
Abstract
Introduction
R
This case report presents an interesting combined application of traditional reconstructive surgery and IPL for the restoration of a post-traumatic eyebrow defect.
Case Report
A 28-year-old male patient was admitted to our Plastic Surgery Department for a post- traumatic loss of the lateral half of his left eyebrow, which had occurred 1 year previously.
The clinical examination demonstrated a broad area of retracting scar tissue involving his left forehead, with complete loss of the lateral half of his ipsilateral eyebrow (Fig. 1).

Pre-treatment view.
Surgical eyebrow reconstruction was performed, with an axial temporal-hair bearing scalp island flap pedicled on the anterior branch of the superficial temporal artery and venae comitantes. The flap was tailored on the contralateral brow and transferred to the recipient site through a subcutaneous tunnel, and the donor site was repaired with a local rotation scalp flap (Figs. 2 and 3). Two months later, multiple Z-plasties were performed to refine the alignment between the native medial eyebrow and the scalp hair-bearing island flap (Figs. 4 –6). The patient regularly trimmed hair growth in the reconstructed eyebrow, and this commitment did not give rise to any complaint by him. Nevertheless, although a significant improvement had been achieved with the restoration of the missing brow tail, the patient still complained of an overall unnatural eyebrow appearance. Objectively, a persistent localized erythema and a marked difference in hair density in comparison with both the native medial half of the left eyebrow and the contralateral one was still apparent 9 months after the last surgical step (Fig. 7).
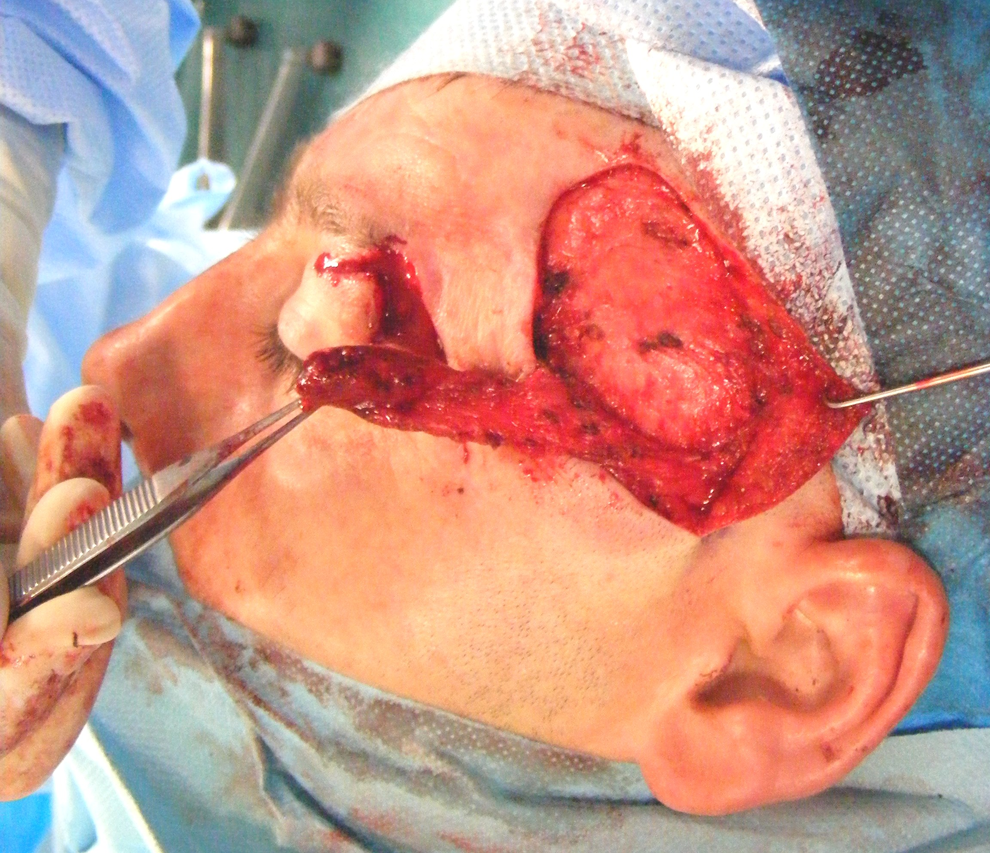
First surgical stage intra-operative view: the axial temporal hair-bearing scalp island flap pedicled on the anterior branch of the superficial temporal artery and venae comitantes.

First surgical stage intra-operative view: hair-bearing skin flap transferred to left brow and donor site repaired with a local rotation scalp flap.

First surgical stage postoperative view.
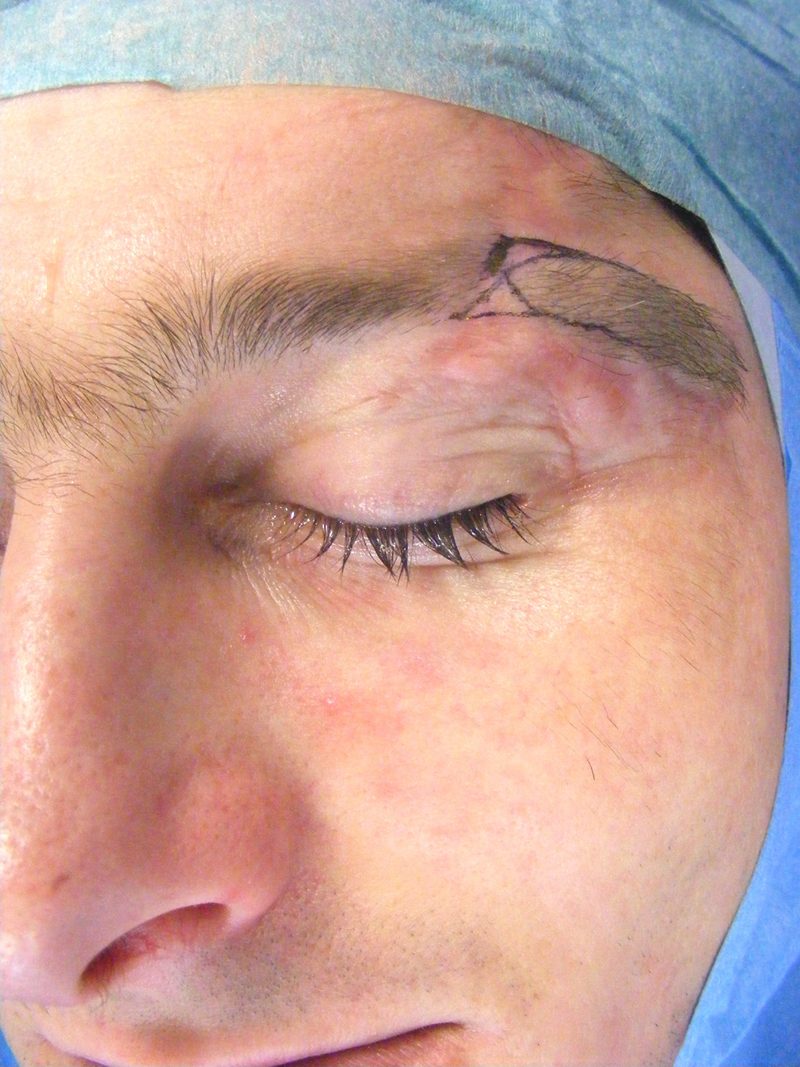
Second surgical stage operative planning.

Second surgical stage intra-operative view: multiple Z-plasties to refine alignment between the native medial eyebrow and the scalp hair-bearing island flap.

Second surgical stage postoperative view.
In order to address such residual imperfections, an IPL treatment was planned using the StarLux® 500 IPL platform from Palomar. The LUX RS™ hand piece was employed for hair removal (wavelength 650–1200 nm, spot size 12×28 mm, pulse length 5–400 ms, maximal fluence 70 J/cm2, maximal frequency 2 Hz). Thirty-six J/cm2 of energy were delivered through four 12×28 mm spots for 20 msec per spot. The MAXG™ hand piece was employed for scar erythema reduction (wavelength 500–670 and 870–1200 nm, spot size 10×15 mm, pulse length 1–500 ms, maximal fluence 80 J/cm2, maximal frequency 2 Hz). Fifty J/cm2 of energy were delivered through eight 10×15 mm spots for 40 msec per spot. This dual combination treatment was repeated after 2 months in order to address some residual imperfections. The parameters were the same as at the first session, except that the number of spots was decreased to two for the LUX RS hand piece and to six for the MAXG hand piece.
Over a period of 6 months, a significant improvement in the overall clinical picture was noted, with a subtotal reduction of scar erythema and a hair density and distribution in the skin scalp island flap similar to that in the native eyebrow (Fig. 8). This outcome was considered to be very satisfactory by both the surgeons and the patient

Post- intense pulsed light (IPL) treatment view.
Discussion
A plastic surgeon is committed to restoration of both body function and the aesthetic appearance of beauty. Several surgical techniques have been described for eyebrow reconstruction: full-thickness scalp and eyebrow grafts, mini- or micro-scalp hair grafts, flaps from a thick ipsilateral or contralateral eyebrow, and axial skin island flap from the temporal scalp. 1 –4 Each technique has its advantages and disadvantages. A full-thickness hair-bearing skin graft, from the scalp or the eyebrow, is a time-honored technique that may undergo an unpredictable rate of take; within such a category a scalp skin graft provides a scalp-like high hair density; mini- or micro-hair grafts are an effective method of eyebrow restoration in terms of hair density and orientation, but are multi-stage and time-consuming procedures; 1,2 the hair-bearing skin island eyebrow advancement flap is the appropriate solution for restoring the missing medial portion of the brow from a thick lateral one; 3 the hair-bearing transposition flap from the contralateral eyebrow provides reconstruction with an excellent hair density, but with the wrong orientation, and a subsequent unnatural appearance; 4 the axial skin island flap from the temporal scalp based on the anterior branch of the superficial temporal artery and venae comitantes provides a single-stage procedure with the correct hair orientation but with a scalp-like hair density. 4 IPL is a very versatile tool that proved its effectiveness in a variety of skin conditions: hypertrichosis and hirsutism, skin vascular lesions (port wine stains, rosacea, teleangectasias, erythrosis), acne, and skin aging. 5 –13 The potential combination of different wavelengths, fluences, pulse durations, and pulse intervals allows a patient customized treatment within a wide spectrum of therapeutic indications. In our case, we deliberately preferred IPL to laser for hair removal, as its lesser hair count reduction could provide a smooth hair thinning out rather than an aggressive and more radical epilation in the reconstructed eyebrow. An increasing number of reports demonstrated the even superior effectiveness of IPL versus laser in the treatment of skin vascular alterations such as rosacea and erythrosis. 7,10,12 Therefore, it was our option of choice for the treatment of persistent localized erythema in our patient's reconstructed eyebrow. Furthermore, to all of the previously mentioned features were added the demonstrated advantages of IPL in providing lower pain scores and local inflammation. 5,9,12
IPL treatment was the only way to overcome the limitations of the traditional surgical technique, by providing a naturally irregular hair density in the reconstructed eyebrow.
Our experience demonstrated the efficacy of the integrated multidisciplinary approach involving traditional plastic reconstructive surgery and the innovative new technologies 5 –13 in aiming for perfection.
Footnotes
Acknowledgments
The authors thank Alan Serge McGhee, Glasgow City Council Education Department, for his contribution to the submission of this article.
Author Disclosure Statement
No competing financial interests exist.