
Abstract
Introduction
MAL, a novel photosensitizer precursor, showed deeper tumour penetration and fewer adverse effects than 5-aminolaevulinic acid (ALA) due to the enhanced lipophilicity. To our knowledge, there has been no clinical trial to date of topical MAL-PDT therapy in the treatment of PEH. Therefore, to test the effectiveness of PDT, we performed this clinical trial involving a case series.
Case Report
After obtaining ethics committee approval and patients' informed consent, three patients with 16 lesions were enrolled. The diagnosis of PEH was confirmed by at least a 5-mm incision biopsy taken from the thickest part of the lesion. Topical 5–30% (w/w) MAL (Biosynth AG, Staad, Switzerland) emulsion (Tanabe, Tokyo, Japan) was applied for 6 h before irradiation with narrowband continuous red light (wavelength 633 nm, output light intensity 126 mW/cm2) from light-emitting diodes (LEDs; Omnilux, Altrincham, Cheshire, UK) The individual LED cone angle and the spacing of the LEDs ensure uniformity of the beam for full coverage of the treatment area. The dimensions of the LED head active area were 150 × 350 mm (length × width). Each lesion, plus a 5-mm margin of disease-free skin, was successively irradiated at 10–15 cm distance for one to three sessions (total delivery light dose = output light intensity × time: 113–339 J/cm2), 15 min per session, 1 week apart. The procedures were handled according the manufacturers' recommendations. The light dose and MAL concentration were randomly used for the lesions. The lesions were photographed on a separate day of each week, so that neither the application of the cream nor the crusts affected assessment. Lesions were evaluated and rated by an observer blinded to the study protocol 3 months after the treatments. The lesions were scored as follows: complete response (CR, complete disappearance of lesions), minimal response (MR, <30% clearance), and no response (NR, no changes in size). Patients were scored on pain by a visual analogue scale (VAS; 0, no pain; 10, worst pain). 8
The clinical characteristics and treatment response of each patient are summarized in Table 1. One PEH (patient 1) occurred after a scratch wound; two PEH cases (patients 2 and 3) were caused by a burn wound. The clinical response of one representative case (patient 3) is shown in Fig. 1. Only 4 of 16 lesions clinically showed a minimal response. No response was seen in 12 of the 16 lesions, using either different cumulative doses or different concentrations of MAL. Although four lesions (patients 1 and 3) had a minimal response, changes were slight in diameter or thickness. This may be due to fibrosis in the dermis caused by PDT. The fibrosis was confirmed by histological examination.
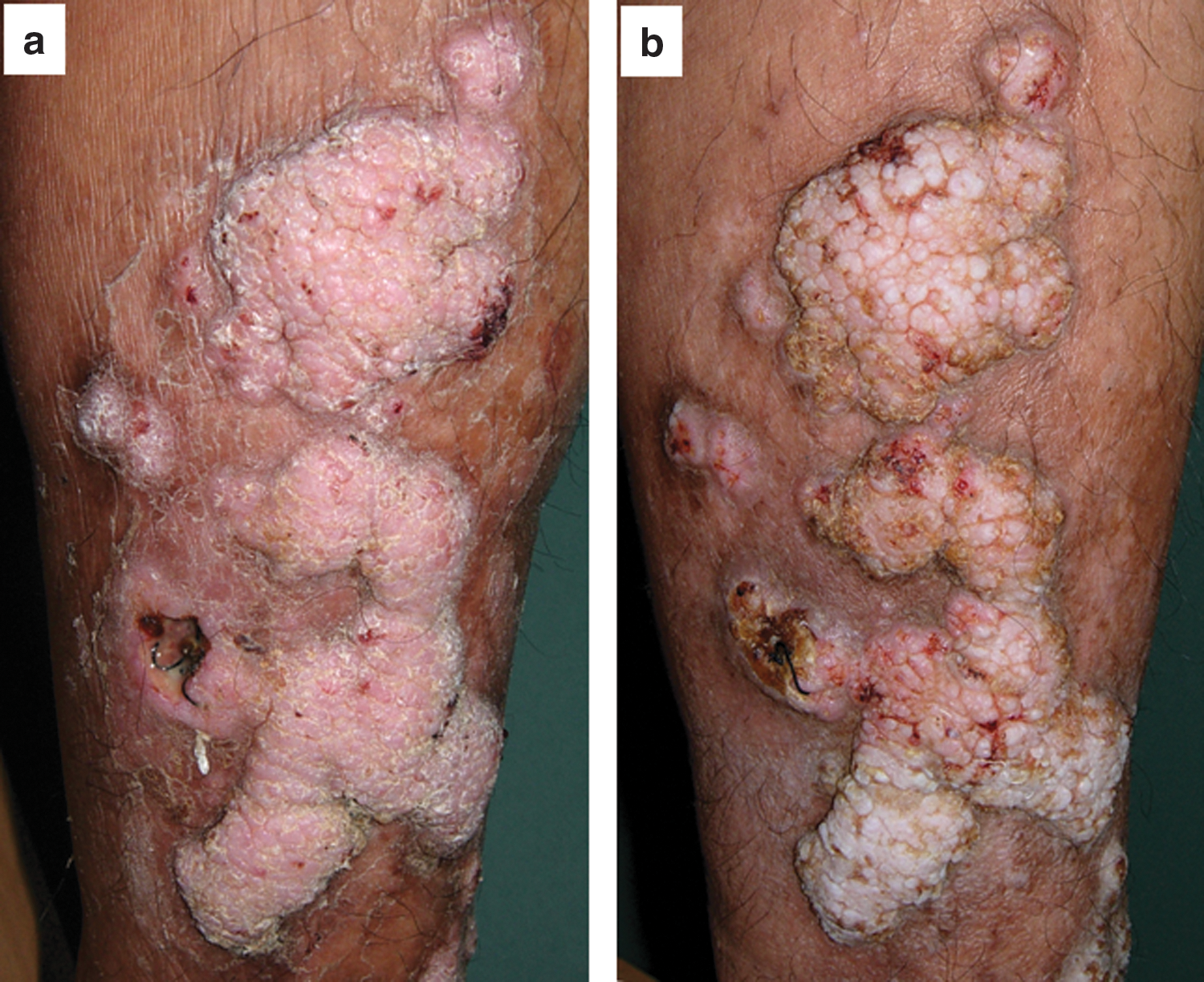
Clinical response of cutaneous pseudoepithliomatous hyperplasia of leg treated with the ALA-PDT. Minimal response is shown after two treatments (226 J/cm2)
MAL, methyl aminolaevulinate; CID, cumulative irradiation dose; MR, minimal response (<30% clearance); NR, no response; VAS, visual analogue scale.
Discussion
PEH is a type of exuberant proliferation of the epithelium with down-growth into the dermis occurring in a variety of settings. The pathogenesis still remains unclear. The histological features are similar with well-differentiated, invasive SCC, or may obscure an underlying malignant process, such as melanoma and granular cell tumour. There is no standard or optimal treatment: inappropriate invasive modalities such as cryotherapy and CO2 laser curettage leads to an extension of the lesion area. In the three cases studied, their occurrences were associated with skin wounds: underlying tumours were excluded by histological examination. They each successively received occlusive topical steroid therapy, cryotherapy, laser curettage, and topical 5-FU. Unfortunately, these treatments were ineffective and even worsened the lesions. The patients refused surgical excision, since a large skin graft would be involved. Thus non-invasive PDT with its low-risk and positive cosmetic outcome was attempted. However, all the 16 lesions treated with topical PDT showed no complete response, even when given an increased photosensitizer or irradiation dose. Patients refused the second treatment.
This clinical trial indicates that topical MAL-PDT is not an effective therapy when applied to PEH after skin wounding. There are two possible factors associated with the poor response. One is the pathological features of PEH. It has been demonstrated that two mechanisms are involved in the clearance of a tumour and proliferating squamous cells. Epithelial neoplastic cells in AK, BD, and SCC may absorb much more photosensitizer than normal cells, leading to the elimination of the atypical cells. A study on the viral wart showed that PDT using an LED source achieved clearance rates of 81% (mean of 3.34 treatments). 4 Complete clearance of periungula hand warts in 18 of 20 patients (30 of 40 warts) was achieved in a pilot study of PDT with ALA after a mean of 4.5 treatments. 7 PDT leads to the release of inflammatory mediators, like interleukin 2, interleukin 1-β, and tumour necrosis factor-α, 9 suggesting that another mechanism for the clearance of these cells is in the indirect stimulation of local immune responses in the lesion area. Although the PDT parameters that were employed for the viral wart or the epithelial neoplasms were also used for PEH, all of the lesions responded poorly. This suggests that the lack of effectiveness could be attributed to the peculiar pathological pattern, not to the neoplastic or inflammatory epithelia proliferation of PEH.
Another possibility for the lack of response is the thickness of the skin keratin layer in PEH. A previous study showed that two precancerous lesions, including oral verrucous hyperplasia (OVH) and oral leukoplakia (OL), responded well to topical 20% ALA-PDT; 8 of 8 OVH lesions achieved CR, 8 of 24 OL lesions showed CR. 10 The major difference between PEH and OVH or OL is the thickness of oral mucosa and the cutaneous surface keratin layer. OL or OVH lesions with a thinner keratin layer achieved CR, which enabled more ALA to diffuse into the tumour tissue. 10 This indicates that the poor response is associated with absorbance of the photosensitizing agent in PEH, not with MAL concentration or illumination dose. It also indicates that therapeutic response seems not to be obviously related to treatment parameters. Nevertheless, there is a limitation with this study. As it was a small-sample case series, sampling error has to be involved in the therapeutic outcome and treatment parameters. Thus a large retrospective comparative follow-up study will be required for the re-confirmation of the relationship between the poor response and the parameters.
To some extent, pain reflects response during irradiation; patients (1 and 3) with greater pain at the same illumination are likely to have better response, as high pain scoring presents a severe destruction of local tumour tissue, regardless of lesion location. Although the patients with minimal response experienced mild pain compared with patients who had no response, the mean pain scores were still lower than the score of 6.4 of well-responded AK irradiated by LED. 11
In conclusion, this case series suggests that topical PDT lacks effectiveness at the variable MAL concentrations and illumination dose. Thus we do not advocate the use of topical PDT for PEH patients with skin wounds. Besides removal of any underlying diseases, surgical excision is still the recommended first option in treating PEH.
Footnotes
Author Disclosure Statement
No competing financial interests exist.