
Abstract
Low back pain (LBP) has received considerable attention from researchers and health care systems because of its substantial personal, social, work-related, and economic consequences. A narrative review was conducted summarizing data about the epidemiology, care seeking, and utilization patterns for LBP in the adult US population. Recommendations from a consensus of clinical practice guidelines were compared to findings about the current state of clinical practice for LBP. The impact of the first provider consulted on the quality and value of care was analyzed longitudinally across the continuum of episodes of care. The review concludes with a description of recently published evidence that has demonstrated that favorable health and economic outcomes can be achieved by incorporating evidence-informed decision criteria and guidance about entry into conservative low back care pathways. (Population Health Management 2013;16:390–396)
Introduction
T
To achieve value for the current levels of investment in care, the factors that contribute to variation in costs and quality must be addressed. In fact, experts have concluded that the quality and efficiency of the US health care system could be improved by approaches that address overuse, and inappropriate or ineffective use of care—the chief factors contributing to the current high levels of expenditures, inefficiency, and waste. 3
A previous article analyzed current practices regarding the use of coronary stents in the chronic stable angina patient. 4 Musculoskeletal disorders represent another diagnostic class that, while usually not life threatening, results in a high prevalence of morbidity and significant societal burden. 5 Low back pain (LBP) management in particular has been linked to inefficiency and waste. 6 This is likely related, in part, to the growing list of treatment approaches recommended for conservative care (pharmacologic and non-pharmaceutical options) and the difficulty in determining the best option for each patient. 7
Although useful in assisting practitioner and patient decisions about appropriate health care for specific clinical circumstances, 8 clinical practice guidelines (CPGs) are not sufficient to maximize effectiveness and cost-effectiveness at the individual level (ie, targeting specific care). 9 The clinical appropriateness of health care services at the individual level can be assessed by considering the patient's clinical characteristics, the relevant risk factors, the setting or health care provider type, the severity of the illness, and the specific requirements for a procedure (eg, availability of the service). 9
The purpose of this article is to discuss the challenges associated with management of LBP and describe an evidence-informed process to effectively and cost-effectively integrate individual patient conservative care for LBP with appropriate population-based recommendations found in high-quality CPGs.
Back Pain—An Overview
Pain affects millions of Americans; contributes greatly to national rates of morbidity, mortality, and disability; and is rising in prevalence. 10 Back pain is the most common physical condition for which patients visit their doctor, 6 and surveys reveal that over one quarter of adults (26%) report LBP in the past 3 months. 11 The lifetime prevalence of LBP is approximately 85% (probably closer to 100% of adults). 12
A substantial majority of those who suddenly develop LBP improve quickly with or without professional care. However, recurrences and flare-ups are common, and individuals with chronic LBP tend to show a more persistent course. 13 Thus, LBP is best viewed as a recurrent disorder that can occur anytime in a person's life and fluctuates between no/mild pain to debilitating pain. 12 Important prognostic factors are related to the back pain episode, individual and psychological characteristics, as well as the work and social environment. 13
About 1 in 2 people who experience LBP seek health care during an episode. 14 Care seekers tend to be those who have high levels of disability, 15 and/or who are experiencing more severe pain, more distal pain, work-related pain, and those who are more fearful about what the pain might mean. 14 Clinicians most commonly consulted for back pain in North America are chiropractors, general medical practitioners, and orthopedists. 14 When initial care seeking is calculated on an episodic basis, chiropractors and primary care physicians (PCPs) are by far the provider types most commonly consulted (D. Elton, unpublished data, 2010) (Figure 1). About 85% to 90% of individuals who seek care are assessed as having nonspecific or ordinary LBP (ie, not associated with a specific cause including serious pathology). 16
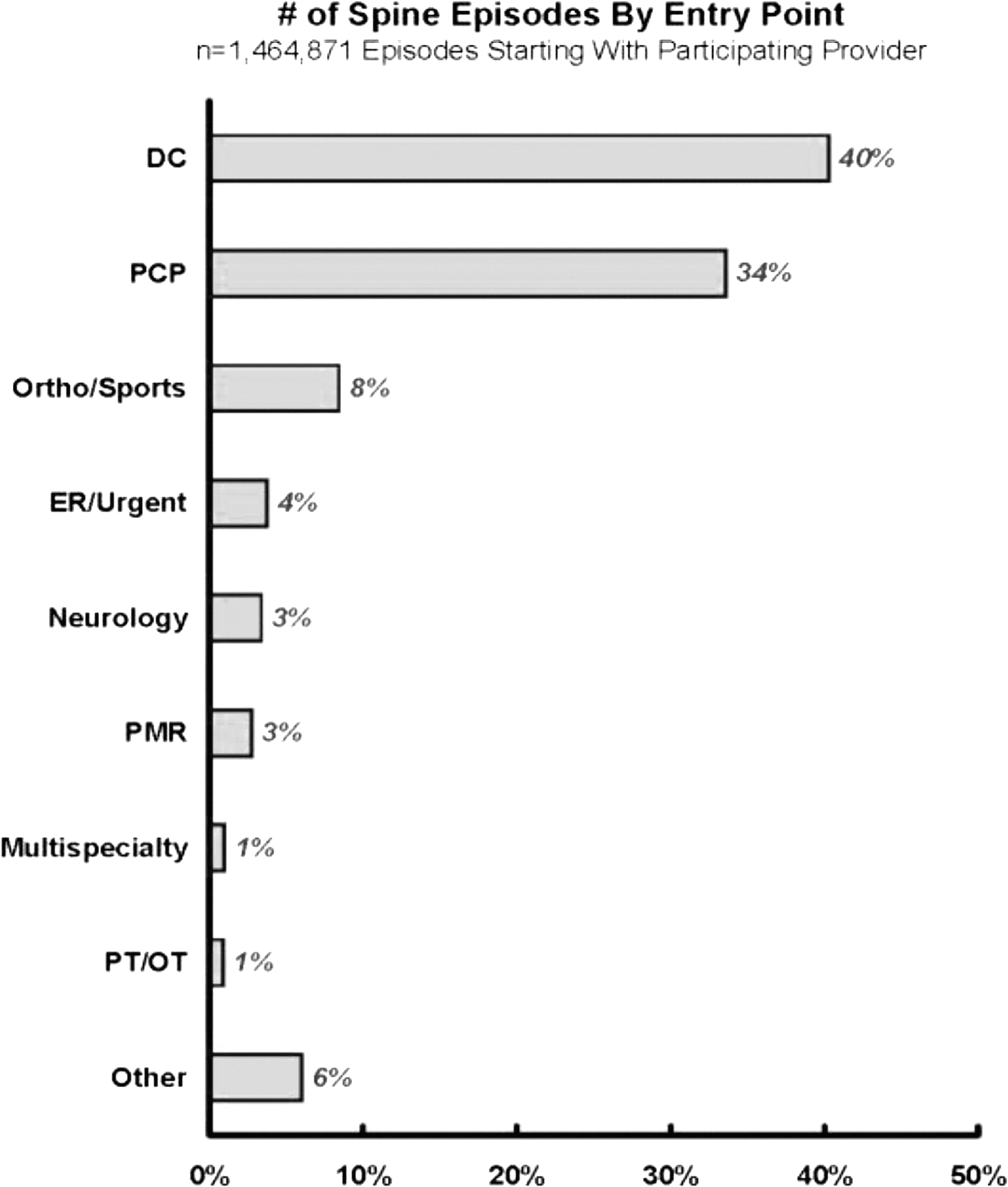
Number of spine episodes by entry point. Source: Elton D., et al. OptumHealth Episode Treatment Group Analysis, 2010. DC, Doctor of Chiropractic; PCP, primary care physician; ER, emergency room; PMR, physical medicine and rehabilitation specialist; PT/OT, physical therapist/occupational therapist.
Increasingly, back pain has become a financial concern because of the high associated direct and indirect costs of testing and treatment. Cost estimates vary, but the most recent estimates (2008) put care related to back pain at $86 billion in incremental health care costs. 17 A 49% increase in the number of patients seeking spine-related care (from 12.2 million in 1997 to 18.2 million in 2006) was the largest contributing factor to increased outpatient expenditures. 18 Adding to the problem is a sharp increase in the number of investigations and interventions performed related to back pain, including imaging, injections, surgical procedures, implantable devices, and medications. These services have value for some patients, but it appears that they are being used in areas beyond those for which data support an improvement in outcomes. 19
Despite the fact that the proportion of office visits has changed little since 1990, there has been remarkable (307%) growth in the use of lumbar magnetic resonance imaging (MRI) in the Medicare population from 1994 to 2004. 21 Using current guidelines as a baseline, one third to two thirds of spinal computed tomography (CT) imaging and MRI may be inappropriate. 19
Use of opioid prescriptions also has increased by 108% from 1997 to 2004 resulting in a 423% inflation-adjusted increase in expenditures. 19 The number of spinal injections grew more than 200% over the same time period, and spine surgery rates have risen over 200% from 1997–2004. Spine imaging rates vary across geographic regions, and the rate of surgery is highest where imaging rates are highest. Moreover, the evidence shows that despite newer technologies, higher spine surgery rates can be associated with worse outcomes. 19
The Challenge of Low Back Pain
Patient “care-seeking” decisions for LBP initiate a cascade of management services and processes representing clinical pathways that may or may not equate to the most appropriate intervention for individuals.
20
Treatment choices can be influenced by patients depending on the types of health care providers they choose to consult, which in turn influences the types of treatments received.
21
In many instances, circumstances require that patients navigate LBP management on their own.
22
Fundamental challenges include: • Provider Type—People who develop LBP and wish to seek care are first required to select a health provider. To a large degree, the tests and services provided to individuals are dependent upon the health care professional type from whom a patient first seeks care.
21,23
More than 20 different health care provider types (eg, physicians, allied health, complementary and alternative medicine) may be considered when seeking treatment for LBP.
7
• Treatment Options—The challenge of weighing alternate treatment options for LBP does not end once the choice of a specific type of health provider is made. A partial list of treatment options available to a person with LBP includes more than 200 different medications, therapies, injections, products, or procedures.
7
It is difficult for any health care provider involved in the management of LBP to understand the relative benefits and harms of each intervention at a level that is sufficient to advise his or her patients. • Individual Patient Variations—The selection of the correct intervention for LBP is further complicated by differences in baseline prognoses among patients seeking care.
24
An important consideration when commencing an episode of care is the “targeting” of interventions that address individual risk factors.
25
Review of Clinical Practice Guidelines for Low Back Pain
A number of CPGs have been published recently that focus on the management of acute and/or persistent (chronic) common (nonspecific) LBP. 26 –35 Typically, these guidelines commence with patient decisions to enter primary care management. They describe recommendations for diagnostic assessment, treatment options (eg, self-care, pharmacotherapy, non-pharmacologic interventions), and indications for referral for testing and specialist care.
Synthesized recommendations from these CPGs provide a consistent set of “quality” recommendations concerning processes of care. 36,37,38 Specifically, 10 CPGs sponsored by 10 different international organizations during the past decade were compared and summarized in a recent text. 13 Both acute and chronic LBP complaints were represented, providing an overview of the best available evidence to inform clinical judgment. Although each new CPG may emphasize a distinct aspect of care or a specific subgroup, the collective recommendations have been largely consistent, with only minor changes throughout the years based on new evidence. 17,30
Among these guidance documents, there was general agreement on 5 main sequential goals when conducting an assessment of LBP: 1. Ruling out potential serious pathology (eg, infection). 2. Ruling out specific causes of LBP (eg, spinal stenosis). 3. Ruling out substantial neurological involvement. 4. Evaluating the severity of symptoms and functional limitations. 5. Identifying risk factors for chronicity.
13
For the 85%–90% of individuals assessed as having nonspecific or ordinary LBP, CPGs recommend against routine imaging (eg, radiography, CT scan, MRI), stronger opioid analgesics, and injection procedures (eg, epidural, facet, soft tissue). Instead, the consensus of the guidelines suggests that patients with acute, nonspecific LBP should: • be reassured of a good prognosis, • be educated in self-care, • remain active, • use over-the-counter medications (eg, acetaminophen, nonsteroidal anti-inflammatory drugs) or spinal manipulation or both as a first line of symptom control.
30
Other physical modalities (eg, traction, ultrasound, transcutaneous electrical nerve stimulation) and supports/braces are not recommended by CPG developers. Supervised exercise and, to a lesser degree, behavioral modification and/or acupuncture therapies also are recommended for individuals who have chronic or persistent LBP. 38
In summary, the goal of CPGs is to provide algorithms whereby busy clinicians can quickly determine/identify “best practice” alternatives for their patients that are based on careful evaluation of the evidence. 39 Ideally, CPGs focus on common problems with significant morbidity or mortality. Back pain fits this ideal. Whether CPGs are worth the resources that continue to be dedicated to them remains a matter of speculation. 40
Current Clinical Practices
When followed by providers and patients, evidence-based guidelines for the clinical management of LBP have been associated with better functional outcomes, reduced health care utilization, and lower health care costs. 41,42 Yet there is a strong body of evidence suggesting a low level of adherence to guidelines in daily clinical practice. 43,44 Overall adherence to guideline-based care by PCPs has been recorded at 65%, a rate that has remained unchanged despite attempts to increase implementation of evidence-based care. 43 For acute nonspecific LBP, 65% of the cases receive recommendations for imaging studies despite clear guidance that this is not routinely indicated. 45 Only half of LBP patients who see a PCP receive a recommendation to remain active. 45 Manipulation, which is supported by most guidelines, is recommended by PCPs in only 2% of the acute nonspecific LBP cases. This gap in adherence to evidence-based practice recommendations by clinicians has become popularly known as the “know-do gap”—the gap between what is known and what is done in practice. 46,47
These national trends are contextualized by data that describe the timing of services received by patients seeking care for spinal pain in the “real world” of clinical practice. A recently published analysis of nationwide private insurer claims covering more than 8 million lives revealed the front-loading of treatment expenditures, even among patients with nonspecific LBP.
17
“Contrary to clinical guidelines, many patients with low back pain start incurring significant resource use and associated expenses soon after the index [initial] diagnosis.”
17
p.623 The analysis showed: • Diagnostic and treatment interventions were common in the first month. • More than 32% of patients with LBP received X-rays, with at least 50% receiving them on the same day as the initial diagnosis. • Second-line medication was prescribed for 69.4% of patients, with at least 50% of those patients filling the prescription within 8 days of the initial diagnosis. • Opioids were prescribed for 41.6% of patients, and more than half of the prescriptions were filled within 25 days of the initial visit. • The median number of days to surgery was 90 for all those having surgery. Surgery was performed within 54 days (median) of the initial diagnosis for those individuals not classified as having chronic LBP (>3 months duration).
The impact of nonadherence to evidence-based CPGs has been measured by analyzing episodes of care—a method that provides longitudinal data across the entire pathway of care (eg, total number of health care providers seen by the individual throughout the episode of care, the diagnostic tests performed, the medication prescribed). 48 As demonstrated by data synthesized by Elton (Figure 1), individuals with similar risk profiles who begin their care pathway with a chiropractor or PCP see fewer total health care providers throughout the overall episode of care than do individuals who initially consult an orthopedic specialist, physical medicine/rehabilitation specialist, or physical/occupational therapist (Table 1). Individuals who commence an episode of care with a chiropractor or PCP are less likely to undergo imaging and are prescribed fewer medications. Also, they are more likely to receive first-line management options as recommended by CPGs.
PCP, primary care physician; Ortho=orthopedist; ER, emergency room; PM&R, physical medicine and rehabilitation specialist; PT, physical therapist; OT, occupational therapist.
These findings are similar to recently published data. A 2-year retrospective claims analysis of BlueCross BlueShield TN members presenting with LBP employed a similar episode treatment grouping methodology. “Paid costs for episodes of care initiated with a DC [chiropractor] were almost 40% less than episodes initiated with an MD [physician]. Even after risk adjusting each patient's costs, we found that episodes of care initiated with a DC were 20% less expensive than episodes initiated with an MD.” 49
The current management of back pain has led to increased resource usage without a corresponding improvement in outcomes. In a nationally representative population sample (Medical Expenditure Panel Survey), trends in health care expenditures from 1997 to 2005 were calculated for adults who self-reported spine problems (neck pain and LBP). 50 Spine-related expenditures were found to have increased substantially from 1997 to 2005 without evidence of corresponding improvement in self-assessed health status, functional disability, work limitations, or social functioning.
These findings about the current state of clinical practice for spine-related disorders provide substance to the assertion that we need to rethink frontline care for back pain. 23
Patient-Centered Conservative Care
Decision criteria and guidance about entry into conservative LBP care pathways represent an opportunity to advance the quality and delivery of health services. The choice of initial health care provider matters when it comes to spine-related disorders. The variable impact of “first provider seen” is greatest for the 85%–90% of health care consulters who have “nonspecific” spine-related pain. 24 For these patients, guidelines highlight the importance of assessing a broad range of potential influences on prognosis including fears and anxieties about pain, physical limitations related to pain, mood, motivation, and work situation. 29,32,35
Previous authors have postulated that targeting specific back pain interventions for particular subgroups of patients holds great potential for boosting their effectiveness. 51,52 “However, this is often difficult to do in practice and, until recently, no validated tool has existed to inform clinicians or others about the risk status of individual patients.” 53 The STarT Back Screening Tool (SBST), developed by researchers at Keele University (United Kingdom) with funding from Arthritis Research UK, can be administered prior to initiating treatment. This tool presents an opportunity to fill a serious knowledge gap in the delivery of health services by incorporating evidence-informed decision criteria and guidance about entry into conservative low back care pathways (Figure 2).
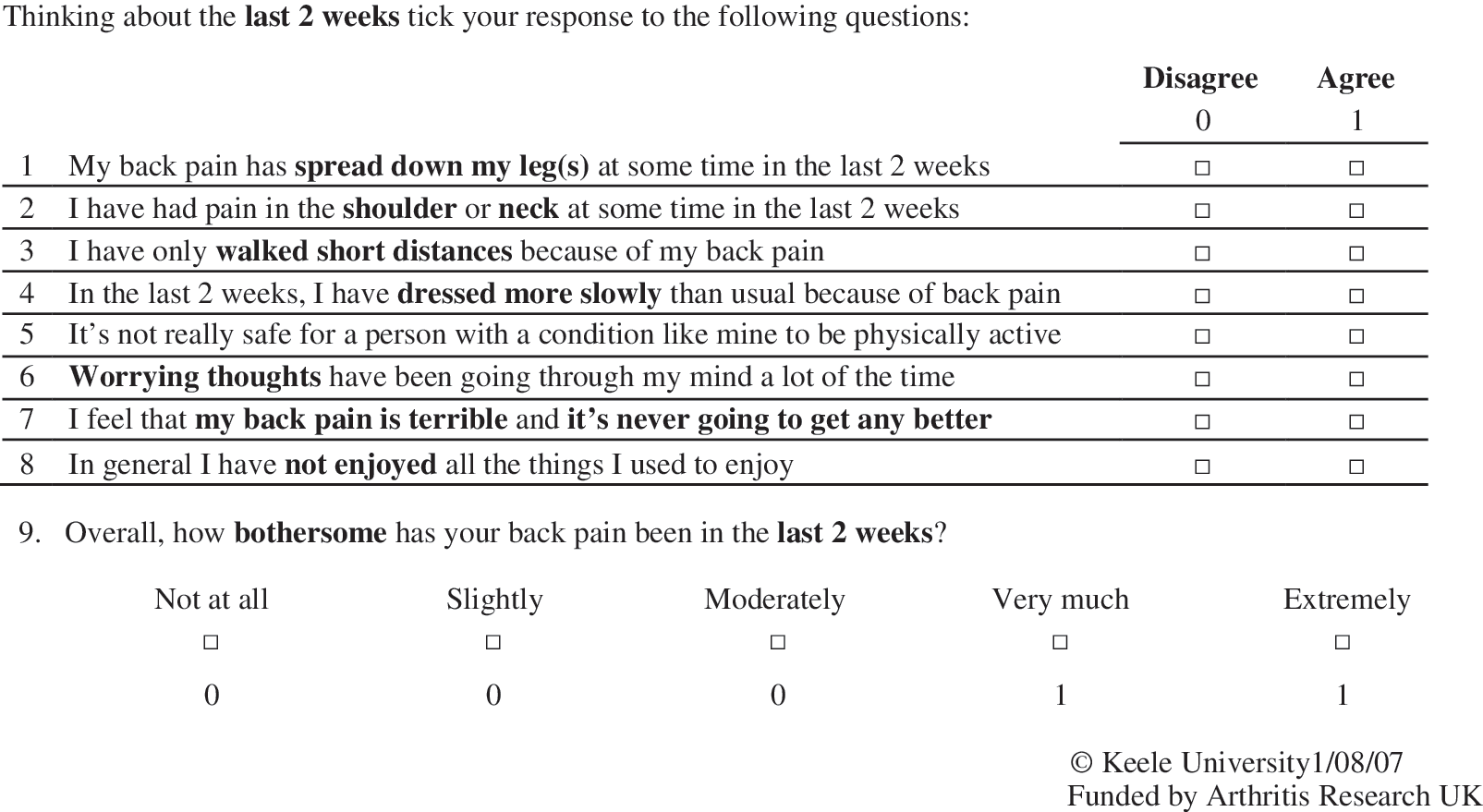
The STarT Back Screening Tool.
This classification-based model for the management of LBP has been shown to improve clinical outcomes and address the inappropriate utilization of services. 25 It is predicated on the understanding that not all patients entering a care pathway for nonspecific LBP are the same. Primary care data suggest that, for first contact settings such as general practitioner consultations, approximately 55% of patients with nonspecific LBP are at low risk of poor outcome (ie, patients who are likely to do well irrespective of treatment); 33% are at medium risk; and 12% are at high risk. 24
Appropriate individualized care management may be facilitated when the first health care provider seen is best equipped to administer the treatment most likely to benefit a particular patient. 23 Using the SBST approach, individuals at “low risk” usually benefit most from receiving reassurance and advice, which can be rendered by PCPs, nurses, or health coaches (Table 2). The treatment options recommended for persons at “medium risk”—manual therapy (eg, manipulation) and specific exercises—are most typically provided by chiropractors and physical therapists. Optimally, the management of patients at “high risk” should be overseen by physical therapists or chiropractors, who are skilled in providing behavioral therapy in addition to the same strategies targeted for patients at medium risk. 54
Hill J, DGT Whitehurst, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet 2011;378:1560–1571.
ADLs, activities of daily living; OTC, over-the-counter medication; RTW, return to work; CBT, cognitive behavioral therapy; SBST, STarT Back Screening Tool.
This framework has demonstrated “proof of principle” in a recently published clinical trial. 25 “The results showed the SBST approach changes the pattern of management and referral in a way that is more appropriate for patients' needs.” 53 When compared to current best practice, use of the SBST tool along with targeted treatments increased efficiency, improved clinical outcomes, and reduced health care costs.
Almost half of the “low-risk” patients in the usual care group, who typically respond well to self-care management, were referred for supervised physical therapy. In contrast, more than 90% of those allocated to the SBST group were provided with advice and education to support self-care management. Conversely, more than a third of patients likely to benefit from supervised therapy (medium- and high-risk categories) in the usual care group did not receive referrals. Virtually all those patients in the SBST group, who were similarly categorized, were referred for therapy.
Overall, 75% of the SBST group were referred for physical therapy vs. 60% of controls. Despite this greater rate of referral, the costs over 12 months were about 13% less for the SBST group. Savings were attributed in large part to more efficient utilization. The SBST referral group averaged 4.2 visits, while the usual care group received a mean of 5.1 visits.
At 4 and 12 months, the SBST group demonstrated superior patient-important outcomes compared to the “usual care” control group at both 4 and 12 months. Adjusted mean changes in disability scores were significantly better in the SBST group than in the control group at 4 months and at 12 months. The patients in the SBST group were significantly more likely to be satisfied with treatment and lost fewer days of work. Importantly, those individuals in the low-risk category who did not receive referral for therapy did as well or slightly better than those in the same risk category who did receive a course of physical therapy.
Conclusion
The current state of the conservative management of LBP is summarized in this narrative review. Current clinical practice has been ineffective in meeting the challenge of consistently adhering to the recommendations of modern evidence-based guidelines. It is not surprising that patient “care-seeking” decisions for LBP initiate a cascade of interventions that may or may not represent the most appropriate management for individuals.
One opportunity to facilitate compliance with clinical guidelines is to assure that the first health care provider seen is best able to administer the treatment likely to benefit a particular patient. This can be achieved, in part, by implementing a triage approach for the early referral of well-defined subgroups of patients into appropriate clinical pathways. Recently published evidence supports this premise. The STarT Back subgrouping and targeted treatment approach has been shown to significantly improve patient outcomes (effectiveness) and is associated with substantial economic benefits (efficiency) compared with current usual practice. 24
Footnotes
Author Disclosure Statement
Drs. Kosloff, Elton, and Shulman are employees of Optum Health Care Solutions. Optum Health Care Solutions is currently contracted with the Jefferson School of Population Health to develop programs around overutilization in health care. Ms. Clarke, Dr. Skoufalos, and Ms. Solis are employees of the Jefferson School of Population Health, which has been contracted to collaborate with Optum Health Care Solutions on programs regarding health care overutilization.
The authors received no financial support for the research, authorship, and/or publication of this article.