program, in which typical incentives ($25–$100) could result in costs as high as $250,000 and may not add incremental value.
Conclusion
Stakeholder groups should consider application of the model, with consideration of the attributes and quantification of 3-dimensional scoring, as an essential planning step for health promotions. This may involve subjective scoring by the planning team or evaluation of a pilot program. Creation of programs that exist in the “ideal corner” should be an aspiration. The 3-dimensional model may be applied to a spectrum of initiatives that endeavor to improve population health through behavior change. Use of 3-dimensional modeling may lead to identification of programs of limited value that, on linear analysis, had seemed designed for success. Low scoring programs may be rejected, modified, or characterized as health amenities rather than health promotions. The model also may be used to integrate isolated health amenity-type programs into a single higher value health promotion. Three-dimensional analysis also allows managers to monitor the impact, engagement, and sustainability of ongoing promotions, and make corrections whenever lapses are detected.
Footnotes
Disclosure Statement
Dr. Goldsmith and Ms. Harris are employees of Novartis Pharmaceuticals Corporation, the funder of this study. They declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received the following financial support for the research, authorship, and/or publication of this article: This work was supported by Novartis Pharmaceuticals Corporation.