
Abstract
Objective:
High-intensity laser therapy (HILT) combined with photobiomodulation therapy (PBMT) using a diode or CO2 laser was administered after extraction of the left first molar in rats. Effects on socket preservation (preservation of the alveolar bone and healing time after extraction) were evaluated histopathologically.
Background:
Irradiation using a diode or CO2 laser has been shown to hasten wound healing, but the effects remain controversial.
Methods:
Five-week-old male Wistar rats that underwent extraction of the left maxillary first molar were divided into three groups: diode laser irradiation (diode group), CO2 laser irradiation (CO2 group), and no laser irradiation (control group). HILT (27 J) was performed immediately after tooth extraction to enhance blood coagulation, followed by PBMT (0.7 J) 1 day later to enhance healing. Tissues, including the extraction socket, were removed en bloc 3, 5, 7, 10, and 21 days postextraction to determine the morphological characteristics of wound healing and the distribution of myofibroblasts involved in scar formation.
Results:
In the diode and CO2 groups, new bone formation and cancellous bone maturation were observed at an early stage of wound healing. The number of myofibroblasts was significantly lower in the laser treatment groups than the control (p < 0.001), and both treatment groups had a significantly higher alveolar crest height (p < 0.01), with almost no concavity in the mucosa of the extraction wound.
Conclusions:
Combined HILT and PBMT following tooth extraction hastened wound healing and preserved alveolar crest height, suggesting a role in socket preservation.
Introduction
Loss of alveolar bone height can often be caused by preexisting periodontal disease. For example, smoking exacerbates loss of attached gingiva, gingival recession, and loss of alveolar bone height due to vasoconstriction in periodontal tissue by nicotine. 1 –3 In addition to periodontal disease, there are various factors associated with loss of alveolar bone height such as tooth impaction or the presence of supernumerary tooth, 4 oral injury, oral disease, and oral surgery for tumors of the jaw. 5 Another such factor is tooth extraction. Although tooth extraction is one of the most frequent procedures in dental practice, including for pre-prosthetic preparation, it has a high likelihood of causing loss of the alveolar crest height.
Previous studies on changes in alveolar bone after tooth extraction have indicated that most of the decrease in alveolar bone height occurs within 3 months after extraction. 6,7 In addition, Schropp et al. have reported an average decrease of 3–5 mm in the bone width of the alveolar ridge within 6 months after tooth extraction, of which 80% occurred within 3 months after extraction, and they found an average decrease of 50% within 12 months after extraction. 8 Furthermore, Huebsch et al. have reported that the difference in the position of blood clot formation in the extraction socket affects the height of new bone formation. 9
With the hemostatic methods typically used after tooth extraction (i.e., compression and suturing), blood is not retained in the extraction socket, leading to considerable outflow of blood and eventual loss of alveolar bone height. In this way, worsened condition of alveolar bone leads to difficulty in occlusion and long-term maintenance of prosthetic function. Thus, preserving alveolar crest height, together with rapid wound healing after tooth extraction, is essential. This is the concept behind socket preservation.
Currently, autologous bone grafting, 10 using a bone filler or a collagen sponge, 11 is performed for socket preservation. This procedure effectively preserves the blood clot in the extraction socket and offers coverage with osteoanagenesis-inducing substances. However, favorable outcomes are not necessarily achieved, probably due to infected granulation tissue and chronic residual inflammation in the socket, infection after bone or artificial bone grafting, and incomplete substitution of bone with synthetic material. 12,13 Thus, thorough curettage of the socket, sufficient bleeding from the socket wall, and good preservation of the blood clot are essential. Laser irradiation to hasten wound healing and achieve reliable retention of blood in the extraction socket is reported to minimize alveolar bone resorption in the clinical setting. 14,15
The U.S. Food and Drug Administration (FDA) has guidelines for the use of lasers in dentistry, wherein the efficacy of laser irradiation after tooth extraction, namely, “coagulation of extraction sites,” is mentioned. 16 Two types of lasers are recommended: diode and carbon dioxide (CO2) lasers. Several clinical studies have evaluated laser irradiation after tooth extraction, but its utility remains unclear because objective evaluation was not possible due to differences in underlying disease and periodontal conditions.
We have been studying changes in the wound healing process induced by high-intensity laser therapy (HILT) that protects the wound surface through coagulation, 17,18 and photobiomodulation therapy (PBMT) that activates tissue 19 –22 using a CO2 laser, 23 and confirmed the presence of numerous osteoclasts with rapid and specific new bone formation early in the socket wound healing process. In contrast, other groups have reported accelerated wound healing in the extraction socket and suppressed scar formation in granulation tissue after postextraction PBMT using a tissue transmission-type laser. 24 –30 However, the laser irradiation conditions used in these studies did not represent conditions used in the clinical setting, precluding evaluation of clinical efficacy of postextraction laser irradiation.
In this study, we used diode and CO2 lasers for HILT combined with PBMT after tooth extraction in rats, in a manner that mimics the clinical procedure, and performed histopathological examination of the extraction sockets to examine the morphology of healing in alveolar bone and the proliferation of myofibroblasts involved in early scar formation.
Materials and Methods
Five-week-old male Wistar rats (weight, 130–150 g) were used. Three rats were housed in one cage with free access to food (CLEA Rodent Diet CE-2; CLEA Japan, Inc.) and tap water. The room was maintained at 24 ± 2°C and 50 ± 5% humidity with 12-h light/12-h dark cycles. Rats were divided into three groups depending on postextraction treatment: a group treated with no laser irradiation (control group); a group treated with a combination of HILT and PBMT using a diode laser (diode group); and a group treated with a combination of HILT and PBMT using a CO2 laser (CO2 group). The term “laser treatment groups” is used to describe the diode group and the CO2 group collectively. Observation time points were days 3, 5, 7, 10, and 21 postextraction. A total of 90 rats, 6 at each observation time point, were examined in this study.
Rats were anesthetized by intraperitoneal administration of pentobarbital sodium and subjected to extraction of the left maxillary first molar using rat-use elevator and mosquito forceps. Extraction sockets were compressed with dry cotton balls to stop bleeding in the control group, while coagulation by HILT without compression hemostasis was performed in the laser treatment groups. The following day, the sockets were disinfected with the benzalkonium derivative Germitol® in all groups, and PBMT was performed in the laser treatment groups (Fig. 1).
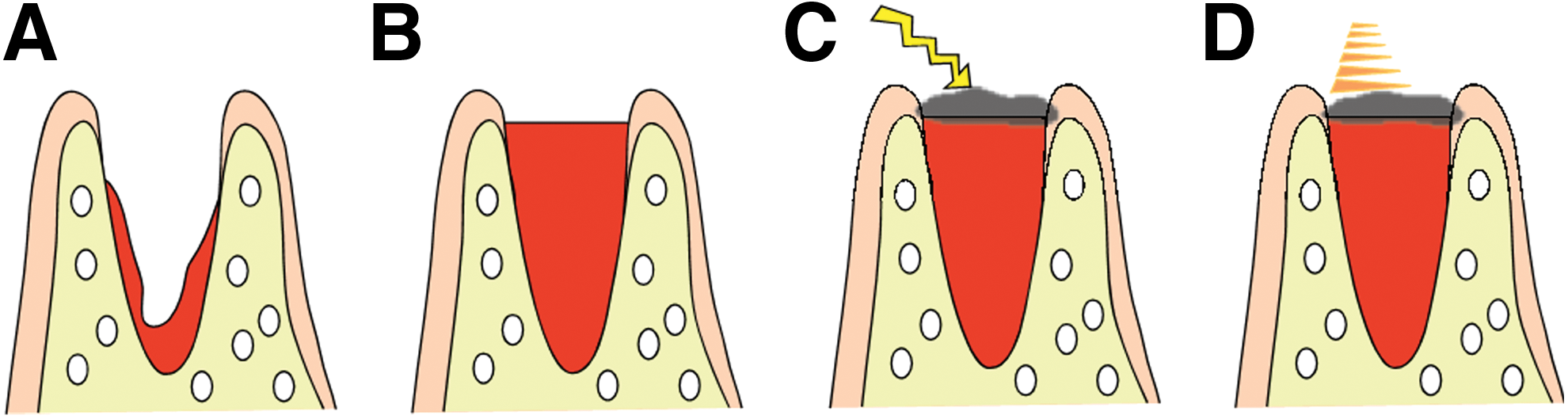
Laser treatment protocol.
Lasers used and detailed irradiation conditions are shown in Tables 1 –3.
Laser Device Specifications
High-Intensity Laser Therapy Irradiation Conditions
Photobiomodulation Therapy Irradiation Conditions
Σ-mode uses an ultrashort pulse width to increase peak power during irradiation, thereby enabling photobiomodulation.
Calculated using the joule conversion table for PanalasCO5Σ.
Histopathological analysis
The extraction socket with the surrounding tissue was removed en bloc from each rat after a lethal dose of the anesthetic and fixed in 4% paraformaldehyde for 48 h. After 3-week decalcification in 10% ethylenediaminetetraacetic acid (EDTA) followed by dehydration using an alcohol gradient, tissue samples were embedded in paraffin. Consecutive sagittal sections (4 μm thick) were then prepared using a microtome and subjected to hematoxylin–eosin staining.
Morphometric analysis
We counted the numbers of osteoclast-like cells in the extraction socket wall on day 3 postextraction, measured bone volume (BV) of extraction sockets on day 7 postextraction, 25 and measured the height of the alveolar crest on day 21 postextraction, 30,31 which is when the formation of trabeculae of alveolar bone was considered to be complete. The detailed measurement procedure is shown in Fig. 2A–C.
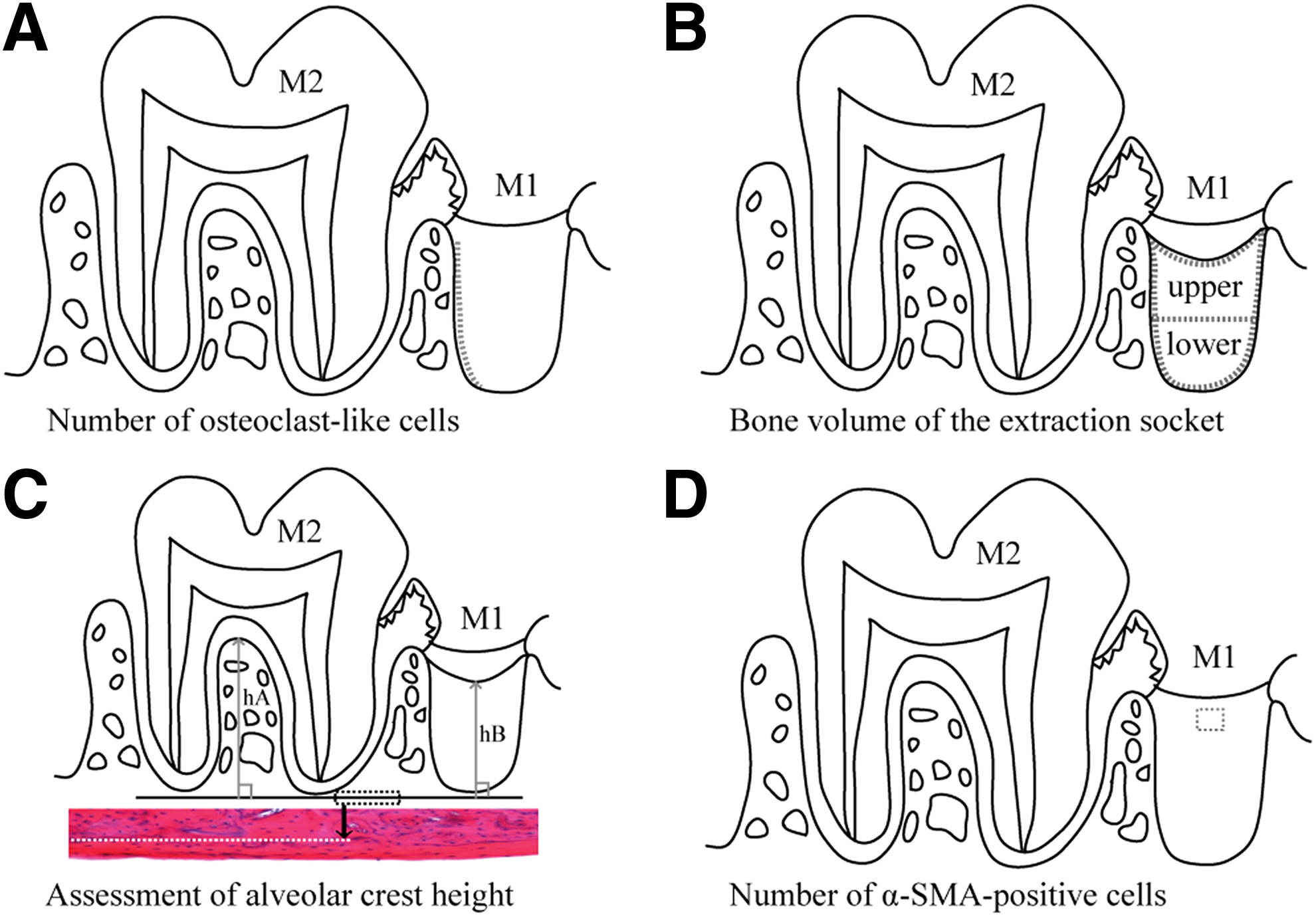
Morphological measurement methods.
Immunohistological observation and measurements
Proliferation of myoblasts involved in early scar formation on day 3 postextraction was examined using anti-human α-smooth muscle actin (SMA)-monoclonal antibody (Clone1A4 N1584; DAKO, Tokyo, Japan) as the primary antibody. Consecutive sagittal sections were incubated with a 1:50 dilution of primary antibody at room temperature, counterstained with Mayer's hematoxylin solution, and observed.
The detailed measurement procedure for counting the number of α-SMA-positive cells is shown in Fig. 2D. Images were scanned using a digital microscope (VZ-9000; Keyence Co., Ltd., Osaka, Japan) and analyzed using Scion-image software (Scion Corporation, Frederick, MD). A coauthor of this study performed blinded measurements. Results are shown as the mean ± standard deviation. Fisher's exact test (STATISTICA; StatSoft, Tulsa, OK) was used for statistical significance (p < 0.05).
The study protocol was in compliance with the Osaka Dental University Guidelines for Animal Experiments (approval no.: 18-01008).
Results
Histopathological and morphometric analyses
Day 3 postextraction
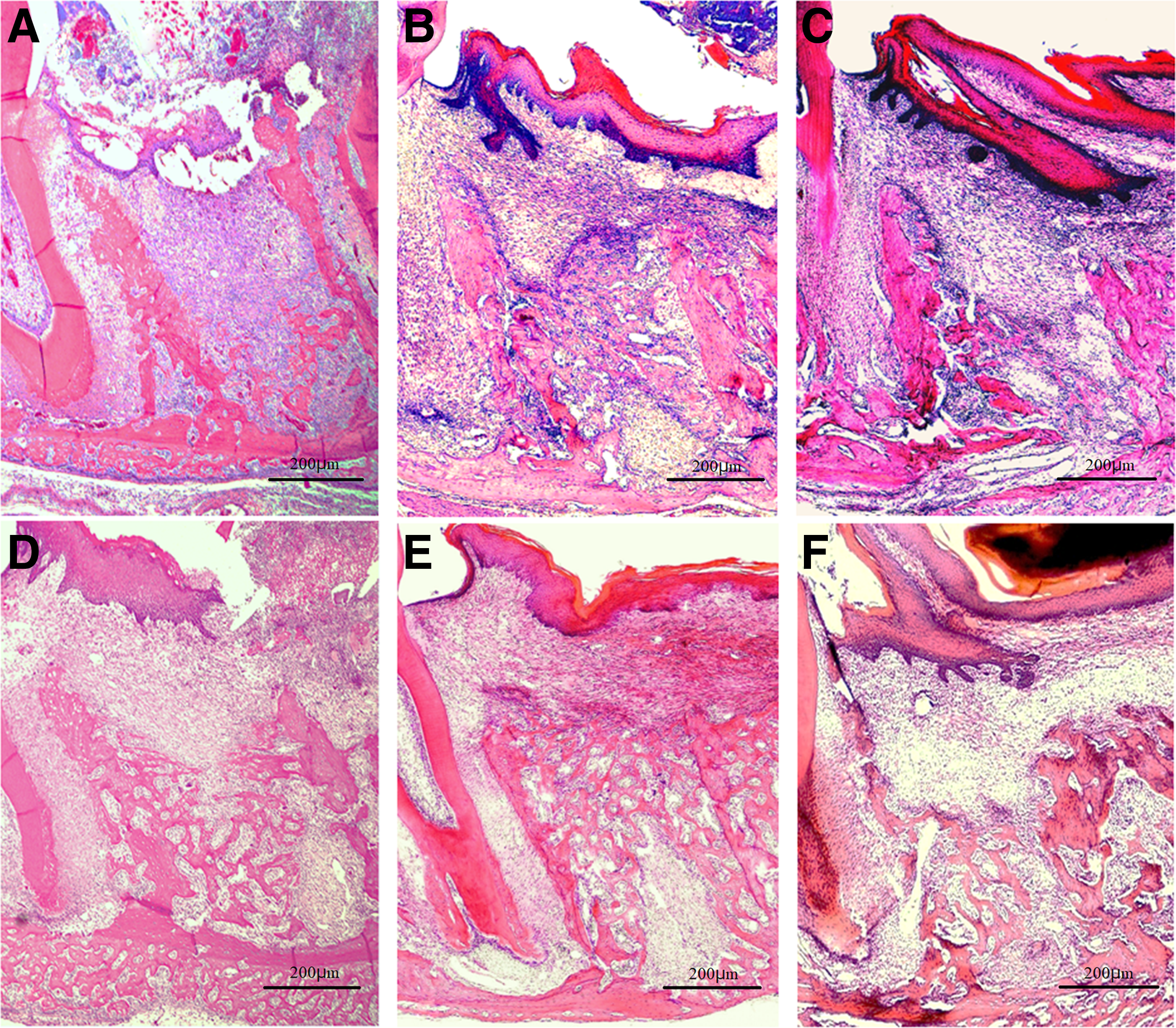
Sockets were almost completely filled with a blood clot in the control group, while the progression of organization from the socket walls was observed in the laser treatment groups (Fig. 4A–C). Organization from the socket fundus was also observed in the diode group. Magnified views of socket walls showed few osteoclast-like cells in the control group (8.737 ± 1.601) and the diode group (9.203 ± 1.336), but many osteoclast-like cells in the CO2 group (12.783 ± 2.901) (p < 0.01; Fig. 3A), and revealed findings indicative of active bone resorption in the CO2 group (Fig. 4D–F).
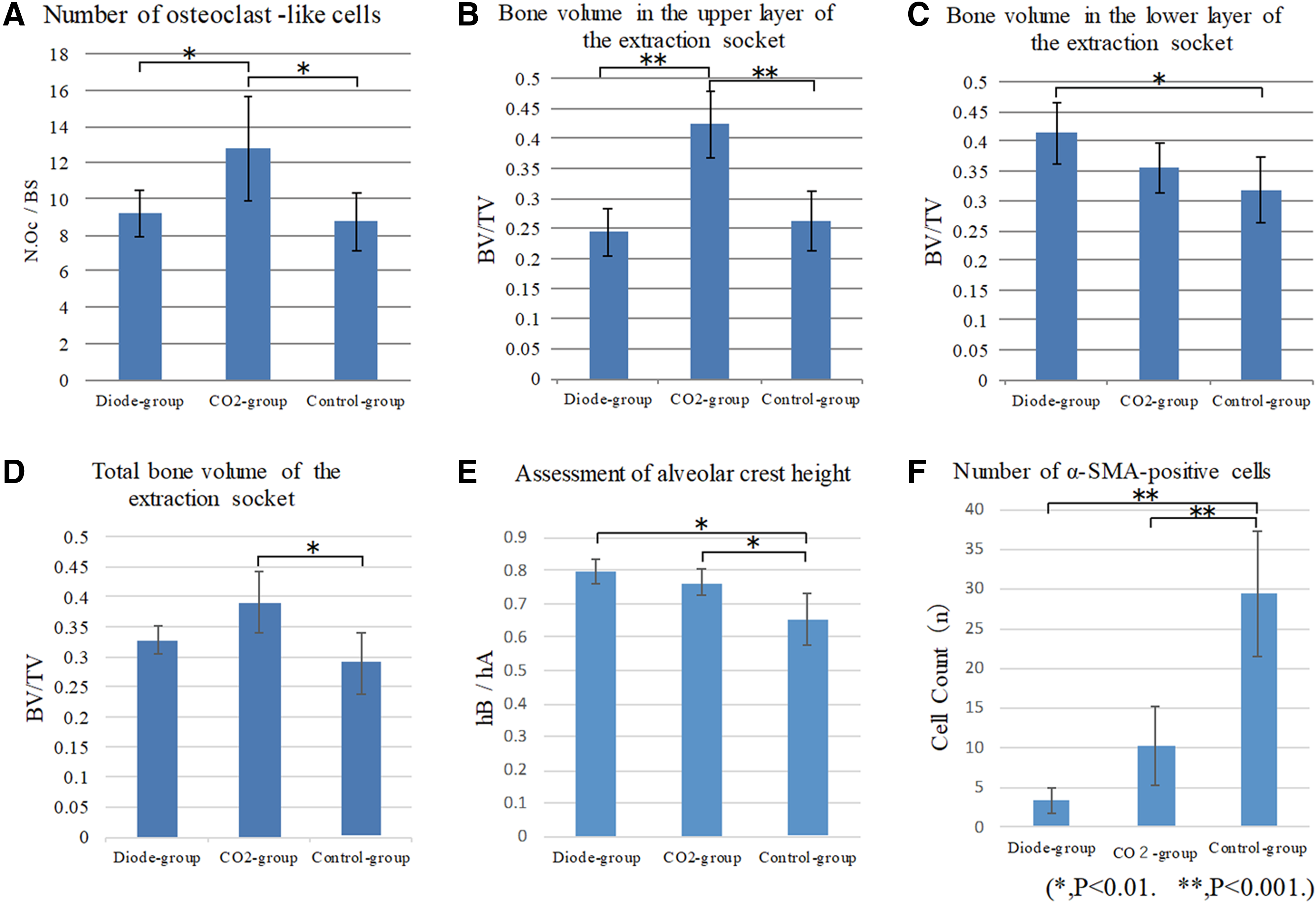
Morphological measurement results.
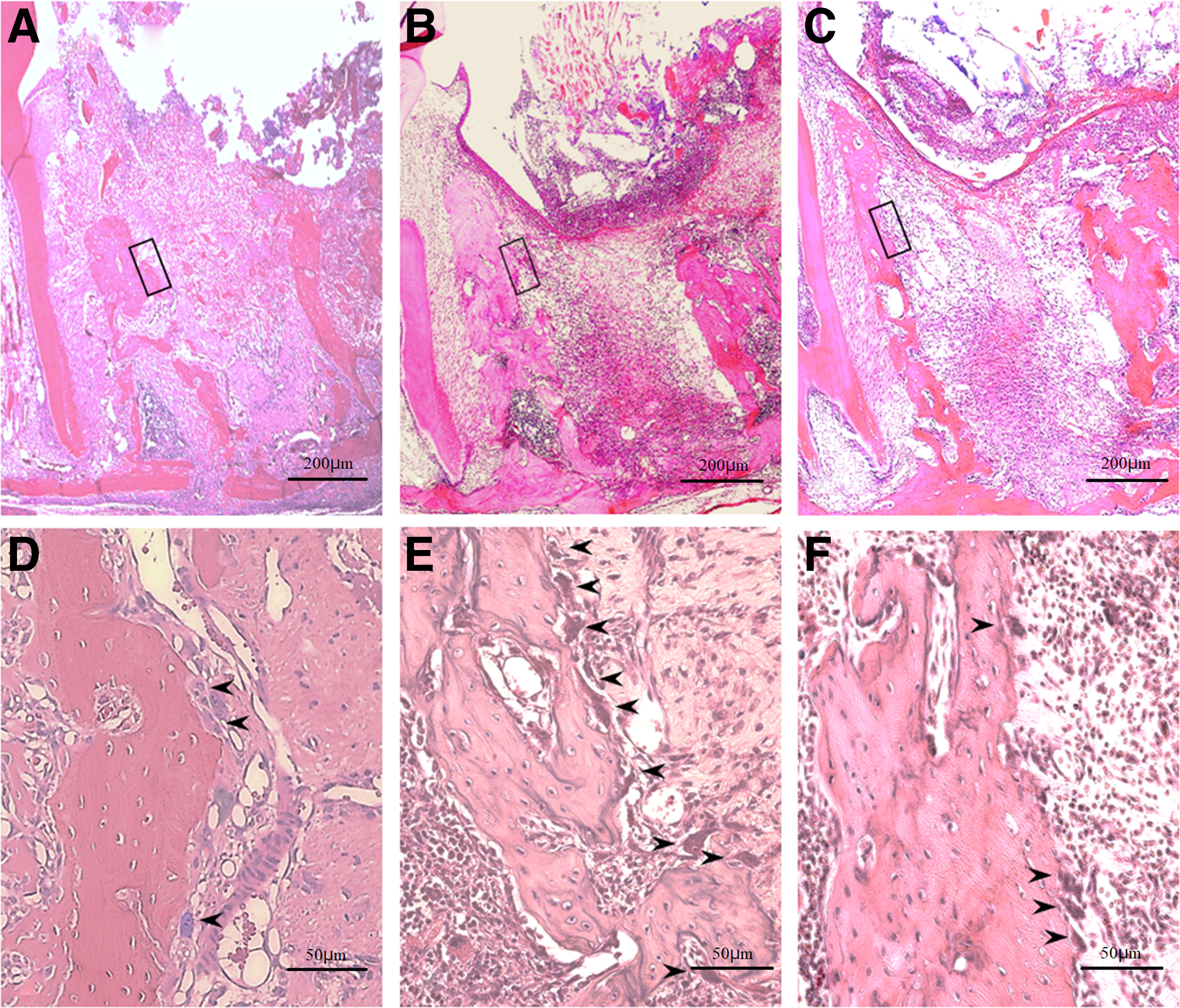
Histopathology on day 3 after tooth extraction.
Day 5 postextraction
New bone formation, which was not confirmed on day 3 postextraction, was seen in all three groups. New bone formation was apparent at only the socket fundus in the control group, but in the area from the socket fundus to the middle layer of the socket in the diode group, and at the socket fundus and the area from the middle layer to the shallow layers of the extraction socket in the CO2 group (Fig. 5A–C).
Histopathology on days 5 and 7 after tooth extraction. H&E staining; original magnification × 40.
Day 7 postextraction
Simultaneous bone resorption by osteoclast-like cells and bone formation around the socket were seen in the control group, while few osteoclast-like cells were observed in the laser treatment groups. The amount of cancellous bone was lowest, and cancellous bone formation was immature in the control group. New bone formation was confirmed from the socket fundus to the shallow layer of the socket in the diode group and from the middle to the shallow layer with a cross-linking pattern in the CO2 group (Fig. 5D–F).
BV was significantly higher in the lower layer of the extraction socket in the diode group compared with the control group (0.414 ± 0.051 vs. 0.317 ± 0.054; p < 0.01), but was significantly higher in the upper layer of the extraction socket in the CO2 group (0.424 ± 0.056), which exhibited cross-linked bone formation, compared with the diode group (0.244 ± 0.041) and the control group (0.262 ± 0.051) (both p < 0.01). Furthermore, in the whole socket, BV showed a tendency to be lower in the control group (0.289 ± 0.050) than in both of the laser groups (diode group: 0.328 ± 0.024; CO2 group: 0.390 ± 0.050) (Fig. 3B–D).
Day 10 postextraction
Extraction sockets were filled with newly formed bone, and there were many cells in the bone marrow and in the area around cancellous bone in all three groups. However, the bone marrow area was wide, and the cancellous bone was immature in the control group (Fig. 6A–C).
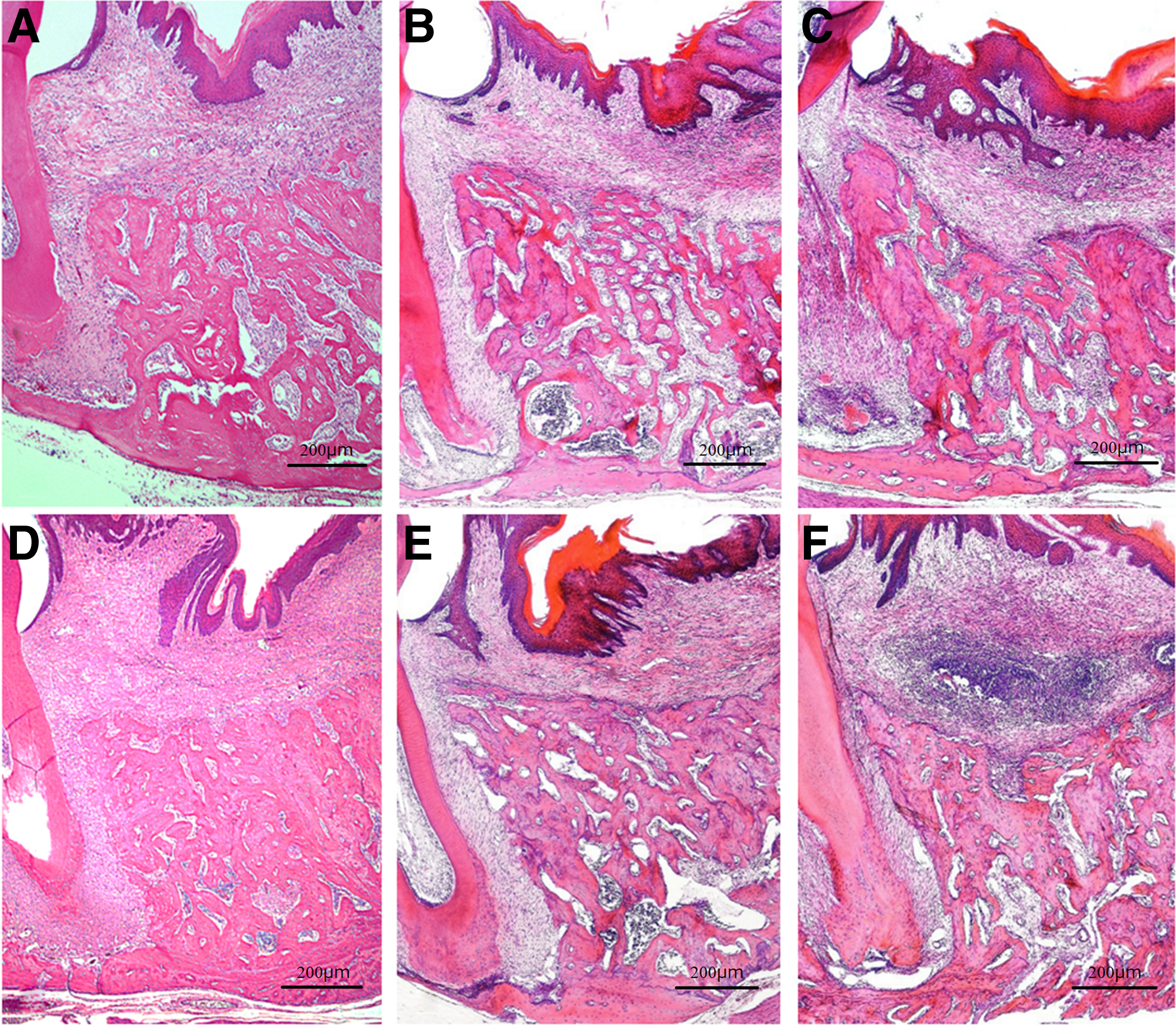
Histopathology on days 10 and 21 after tooth extraction. H&E staining; original magnification × 40.
Day 21 postextraction
Extraction sockets were filled with mature new bone with dense cancellous bone in all three groups. However, a concavity was noted at the center of the alveolar crest in the control group, while no concavity was seen in the laser treatment groups (Fig. 6D–F). The alveolar height index was significantly higher in the CO2 group (0.766 ± 0.039) and the diode group (0.798 ± 0.036) than in the control group (0.652 ± 0.079) (p < 0.01; Fig. 3E).
Regeneration of the mucosal epithelium in the extraction socket
We confirmed that a carbonized blood layer had formed on the extraction socket surface by applying HILT immediately after tooth extraction in the laser treatment groups. Regeneration of the mucosal epithelium was observed in all three groups at postextraction day 7. At postextraction day 21, there were no differences in histopathology findings of the mucosa among the three groups.
Immunohistological observation and measurement using α-SMA
α-SMA-positive cells were distributed across the extraction socket and mucosal epithelia of the extraction wound in the control group and in the CO2 group, but the number of positive cells was significantly higher in the control group than in the CO2 group (29.389 ± 7.846 vs. 10.130 ± 5.019; p < 0.001). In contrast, in the diode group, few α-SMA-positive cells were seen across the surface layer and the deep layer of the mucosa of the extraction wound with a significantly lower positive cell count compared with the control group (3.361 ± 1.556 vs. 29.389 ± 7.846; p < 0.001) (Figs. 3F and 7).
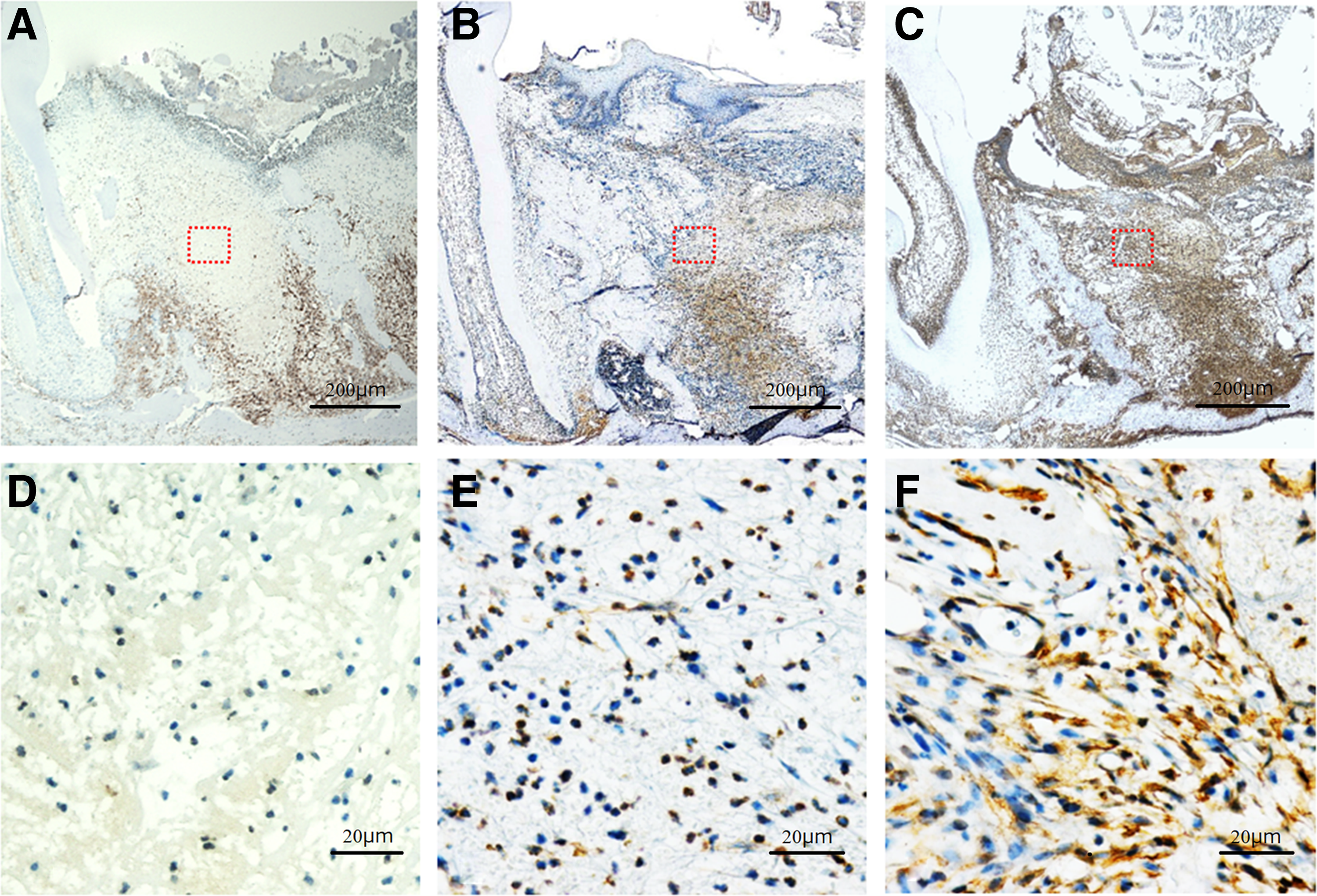
Histopathology and anti-α-SMA immunostaining of the extraction socket on day 3 after tooth extraction.
Discussion
The clinical efficacy of laser irradiation after tooth extraction was recently reported. 14,15 Basic research showed that irradiation with a tissue transmission-type laser (typically a diode laser) resulted in considerable fibroblast proliferation and organization in the early stage of healing, enhanced new bone formation and cancellous bone maturation, and a significant increase in BV. 24,28,29 In addition, several in vitro biochemical studies showed significantly increased expression of osteocalcin secreted by osteoblasts, 25,26 as well as type I collagen. 27 While in vitro studies showed increased alkaline phosphatase activity and type I collagen and osteopontin expression levels 72 h after CO2 laser irradiation of human osteoblast-like cells, 32 TGF-β1, BMP-4, and BMP-7 expression levels were increased from 4 days after irradiation, followed by enhanced calcification. 33
Meanwhile, results similar to those of extraction wound healing by PBMT have been reported. Mendes et al. applied hyaluronate sodium in the extraction sockets in rats. They found that active alveolar bone resorption was followed by marked new bone formation 7 days after extraction in the hyaluronate sodium-treated group; bone density was higher 21 days after extraction; and the boundary between existing alveolar bone and newly formed bone became unclear early. 34 These results also indicate that PBMT enhances wound healing.
In this study, the HILT and PBMT conditions were set according to a study by Fukuoka et al. 23 More precisely, the energy for HILT was calculated based on the time required for surface layer coagulation of the extraction socket in rats based on the output power and irradiation mode commonly used in clinical HILT. For PBMT, the rat gingiva was irradiated, and the output power, irradiation mode, and energy that did not cause irreversible changes were determined based on histopathological findings. The most significant point in this morphometrical analysis is that the two kinds of lasers differ in terms of characteristics recommended by the FDA.
Based on this difference between the lasers used, we measured the bone quantity of the extraction socket divided into three regions, namely, the upper part of the extraction socket which was expected to reflect the effect of the CO2 laser, the lower part of the socket which was expected to reflect the effect of the diode laser, and the entire socket. In addition, we selected day 7 postextraction for this measurement because the boundary between the extraction socket wall and newly formed bone became unclear with the healing of the socket, so conducting measurement became difficult on and after day 10 postextraction.
In the measurement of the height of alveolar bone, the rat maxillary first molar has five dental roots. Because damage to the interradicular septum during tooth extraction could cause measurement failure, our measurements were based on the relative evaluation of the height of the interradicular septum (hA) of the second molar and the surface layer of new bone (hB) in the extraction socket of the first molar (Fig. 2C). Fukuoka et al. and Noda et al. had almost the same opinions as ours about these measurement methods. 23,25
Results of this study indicated an important role for carbonization of blood on the socket surface that resulted in the formation of artificial scab by HILT, in addition to the well-documented tissue activation by PBMT. This artificial scab enabled rapid physical closure of the extraction socket and clot retention high up in the socket with inhibition of mucosal epithelial invagination into the extraction socket, ultimately resulting in formation of new bone with good height (a space-making effect of the artificial scab in the extraction socket).
New bone formation in the extraction socket usually starts from the fundus, but a cross-linking pattern of new bone formation was observed in the shallow layer of the socket in the CO2 group. The penetration depth of CO2 laser light was shallow at 0.05 mm, and thus, the effect of photobioactive reactivity may be concentrated on the surface layer of the extraction socket. In contrast, the penetration depth of diode laser light is deep with an area of photobioactive reactivity, suggesting enhancement of new bone formation at the lower layer of the extraction socket.
The photobioactive reactivity caused by irradiation with these lasers was considered to promote the differentiation and proliferation of cells by stimulating undifferentiated mesenchymal stem cells, bone marrow stem cells, osteoblasts, osteoclasts, and bone lining cells, thereby activating bone remodeling. 35,36 Subsequently, the stimulated osteoblasts produced collagen fibers and proteins associated with bone formation. 37 –39 In addition, the osteoblasts migrated on the fibers forming scaffolds for new bone formation. We therefore surmise that characteristic bone formation in the same area occurred in our study. These phenomena were similar to the finding that an artificial collagen sponge implanted in the extraction socket promotes the differentiation and proliferation of mesenchymal stem cells and provides a scaffold for bone formation. 40,41
Recently, tissue activation by PBMT was shown to be strongly associated with mitochondrial adenosine tri-phosphate (ATP) production facilitated by cytochrome C oxidase, but the precise effects of the laser wavelengths used in the present study remain to be clarified.
Infection is a potential concern, but bacteria will be dispersed following HILT, and the carbonized blood on the surface of the extraction socket will prevent entry of bacteria and food debris. Accordingly, the risk of infection in the extraction socket below the carbonized blood is expected to be minimal.
In terms of expression of myofibroblasts in the extraction wound in this study, decreased myofibroblast counts were seen in only the surface layer of the extraction wound in the CO2 group, while few myofibroblasts were seen across the extraction wound in the diode group. This may also be explained by the difference in penetration depth between the two lasers. de Freitas et al. reported that the number of myofibroblasts proliferating in an incision wound on the back of the tongue was smaller when a CO2 laser was used than when a scalpel was used in rats. 42 Pinheiro et al. also reported that the number of myofibroblasts in an incision wound on the back was increased when rats were irradiated with polarized light, but decreased with a diode laser. 43 These are in good agreement with decreased myofibroblast number in the early wound healing stage shown in the present study.
The method examined in this study is promising for broad clinical application in humans, with potential use for nearly all patients who undergo tooth extraction. This method would be very effective for patients taking anticoagulants or antithrombotic agents or those prone to bleeding. In addition, for cases with limited blood supply from the extraction socket wall, it would be effective to soak artificial filling material (e.g., a collagen sponge) with blood, place it in the upper extraction socket, and char the surface layer. This is consistent with “coagulation of the extraction site” advocated by the FDA.
Conclusions
Combination of HILT and PBMT achieved good socket preservation, specifically, preservation of good alveolar crest height and enhanced wound healing in a rat model of tooth extraction. This method appears promising for clinical application in humans and warrants further investigation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Grants-in-Aid for Scientific Research from Japan Society for the Promotion of Science (JSPS-KAKENHI-Grant no. 15K11183).