
Abstract
Abstract
Purpose:
To investigate the association between pancreatic neuroendocrine tumors (panNETs) and sinistral portal hypertension (SPH) and provide insights into the pathogenesis.
Methods:
A retrospective review of panNETs was conducted from our institution for 12 years. Medical imaging findings were analyzed to determine any association with splenic vein thrombosis (SVT) at diagnosis. The cases were further selected based on the criteria for SPH, namely, (1) presence of SVT, (2) gastric varices, (3) patent portal vein, and (4) normal liver function tests.
Results:
There were 61 patients with panNETs and 8 (8/61) had SVT and gastric varices at diagnosis. Four (4/8) met the strict criteria for SPH while the other four had more conventional portal hypertension. The four with SPH had large tumors located in the tail with splenic vein invasion and three of four presented with bleeding gastric varices. All four patients underwent surgical resection. Mean follow-up was 8.5 years and the hematemesis never recurred. The other four patients (four of eight) with gastric varices had unresectable disease and all died after a mean survival of 29 months.
Conclusion:
PanNETs appear to be more commonly associated with SVT and SPH compared with other tumors. This could be related to their relatively indolent nature and their intrinsic vascularity. From a surgical viewpoint, the decision to operate depends on many factors including but not limited to the size/stage, grade, and functionality of the tumor and comorbidities. These considerations notwithstanding, the association between panNETs and SPH suggests that there is benefit in timely resection of panNETs located in the tail.
Introduction
Sinistral portal hypertension (SPH) is a localized or left-sided form of extrahepatic portal hypertension that may lead to gastric variceal hemorrhage. The pathogenesis of SPH is related to splenic vein thrombosis (SVT), which causes retrograde blood flow through the short and posterior gastric and gastroepiploic veins.1–4 In contrast to conventional portal hypertension, the features of SPH occur in the absence of chronic liver disease.
The most common causes of SPH are chronic pancreatitis, pseudocysts, and pancreatic tumors.1–8 In the case of chronic pancreatitis, the mechanism relates to fibrosis with resultant compression of the splenic vein. For pancreatic neoplasms, the most common tumor is ductal adenocarcinoma. It is an aggressive malignancy and the mechanism for SPH in this case is direct invasion or encasement of the vessels by the tumor. Since this tumor has such a dismal prognosis with a mean survival of <12 months,9,10 SPH is generally a lesser consideration in the management of these patients. Conversely, pancreatic neuroendocrine tumors (panNETs), as a group, are relatively indolent tumors and the patients can live for many years even with metastatic disease.9–11
A review of the literature shows that most studies on SPH and pancreatic tumors are case reports or small series.12–21 However, an analysis of these studies suggests that panNETs are disproportionately cited with regard to SPH compared with other benign or low-grade pancreatic tumors. In this report, we reviewed panNETs focusing on those complicated by SVT and SPH, and we were interested in ascertaining the mechanistic basis for this association.
Methods
Patient selection
The study received approval from our institutional review board. The records of our pathology department were searched for all cases of panNETs between 2002 and 2016. More detailed information about the clinical history, medical imaging, laboratory findings, patient management, and follow-up was obtained from the hospital's electronic medical records.
Pathology
The diagnosis of panNET was based on routine hematoxylin and eosin slides. In select cases, additional stains such as Congo red and Masson trichrome were utilized. Immunohistochemical assessments of the neuroendocrine markers synaptophysin and chromogranin A were conducted on a representative block from the surgical biopsy, resection, or cytology specimens as previously described. 22 In some cases, additional stains were used to further substantiate the immunohistochemical profile or diagnosis, for example, insulin, somatostatin, glucacon, gastrin, and serotonin.
Medical imaging
The medical imaging findings of the panNET patients were reviewed to determine whether any were associated with SVT at the time of diagnosis. All patients underwent computed tomography (CT) of the chest, abdomen, and pelvis with intravenous (IV) contrast enhancement. A few selected cases had magnetic resonance imaging or ultrasound depending on their clinical status. All the cases were performed with IV contrast and most with a dedicated multiphasic pancreatic cancer protocol. Case 1 (Fig. 1A) was scanned with pancreatic parenchymal phase and portal venous phase (kV120, mA280, slice thickness 2.5 mm, and 5 mm on a GE Lightspeed Plus CT Unit [GE Healthcare, Milwaukee, WI]). The corresponding surgical resected specimen is shown in Figure 1B. Case 2 had a contrast-enhanced abdominal magnetic resonance (Fig. 2) with coronal and axial postgadolinium contrast T1-weighted Vibe FS images (repetition time [TR] 4.64, echo time [TE] 2.4, 240 × 320 mm field of view, 3 mm slice thickness, on a Siemens 1.5T TRIO Unit [Siemen Medical Systems, Erlangen, Germany]) and axial T2-weighted turbo spin echo images (TR 3206, TE 81, 240 × 320 mm field of view, 5 mm slice thickness). Majority of the patients underwent Octreotide scan with SPECT CT (In-111 chelated to octreotide using diethylenetriaminepentaacetic acid [In-111 penetetreotide] as part of their work-up (images not shown).


Case 2. This figure shows coronal and axial MR image with fat saturation and contrast in the portal venous phase, and axial T2-weighted images (bottom row). A large invasive m arising from the tail of the pancreas extends into the hilum of the spleen. The direct invasion of the spleen from the pancreatic tail invades and obstructs the splenic vein from the level of the pancreatic tail. The splenic vein is obliterated at the splenic hilum and not visible. A large gev shunts venous blood from the spleen back into the patent portal vein through collaterals in the pancreatic head. The dilated and enhancing gev is easily seen on postcontrast MR images running in a tortuous course inferior to the greater curvature of the stomach. MR, magnetic resonance.
Results
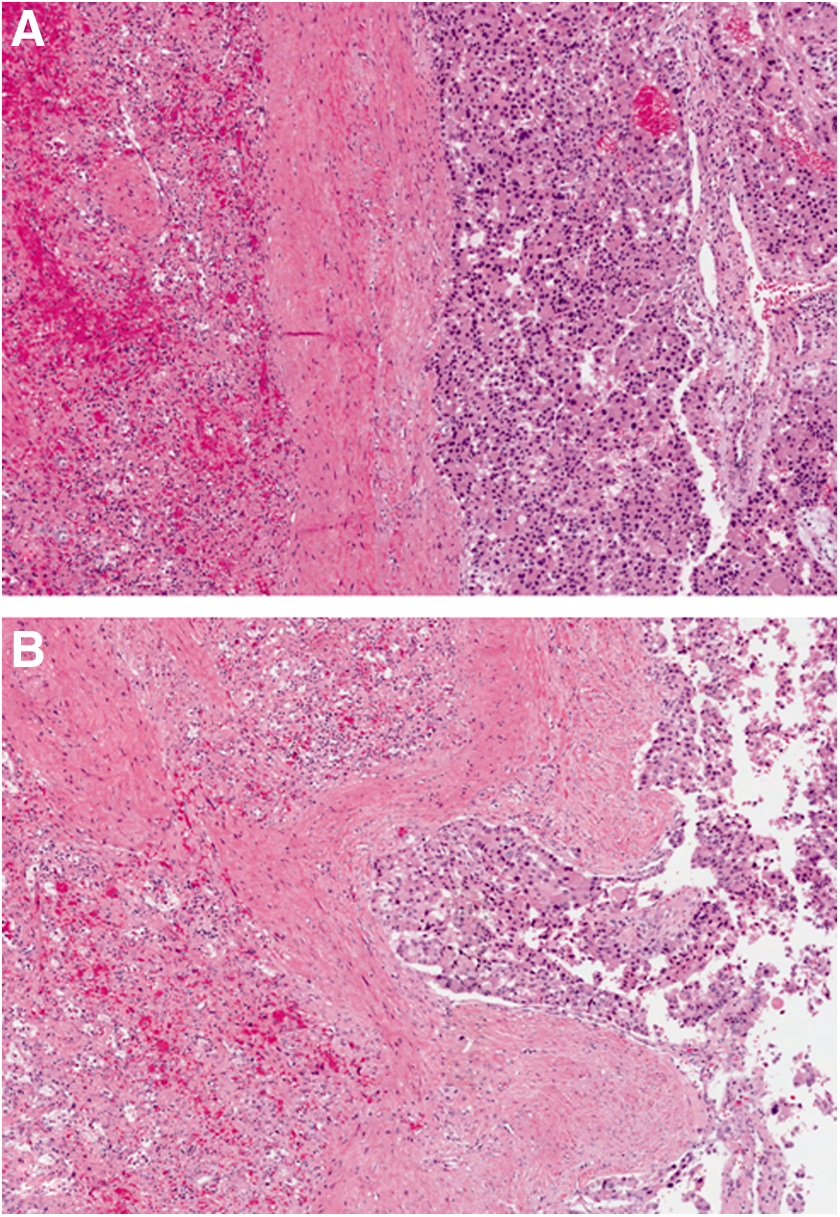
A total of 61 patients with panNETs were identified. Eight of them (8/61) were found to have SVT and gastric varices at the time of diagnosis (Table 1). Of these, four (four of eight; cases 1, 2, 7, and 8) met the strict criteria for SPH as defined by the presence of SVT, gastric varices, patent portal vein, and normal liver function tests.1–6 Three of these patients presented with hematemesis from bleeding gastric varices. They were resuscitated and stabilized. Patient 8 presented with abdominal pain but without a variceal hemorrhage. After work-up, all four patients underwent distal pancreatectomy and splenectomy with partial gastrectomy. The tumors were large with a mean maximum dimension of 9.7 cm (Figs. 1 and 2). They were located in the tail (Fig. 3A,B) with extrapancreatic extension and invasion and thrombosis of the splenic vein (Fig. 4A,B).

DPSPG, distal pancreatectomy and splenectomy with partial gastrectomy; F, female; GI, gastrointestinal; Liv, liver; M, male; Panc, pancreas;
Microscopy of all the eight cases with SVT showed that the tumors had characteristic features of panNETs—an organoid morphology with some areas having a trabecular pattern, others being diffuse, gyriform, or nested (Fig. 3A,B). The cells had round to oval nuclei with variable pale to amphophilic cytoplasm. Mitotic activity was low, ranging from 1 to 3 per 10 high-power fields, except for case 3 that showed 5. In all the eight cases with SVT, the Congo red stain for amyloid was negative. By immunohistochemistry, the stains for insulin, somatostatin, glucagons, gastrin, and serotonin were negative. The Ki-67 labeling index was determined using the camera-captured/printed image method. 23 Using the 2017 World Health Organization classification, seven of the eight cases were classified as well-differentiated panNETs, grade 2,24,25 and one as grade 3 (Table 1).
Patient 1 was staged as pT3N0M0 (American Joint Commission for Cancer). The surgical margins were clear but with narrow clearance. Since he was only 42 years old and the tumor was relatively large with narrow margins, he was given adjuvant radiotherapy to the tumor bed to reduce the possibility of local recurrence. The gastric varices never recurred, but 2 years postsurgery he developed liver metastases that were managed by radiofrequency ablation and chemotherapy. He did well as his disease was kept under control for many years. He eventually succumbed to metastases 13.2 years after his surgery.
For patient 2, based on preoperative imaging, it was determined that curative resection was unlikely; however, surgery was undertaken with the intent of preventing further variceal bleeding. The pathology specimen was staged as pT3N1M1 with the M1 being attributed to a separate wedge resection of diaphragm that was positive for tumor. He also had positive surgical margins. He was treated with postoperative chemotherapy. Approximately 1 year after surgery, he developed small volume metastatic liver disease that appears to have been controlled by chemotherapy and thus far has been nonprogressive. He is now >3 years postsurgery, and the varices have not recurred.
Patient 7 had varices that were glued at endoscopy. He then underwent surgery and was found to have positive margins postresection. Owing to a concurrent psychiatric illness and other comorbidities, he was not given any postoperative chemo- or radiotherapy. One year after resection, the varices have not recurred and the disease has not progressed. He remains under watchful observation.
Patient 8 presented with abdominal pain and was found to have a pancreatic mass. It was resected with clear margins. Eight months later, he is alive and well with no evidence of disease or varices.
The other four patients (four of eight) with SVT and gastric varices (patients 3–6) already had liver metastases with portal hypertension and/or portal vein thrombosis. All these four patients had unresectable disease and were mainly treated with chemotherapy. They died of disease or other causes with a mean survival of 29 months.
Discussion
This is a retrospective review of 61 patients with panNETs for a 12-year period. Eight of these patients were found to have SVT and gastric varices but only four fulfilled the strict criteria for SPH.1–6 In all four patients, the tumors were relatively large, located in the tail with extrapancreatic extension and invasion of the splenic vein. Even though there were no liver metastases, the extensiveness of the locoregional disease augered against a curative resection. However, since three of these patients had presented with life-threatening hematemesis, surgical resection was necessary irrespective of whether it was curative or debulking/palliative. It turned out that in one case, there was complete surgical clearance although with narrow margins, whereas the other two cases had positive margins. It is noteworthy that the varices and hematemesis never recurred after a mean of 54.9 months postsurgery. The surgical resection and splenectomy decompress the splanchnic venous pressure in this region, which effectively removes a life-threatening complication and thus prolongs survival and quality of life.1–8
SPH can occur in various conditions, both non-neoplastic and neoplastic. The most common non-neoplastic association is with chronic pancreatitis and the mechanism here relates to fibrosis.1–8 In those cases of pancreatitis complicated by pseudocyst formation, the pseudocyst itself can cause compression of splenic vein.1–4,12 The neoplastic associations include not only pancreatic tumors such as panNETs,11–21 solid pseudopapillary neoplasms, 26 mucinous 27 or serous cystadenomas, 28 and ductal adenocarcinoma2,6 but also nonpancreatic neoplasms, for example, renal cell carcinoma 29 and colonic lymphoma, 30 and even ectopic spleen. 31 Nonetheless, pancreatic tumors, particularly panNETs tumors,11–21 are more commonly implicated than others. In this report, we document additional cases of panNETs that were complicated by SPH and upper gastrointestinal hemorrhage.
The fact that panNETs (∼1–2% of pancreatic tumors)9–11 are more commonly cited in relation to SPH than ductal adenocarcinomas (85% of pancreatic tumors)9,10 or any other tumors for that matter suggests that the pathogenesis of SPH may not simply be based on the invasion or compression by tumor. It could be due to the secretion of fibrogenic neurohormonal substances in much the same way that small bowel NETs secrete serotonin and other biogenic amines that cause mesenteric fibrosis, kinking of the bowel, vascular sclerosis, ischemia, and tricuspid stenosis.24,32,33 However, our patients did not manifest the carcinoid or other functional neurohormonal syndromes, and the tumors were negative for serotonin, insulin, somatostatin, and glucagon.
Conventional portal hypertension 34 has been associated with hepatic amyloidosis. 35 Since panNETs can produce amyloid36,37 (Apud amyloid), we were interested in whether this could be a factor in the pathogenesis of SVT and SPH. However, all eight of our cases with SVT were negative for amyloid. We, therefore, hypothesize that the predisposition of panNETs to SVT and SPH may simply be related to the intrinsic vascularity 38 of these tumors just like other NETs in general. In the face of SVT, such vascularity could exacerbate blood flow and backpressure on short gastric and gastroepiploic veins.
Despite recent advances in the medical management of panNETs with newer drugs such as octreotide, sunitinib, and everolimus,39,40 surgery remains the mainstay of treatment. That being said, many considerations have to be factored into the decision to operate. They include but are not limited to the size/stage, grade, and functionality of the tumor and surgical comorbidities.41–44 These considerations notwithstanding, our study suggests that there is benefit to timely resection of panNETs located in the tail. Furthermore, even in patients wherein a curative resection is not possible, palliative resection with splenectomy can improve the quality of life and outcomes.
In summary, it would appear that panNETs are more likely to get complicated by SVT and SPH than other pancreatic neoplasms. This may be related to their relatively indolent nature and intrinsic vascularity. Although this proposed hypothesis is more germane to the four cases that strictly meet the criteria of SPH, mechanistically it could to some extent also apply to the other four panNETs with SVT and conventional portal hypertension.
Footnotes
Author Disclosure Statement
No competing financial interests exist.