
Abstract
Tobacco use among pregnant women, as well as second- and third-hand smoke exposure of their infants, translates into the startling fact that more than one third of American children live with at least one parent who smokes cigarettes daily. Maternal smoking or second-hand smoke exposure during pregnancy is deleterious to the mother's health and contributes to prematurity, low birth-weight infants, and increased risk of sudden infant death syndrome (SIDS) and recurrent wheezing during the first year of life. Pregnant women who stop tobacco use during pregnancy are at high risk for postpartum relapse frequently associated with a partner who smokes tobacco, stress, poverty, and lack of social and medical support to remain tobacco free. Enhanced efforts to identify and support pregnant women who smoke, and to implement strategies to prevent exposure of their fetus and newborn to the hazards of tobacco-smoke exposure, are paramount in our public health efforts to eliminate health disparities in the United States. We discuss the critical elements of programs to assist mothers to stop smoking during pregnancy and toward family efforts to maintain a smoke-free environment for their infant.
Postpartum interventions, whether in the neonatal intensive care unit (NICU), newborn nursery, or postnatal care setting, can provide assistance that women need to remain smoke free, to educate spouses or significant others and their families, and to aide in establishing goals of maintaining a tobacco smoke-free home and car. Physicians and other perinatal healthcare providers have a duty to identify pregnant women who smoke for “meaningful use” in the electronic medical record, and to provide advice and assistance in evidence-based smoking interventions in obstetrical care settings. Pediatricians, neonatologists, and others providing postpartum, “normal” nursery or NICU care have an opportunity to protect infants and young children from second- and third-hand smoke exposure by assisting their parents and family members in maintaining a tobacco-free environment to improve the health of infants, toddlers, and young children.
Maternal smoking has been linked to a variety of deleterious effects on the mother's pregnancy and her developing child. Pregnancy-associated complications include increased risk of ectopic pregnancy, spontaneous abortion, premature rupture of membranes, and placental complications, including placental abruption. Long-term health risks to smoking women include heart disease, cancer, early death, and links to many other diseases and health problems. Infants of smoking mothers have an increased risk of preterm birth, low birth weight, and sudden infant death syndrome (SIDS); they also are more likely to have recurrent wheezing during the first year of life, frequent otitis media, restless sleep, and colic.2–10 Cognitive effects from smoke exposure, including learning disabilities and conduct disorders, have been reported.11–13 Levy et al. reported that school-aged children, aged 6 to 11 years, living with one or more smoking adults had 1.06 to 1.54 more days absent from school per year compared to children from non-smoking homes. Children in the cohort had increase number of ear infections and “chest colds” compared to children who did not live with smokers. 14
While exposure to second-hand smoke has received much attention, the importance of exposure to third-hand smoke should not be overlooked. Winickoff described third-hand smoke as the contamination that remains after a cigarette (or other tobacco products) has been extinguished.15,16 Even unburned tobacco (such as residual tobacco in a “butt”) can create carcinogenic compounds, tobacco specific nitrosamines (TSN), by reacting with nitrous acid (emitted from gas appliances and vehicles, among other sources). Sleiman et al. report substantial levels of TSN on surfaces resulting from a 0.4% conversion of nicotine to TSN. 17 Residual nicotine persists in high concentrations on indoor surfaces, including clothes and human skin. Once TSNs are created, they can persist on surfaces for weeks to months. Infants and children are more likely than adults to be in contact with TSN through dermal exposure, dust inhalation, and ingestion as they crawl and explore their homes. This represents “an unappreciated health hazard.” While it has been well documented in animal models and in premature human infants that in utero tobacco-smoke exposure damages fetal lungs during lung development, TSNs have also been shown to cause fetal lung injury.18–20
Rates of breastfeeding are also affected in mothers who smoke. While the American Academy of Pediatrics recommends that mothers breastfeed their infants for at least 6 months, women who smoke are less likely to initiate breastfeeding and are more likely to stop early.21,22 One reason smoking mothers may breastfeed less is that they perceive insufficient milk supplies and may have difficulty with milk “letdown” and release.23,24 Many mothers believe that by not breastfeeding, they are not exposing their infants to the toxins in tobacco smoke. Indeed, smoking mothers who breastfeed expose their infants via breast milk to the pesticides, dioxins, and cadmium that are in tobacco smoke.25,26 Breast milk of smoking mothers also has lower vitamin and antioxidant levels; the taste of the milk is also altered leaving the milk less desirable to nursing infants. 27 Breastfed infants of mothers who smoke have a 10-fold higher urinary cotinine concentration, a metabolite of nicotine, than formula-fed babies.28,29 Smoking mothers are still advised to breastfeed their infants, despite nicotine levels and other contaminants, because the benefits to immunity, growth, and nutrition outweigh the risks of chemical exposure. 30 Women who manage to stop tobacco use either before or during pregnancy are just as likely to breastfeed their infant as non-smoking women, as long as relapse prevention strategies are implemented after birth. 23
The Department of Health and Human Services has stated that “women are more likely to quit smoking during pregnancy than at any other time in their lives.” 5 Mothers-to-be are highly motivated to do whatever it takes to have a healthy baby. While motivation and confidence to stop smoking are typically high during pregnancy, they are not consistent predictors of remaining tobacco free. Johnson et al. reported that approximately 90% of mothers who stopped smoking during pregnancy intended to remain smoke free postpartum. 31 Approximately 45–70% of women who successfully stop smoking during pregnancy resume tobacco use within 1 year after delivery.32–36 Hajek et al. reported a direct relationship between a mother's desire to stop smoking and not smoking up to birth, but an inverse relationship between the severity of the pregnant mother's tobacco dependence and her ability to stop smoking without treatment. 37 A mother's level of confidence in her ability to control smoking in her home is a significant factor in minimizing an infant's second-hand smoke exposure. 38 Likewise, a mother's level of confidence to remain tobacco free significantly affects relapse rates.39,40 Without support to remain abstinent after birth, a mother's level of confidence wanes, and a relapse is predictable.
The challenges that new mothers confront make them more susceptible to return to tobacco use, and the reasons for their relapse are multifaceted. Mothers who smoke during pregnancy tend to be Caucasian and African American, infrequently Hispanic. They tend to be from lower socioeconomic backgrounds, have less education, and be more resistant to stop tobacco use.41,42 Women of lower socioeconomic backgrounds are at higher risk for domestic abuse, other addictions, have less social support, and may be depressed, all of which contribute to increased stress levels and relapse.41,43–45 While mothers are often motivated to quit during pregnancy by their desire to protect their developing baby, they relapse after birth believing that smoking is no longer harmful to their children.46,47 A survey of parents whose infants were admitted to the neonatal intensive care unit (NICU) reported that more than 70% said smoking was only “a little” or “somewhat” harmful to their infant. 48 Clearly, there is a gap or lack of maternal knowledge on the effects of infant exposure to second-hand smoke, and there remains a chasm in efforts to educate and support these women effectively to prevent harm to their fetus and infant. This gap in infant protection often extends to the spouse or partner, who may have smoked throughout the pregnancy, yet the issue of their stopping tobacco use was never broached. Recent studies have shown that approximately 50% of women are exposed to second-hand smoke either by a partner who smokes or by coworkers. 49 While spouses and significant others are more likely to be the smoker in the household, mothers are more likely to receive nicotine-dependency treatment.48,50,51
The American Congress of Obstetrics and Gynecologists (ACOG) recommends obstetric healthcare providers screen all patients for their smoking status and offer tobacco-dependence treatment.52–54 The importance of early identification of mothers in need of tobacco-dependence treatment services is underscored by the evidence that successful efforts to stop smoking initiated early in pregnancy significantly improve pregnancy-related outcomes. 41 Studies reveal a 17% decrease in preterm births in women who successfully quit tobacco use. Furthermore, infant birth weight can be increased, by nearly 1 ounce, if efforts to stop smoking are successful before the 30th week of gestation; this accompanies a 20% reduction in the number of low birth-weight infants.53,55,56
While 93% of obstetricians ask their patients about smoking, only 28% assist them with stopping tobacco use, and only 24% actually follow up. 52 Screening by simply asking women whether they use tobacco products, or are exposed to tobacco smoke, is insufficient. When verbal reports of smoking status have been compared to urinary cotinine levels, an approximate 25% discrepancy has been reported. 57 Since urine cotinine measurement is relatively inexpensive and quick (dipstick method), it can be easily integrated into prenatal visits and may reveal tobacco-smoke exposure unknown to the pregnant woman.
Using the technique of the “5 As” has been shown to be effective in identifying and assisting individuals in their efforts to stop smoking. Care providers are encouraged to ask their patients about tobacco use, advise them to quit, assess their willingness to make a quit attempt, assist them in a quit attempt, and arrange follow up. 52 For patients who are clearly unwilling to quit at the time of assessment, motivational interviewing using the “5 Rs” can be effective. This helps the patient to identify relevant motivational factors, know the risks of continued smoking, determine the rewards of quitting, prepare for potential roadblocks, and encourage repetition of these strategies at every visit. 5 Even though these brief interactions have been shown to help smokers stop, fewer than 20% of obstetricians fully implement the guidelines of ACOG.58,59
Recently, ACOG has reemphasized the importance of prenatal screening and tobacco-dependency treatment by providing a brief, clinically focused toolkit for practitioners based on pregnancy-specific tobacco-dependency interventions. 52 A meta-analysis of interventions that provide brief counseling sessions and integrate pregnancy-specific self-help materials showed rates of stopping smoking of up to 80% in those who participate from the first prenatal visit throughout pregnancy. 60 Obstetrical care providers are in a unique position to provide focused tobacco-dependence treatment during prenatal visits and may have the biggest impact influencing mothers to stop smoking. Relapse may also be delayed or prevented among women who receive postpartum interventions; therefore, more emphasis on relapse prevention must be a goal of both obstetric and pediatric providers.46,61
Following delivery, systematic follow-up of smoking status is critical and should be continued within the context of pediatric care. Few postpartum wards and neonatal intensive care units in Southern California (6%) have a formal postpartum educational program (survey performed in Southern California, 2011 by the authors, unpublished data). Accurate medical record documentation of the interventions provided during prenatal care, positive counseling to encourage mothers to remain abstinent, and ongoing education regarding the benefits to a newborn of having a smoke-free home is required. The Health Information Technology for Economic and Clinical Health Act authorizes incentive payments through Medicare and Medicaid to clinicians and hospitals when they use electronic health records for “meaningful use.” Identification of tobacco smoking for all patients 13 years or older is one meaningful use criteria; however, this Act did not provide funding for effective interventions when smokers were identified. 62
Several studies have emphasized the importance of programs targeting parents to stop smoking during any period when they are more likely to make life-style changes, “teachable moments,” including the postpartum hospital stay,44,50,63,64 the hospitalization of a child, including the NICU,51,63,65 and at follow-up pediatric and obstetric appointments. 43 These “teachable moments” are critical points in time when parents are most open and willing to focus on improving their health and the health of their infants. Parents and extended family members should receive teaching and counseling and be enrolled in programs that assist them to stop smoking. Ideal programs should offer resources, follow-up to prevent relapse, nicotine replacement therapy, and potentially group encounter sessions.
Counseling provided to parents needs to emphasize education that is relevant to the parents. Specific information reported to be the most powerful in overcoming tobacco dependency is the increased awareness regarding the impact of smoking. Information that can have a positive impact on successful stop tobacco use efforts includes education on the incidence of miscarriage and SIDS, 66 the value of support from family and friends, how to manage stress properly, good parenting techniques, and how to maintain a smoke-free home. In addition, the importance of breastfeeding, how to have a good attitude and body image, maintaining proper nutrition and exercise, knowing the consequences of smoking on the baby's health, and viewing abstinence as a permanent life-style have a positive impact. 51 Ongoing praise and reinforcement by pediatric and postpartum staff with encouraging phrases, such as “Your decision to remain smoke-free is helping your baby have a healthy start,” may reduce the likelihood of relapse. In addition, women should be counseled that stopping tobacco use will reduce all associated smoking effects. Enrolling mothers in a program can ensure they are receiving this information.
There have been a variety of specific programs developed that have used videos, educational handouts and pamphlets, certificates, phone calls, and in-person counseling sessions to help mothers quit. A media campaign called “The Great Start Program” was the first national program focused on providing free counseling to pregnant women on how to stop tobacco use. It was a public service announcement (PSA) campaign in 33 states intended to raise awareness regarding the dangers of smoking. PSAs would direct pregnant smokers to telephone counseling that was specifically targeted to their demographic. Focus groups conducted during the program found that a media campaign alone was insufficient to affect smoking habits. 45 In Australia, Ling et al. demonstrated that an evidence-based smoking intervention for parents during their infant's NICU stay resulted in one third of parents stopping smoking. 67
The most effective programs are those that provide incentives in addition to education and support.56,68 The “Baby and Me” program, funded by the New York Department of Health, combined prenatal and postpartum tobacco-dependency services. As an incentive, mothers were given diapers, because these essential items could not be obtained from other assistance programs, such as the Women, Infant and Children Program (WIC). The study reported an increase in their quit rate up to 60% prenatally and 32–64% postpartum. 46
At Loma Linda University Medical Center (LLUMC), we have developed a multimedia program with incentives called “When You Smoke Your Baby Smokes.” The program is designed to support mothers and fathers during the immediate postpartum period. Trained personnel interview mothers during their postpartum hospitalization regarding their smoking status. Mothers and family members, if present, watch an interactive video presentation that educates them on the harmful effects of smoking and second- and third-hand smoke exposure on their infants regardless of smoking history. This educational video was developed by Loma Linda University and Patient Programs of Richmond, Virginia, and is available at www.patientprograms.com/PEP/Smoke.html (for PCs only). Eight weeks of follow-up educational material, including weekly mailings, e-mails, and robotic telephone calls, were developed to provide education on smoking relapse prevention and normal newborn care. We conducted a prospective randomized study from March to September 2010 where mothers with a history of smoking within 12 months prior to conception or during pregnancy and who were not currently smoking at time of delivery were randomized to receive only the educational video while hospitalized or to watch the educational video and to receive the additional 8-week postnatal educational intervention. During the study period, our overall relapse rate was 20% at 8 weeks postpartum; however, there was no statistical difference between the two groups. 69
We have integrated the “When You Smoke Your Baby Smokes” program at LLUMC with the Comprehensive Tobacco Treatment Program, a California First 5 funded program, which provides tobacco-dependency and smoking-relapse prevention services throughout San Bernardino County, California (Fig. 1). Smoking mothers and/or their smoking partners are enrolled in the program and are contacted weekly for 8 weeks via weekly mailings, telephone calls, and visits with program staff. If they are confirmed to be smoke free by urine cotinine levels, they receive weekly incentives. From July 2010 to September 2011, we enrolled 242 mothers and 124 fathers or other family members, who were self-selected during interviews with the program staff. A total of 106 mothers (43%) completed the 8-week program with urinary cotinine documentation of non-smoking. By October 2011, 45 mothers had been contacted for follow-up. Of those, 42 mothers (93%) reported they continued to be tobacco free. Thus it is highly likely that mothers who are able to remain abstinent during the 8-week program will continue to remain tobacco free. 70
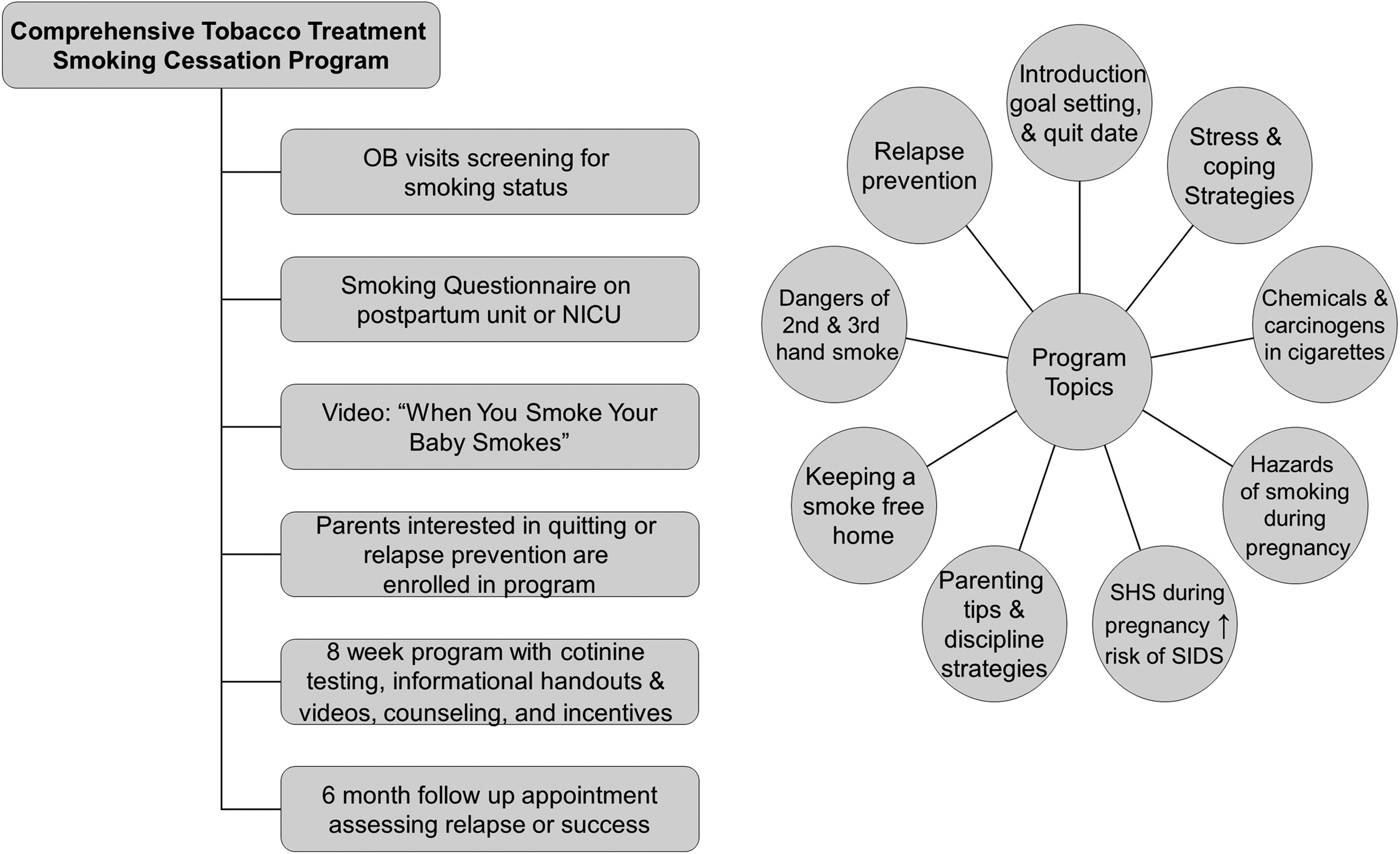
A diagram of the comprehensive “When You Smoke Your Baby Smokes” treatment program at Loma Linda University Children's Hospital. SHS=second-hand smoke; SIDS=sudden infant death syndrome; OB, obstetric; NICU, neonatal intensive care unit.
Phillips et al. conducted a randomized trial targeting mothers with a history of smoking whose infants were admitted to the LLUMC NICU. We used motivational interviewing during one-on-one counseling and educational video presentations, while focusing on infant cues and development. With these strategies, there was a significant reduction in smoking relapse rates from 81% to 46% and an increase in breastfeeding rates from 21% to 86%. 61 (Fig. 2).
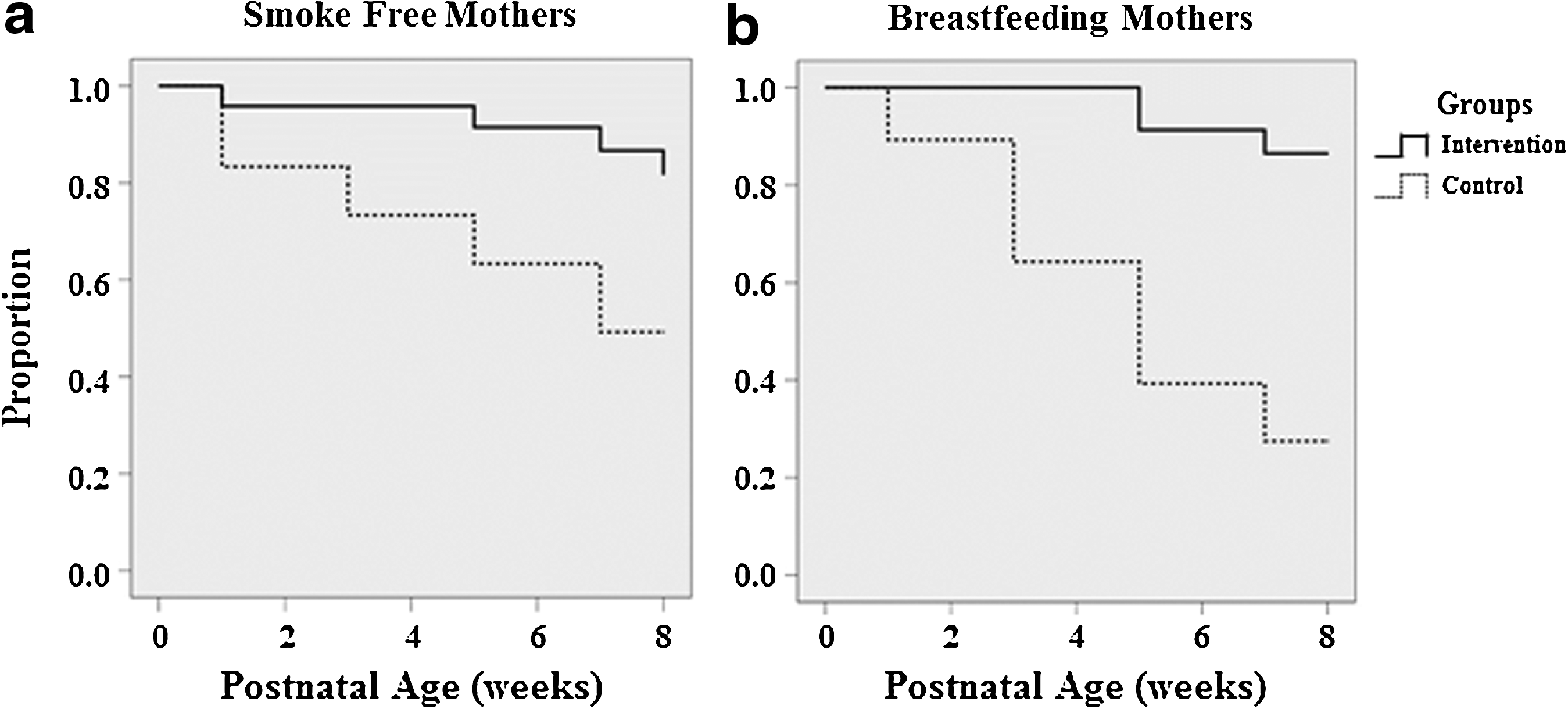
Prevention of postpartum smoking relapse by RM Phillips et al.61
Despite the positive effect of programs employing educational and supportive interventions, tobacco dependency makes it very difficult for most pregnant women to stop smoking, especially those moderate to severe levels of tobacco dependence (a Fagerström Test for Nicotine Dependence of 5 or more). To assist clinicians in their efforts, the American College of Chest Physicians created a Tobacco Dependence Treatment Toolkit in 2010 that summarizes current evidence regarding recommendations for pharmacologic treatment in a subsection titles “Smoking and Tobacco-Dependence Treatment for Pregnant Women and Women of Childbearing Age.” 71 This toolkit concludes that tobacco-dependence pharmacotherapy presents “a lower risk to the fetus than the significant harm caused by the mother's continued smoking,” and recommends that the physician needs to balance the risk of pharmacotherapy against the substantial risk of continued exposure to tobacco smoke. In terms of treatment, after careful risk assessment and behavioral counseling, prescribing bupropion (Class C) as the second intervention and use of nicotine replacement therapy (NRT; Class D) in its various forms as a third alternative. Combination therapy using bupropion and nicotine medications are recommended as a fourth choice. While Varenicline is rated Class C, it is advised that this drug should be reserved when these older standard medications are ineffective to achieve abstinence.
The U.S. Prevention Services Task Force has concluded that NRT and other pharmaceuticals to assist pregnant women to stop smoking have not been completely evaluated for either efficacy or safety. 72 The U.S Surgeon General advises caution regarding use of these drugs in pregnant women, while in the United Kingdom, the National Health Service endorses the use of NRT with guidance.73,74 In September 2011, the ACOG issued a technical bulletin that recommended against the use of NRT and other drugs to assist pregnant women to stop smoking. 54 Given the conflicting options, we believe that a thoughtful risk-benefit assessment should be adopted given the risk to the fetus and mother compared to her continued smoking. Obstetricians might ask which is safer for the fetus—the mother who continued smoking exposing her fetus to higher nicotine levels (than would be experienced with nicotine replacement therapy) plus the extraordinarily high carbon monoxide levels with exposure to high levels of other toxins in tobacco smoke versus a few weeks of effective medications to eliminate maternal and fetal risks in second and third trimesters.75,76
In the end, tobacco-dependency treatment is a cost-saving endeavor. Neonatal healthcare costs attributed to tobacco use during pregnancy have been estimated to be more than US$367 million annually. 77 To assess fully the economic impact of successful tobacco-dependency treatment, it is necessary to analyze both the cost-effectiveness of perinatal tobacco-dependency counseling and the overall effectiveness of tobacco-dependency counseling when provided by trained counselors, certified nurse midwives, or physicians compared to stop smoking efforts via a clinical trial or quit line. Assuming the time per counseling session ranges from 5 to 13 minutes at an estimated cost of $24–34 per session, if there is a 30% increase in the maternal stop-smoking rates, then $881 will be saved per maternal smoker, and there will be a reduction of $5–11 million (2006 dollars) worth of excess neonatal costs. Ruger and Emmons in eight studies analyzing benefit–cost ratios for tobacco-dependency treatment programs during pregnancy and for tobacco relapse prevention programs found that for every $1 invested in such services, $3 were saved in downstream health-related costs. 78
Obstetricians, pediatricians, and neonatologists need to work together in their efforts to assist and educate not only mothers, but also their partners/spouses and families in reducing environmental tobacco-smoke exposure of infants. There remain serious gaps in knowledge (Table 1) and in the application of professional guidelines by both obstetricians and pediatricians in helping mothers and fathers in their efforts to reduce infant exposure to second- and third-hand smoke. With the identification of pregnant smokers, it is imperative that they be supported to stop smoking early in their pregnancies through interventions by their physicians or midwife and asked at each prenatal visit about any tobacco exposure. Current smokers should have their tobacco dependence assessed using a validated scales such as the Fagerström Test for Nicotine Dependence. As mental health morbidities impact tobacco-dependence treatment, mental health problems should be inquired about and a scale of symptoms of depression administered. Both obstetricians (or midwives) and pediatricians need to emphasize the danger of second- and third-hand smoke exposure to their infants and ensure that postpartum follow-up is continued during pediatric care for their infants and the mothers' follow-up visits. As pediatricians and neonatologists, it is our duty to protect infants from second- and third-hand smoke exposure by carrying through on interventions started during pregnancy and involving fathers to commit to maintaining a tobacco-free home and car. Education, motivation, use of pharmacologic therapy, and ongoing support by continuing to Ask, Assist, and Refer and taking the extra 5–10 minutes to reinforce positive decisions made by parents should be high priority for pediatric providers. Further, the often-extended stay in the NICU for some infants (and visits by their parents) offers the opportunity to engage parents with additional opportunities for infant attachment and further education regarding the absolute necessity to rear their infant in a tobacco-free home and car.
The ball is in our court: we must protect the most vulnerable in our society from the hazards of tobacco-smoke exposure throughout fetal development, infancy, and childhood. This dismissal of our role in preventive healthcare and active intervention for pregnant women and their infants is intolerable in a society that values women and their pregnancies that produce our future generations of children.
Footnotes
Author Disclosure Statement
No competing financial interests exist.