
Abstract
Abstract
Background:
Pancreatic cancer is an aggressive and malignant disease that usually presents as an isodense or hypodense lesion with no significant enhancement in contrast CT. CT scan plays an important role in the diagnosis of pancreatic diseases, especially in pancreatic cancer and pancreatic neuroendocrine tumors.
Presentation:
This report includes a case of a 53-year-old female patient presenting a high-density mass in the pancreas on contrast CT. The mass was surgically removed, and the pathology confirmed the diagnosis of pancreatic adenocarcinoma.
Conclusion:
Sometimes the contrast CT of pancreatic cancer can be expressed as high density, which is similar to pancreatic neuroendocrine tumors. It is necessary for us to identify carefully.
Introduction
Pancreatic cancer is often characterized as an insidious, rapid progress, unsatisfactory response to treatment and a very poor prognosis. Recent epidemiological investigation has suggested an increased incidence in many countries. Nowadays, radical surgery is still the only way to cure pancreatic cancer in clinical practice. Pancreatic neuroendocrine tumors (PNETs), a minor group of benign or malignant tumors with different clinical and pathological manifestations, have been the focus of research in recent years. According to the biological characteristics, PNETs can be divided into “functioning” and “nonfunctioning” types. In clinical practice, insulinoma and gastrinoma are relatively common. The following is a case of PNET before the operation, which was modified as pancreatic cancer by a postoperative pathological test.
Case Presentation
A 53-year-old female patient had suffered from unusual fatigue resulting from manual work or emotional stress for 6 months before her hospitalization in April, 2013. She neither had history of diabetes or pancreatitis, nor did she smoke or drink. She was found with no medical history except left shoulder lipoma resection.
Initial laboratory results showed normal corrected calcium and amylase with unremarkable hematology and biochemistry results. Tumor markers, such as AFP, CA19-9, CA125, were all within normal range. Physical examination did not reveal any positive findings.
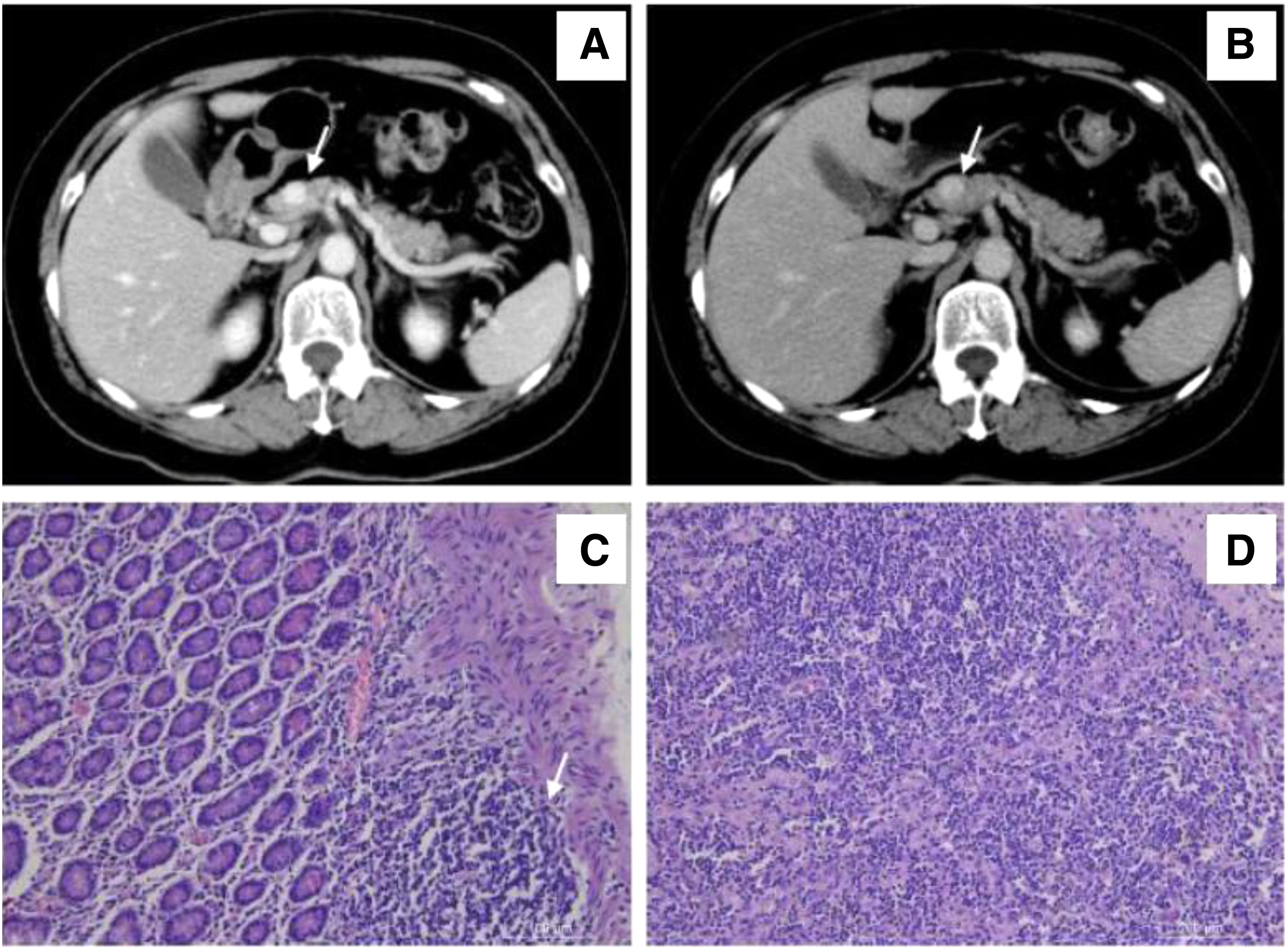
An abdominal ultrasound that diagnosed a 1-cm mass inside the pancreas was first performed. The size and shape of the pancreas were normal with no dilatation of the main pancreatic duct. Contrast abdominal CT demonstrated a small nodule in the head of the pancreas, about 1.08 cm in diameter, with a CT value of about 42 HU. A contrast-enhanced scan showed significant enhancement. The CT values were 104, 143, and 105 HU in the three stages (Fig. 1A, B). The nodule was considered a pancreatic islet cell tumor. During the next 6 months, the patient received upper abdomen CT scan every 3 months. The nodule did not enlarge significantly. However, the patient and her family members strongly argued for surgery. Therefore, surgery for tumor resection was scheduled.
The patient underwent “pancreatic exploration and pancreatic head tumor resection” under general anesthesia on April 11, 2013, after relevant examination and preoperative assessment. During the operation, the mass was observed to be located in the back of the pancreatic neck, about 1.5 cm in diameter, hard in texture. No ascites or intra-abdominal adhesions were observed. Since the tumor was large in size, it was feared that simple tumor enucleation might result in pancreatic fistula. Thus, the surgeons performed pancreatic head resection.
Intraoperative frozen section reported abundant fibrous tissue, deformed glands and ducts, cellular atypia inside the tumor. The preliminary diagnosis was adenocarcinoma. After informing the patient's family members of this finding, surgeons decided to perform a pancreaticoduodenectomy. The final pathological report (Fig. 1C, D): a mass from the pancreatic neck, about 1.1 × 1.1 × 1.0 cm in size, gray insection surface, hard texture, with a clear boundary and no envelope. Microscopically, the normal pancreatic tissue structure was replaced by cells of abnormal hyperplasia with obvious atypia, pink cytoplasmic staining, increased nuclear/cytoplasm ratio, darkly stained nucleus, and obvious polymorphism. Mucus secretion was visible in some parts. The glandular cells were arranged in streaks and grew invasively. No lymph node metastasis was reported in any of the specimens.
The patient recovered well postoperatively with no recurrence or metastasis during the 30 months of follow-up.
Discussion
Pancreatic cancer is aggressive and highly malignant. Due to the lack of specific clinical manifestations at early stage, 80% of the cases have reached an advanced stage by the time of initial assessment and miss the optimal opportunity of radical surgery. Resection is the only potentially curative option for pancreatic cancer. 1 Early diagnosis is of dramatic significance for pancreatic cancer patients if the tumor can be discovered when localized and nonmetastatic.
Pancreatic endocrine tumors, also called PNETs, are another kind of pancreatic tumor, most of which are benign or low malignant potential tumors. About 75% of the pancreatic endocrine tumors are nonfunctional. It is classified as many types according to endocrine hormone. The latest research has showed that small NF-PNETs without metastasis can be observed with a low level of evidence. 2 However, to the same condition of pancreatic cancer, surgical resection should be performed as soon as possible.
In the present case, the patient was challenging before the surgery, mainly due to the following reasons: (1) the patient was a middle-aged women. The tumor markers were within the normal range. Despite the lesion in the head of the pancreas, no dilated pancreatic duct and jaundice were presented. (2) During the 6 months before surgery, the nodule did not enlarge significantly according to the upper abdomen CT scans twice. Apart from occasional fatigue, the patient did not have weight loss nor other symptoms of consumption. (3) Contrast abdominal CT showed a small nodule in the head of the pancreas, about 1.08 cm in diameter, with a CT value of about 42 HU. Enhanced scan showed significant enhancement. The CT values were 104, 143, and 105 HU in the three stages. Most importantly, the enhanced CT scan showed significant enhancement, which directly leads to the misdiagnosis of a PNET, rather than a pancreatic ductal adenocarcinoma.
Normal pancreatic tissue is extremely rich in blood flow. Pancreatic cancer damages the surrounding normal tissues. The tumor cells are dispersed between the residual pancreatic tissue and fibrous mesenchyme. The intimal hyperplasia, arteriosclerosis, and involvement of small arteries around the tumor lead to a significant decrease in blood flow in the cancer tissue. Therefore, pancreatic tumor usually presents as the equal-density or low-density lesions with no significant enhancement in contrast CT.3–5 However, PNETs are composed of hypervascular tissues, which present as high-density lesions in contrast CT. In most conditions, contrast-enhanced CT is enough to confirm a pancreatic mass. 4
After the operation, the authors reviewed the medical history and imaging information and communicated with the radiologists. Our patient had unusual CT imaging and untypical manifestations. Clinicians should be even cautious in future work. We also searched the relevant documents and found no description of pancreatic cancer presented as a high-density lesion via enhanced CT, although we ended up with rare cases.
The early diagnosis of pancreatic cancer is very important. Resections in early phase can prolong the survival time and improve the patients' quality of life. This case suggests that, in the future clinical work, enhanced CT found that high-density nodules in the pancreatic head region should be considered for pancreatic cancer. The case also suggests that radiological checks should be completed before the operation. For major surgery such as pancreas resection, MR examination may be routinely performed. When necessary, PET-CT can be used to avoid blind operation.
Footnotes
Acknowledgment
National Natural Science Foundation of China (81373875), (81072918), (LNCCC-A03-2015).
Authors' Contributions
H.X. and Q.Z. searched the database and wrote this article. They are cofirst authors. X.G. made the pathological diagnosis and managed the pathological pictures. D.S. supervised the methodology and the writing of the article. D.S. is the corresponding author of this article. All authors have read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.