
Abstract
Abstract
Background:
Insulinomas are a rare entity commonly treated by resection. Central pancreatectomy represents an uncommon type of resection for pancreatic lesions.
Case Presentation:
A 77-year-old female underwent a central pancreatectomy with Roux-en-Y pancreaticojejunostomy and pancreatic stump oversew after presenting with symptoms of hypoglycemia concerning for an insulinoma. Her hospital course was uncomplicated and her symptoms resolved after resection.
Conclusion:
Resection of insulinomas is the preferred approach of treatment, and resection by central pancreatectomy is a safe option for benign lesions in the neck of the pancreas.
Introduction
Pancreatic neuroendocrine tumors (PNETs) are rare entities of the endocrine pancreas with poorly understood progression. PNETs represent 3% of pancreatic neoplasms and insulinomas account for 3% of all PNETs. 1 Insulinomas are commonly sporadic but sometimes arise within the setting of multiple endocrine neoplasia-type 1. 2 Symptoms that accompany insulinomas are related to hypoglycemia and include confusion, dizziness, behavioral changes, seizures, visual disturbances, weight gain, and, in severe cases, coma.
Resection of pancreatic tumors is determined by location of the lesion within the pancreatic gland. Enucleation is the preferred approach to excising PNETs; however, tumors that arise in the head of the pancreas are often resected by pancreaticoduodenectomy and lesions arising in the body or tail of the pancreas are typically resected by distal pancreatectomy. Central pancreatectomy for lesions in the neck and proximal body of the pancreas is performed much less frequently, but has been shown to be a safe operation that preserves maximal pancreatic endocrine and exocrine function while avoiding the morbidity and mortality associated with pancreaticoduodenectomy. 3
In this study, we present a case of an insulinoma resected through central pancreatectomy with pancreaticojejunostomy.
Presentation of Case
The patient is a 77-year-old female who presented with symptomatic hypoglycemia in September 2016. She had a 2- to 3-year history of syncopal and near-syncopal events. Three years prior, she had a neurological work-up for an episode of seizures, was diagnosed with a seizure disorder, and was started on lamictal. During a recent trip to the emergency department 1 month before presentation, her blood glucose was found to be 20 mg/dL and a computed tomography (CT) scan of the abdomen and pelvis was obtained. Although the CT was initially read as normal, there was a hypervascular mass evident in the neck of the pancreas. She underwent a follow-up octreoscan, which was negative. She subsequently had a set of synchronous laboratories that were significant for a serum glucose of 55 mg/dL, a c-peptide level of 2.87 ng/mL, and an insulin level of 6.6 mcU/L. Her carcinoembryonic antigen, CA19-9, and bilirubin levels were normal. She underwent an endoscopic ultrasonography that showed an 8 mm mass thought to be in the head of the pancreas. Her CT scan was reviewed at her initial outpatient consultation visit, and she was noted to have a hypervascular mass in the central pancreas with no evidence of dissemination (Fig. 1). The clinical impression was that she had an insulinoma located in the central pancreas that was causing her hypoglycemic episodes and symptoms, which were previously attributed to a seizure disorder.

Computed tomography scan at the initial presentation.
The patient underwent central pancreatectomy with Roux-en-Y pancreaticojejunostomy and right-sided pancreatic stump oversew in September 2016. Intraoperative ultrasonography identified a 9-mm hypervascular lesion in the neck of the gland (Fig. 2). Enucleation of the lesion was initially attempted; however, it appeared to traverse the entirety of the gland from the anterior to posterior pancreas, taking up most of the neck of the pancreas and dilating the pancreatic duct. Given the potential risk of damaging the pancreatic duct in the process, enucleation was abandoned. Distal pancreatectomy and an extended Whipple procedure were also considered, but the patient would lose a large amount of normal functioning gland with both options. Therefore, central pancreatectomy was ultimately chosen as it allowed for the most amount of normal pancreatic parenchyma to be preserved.
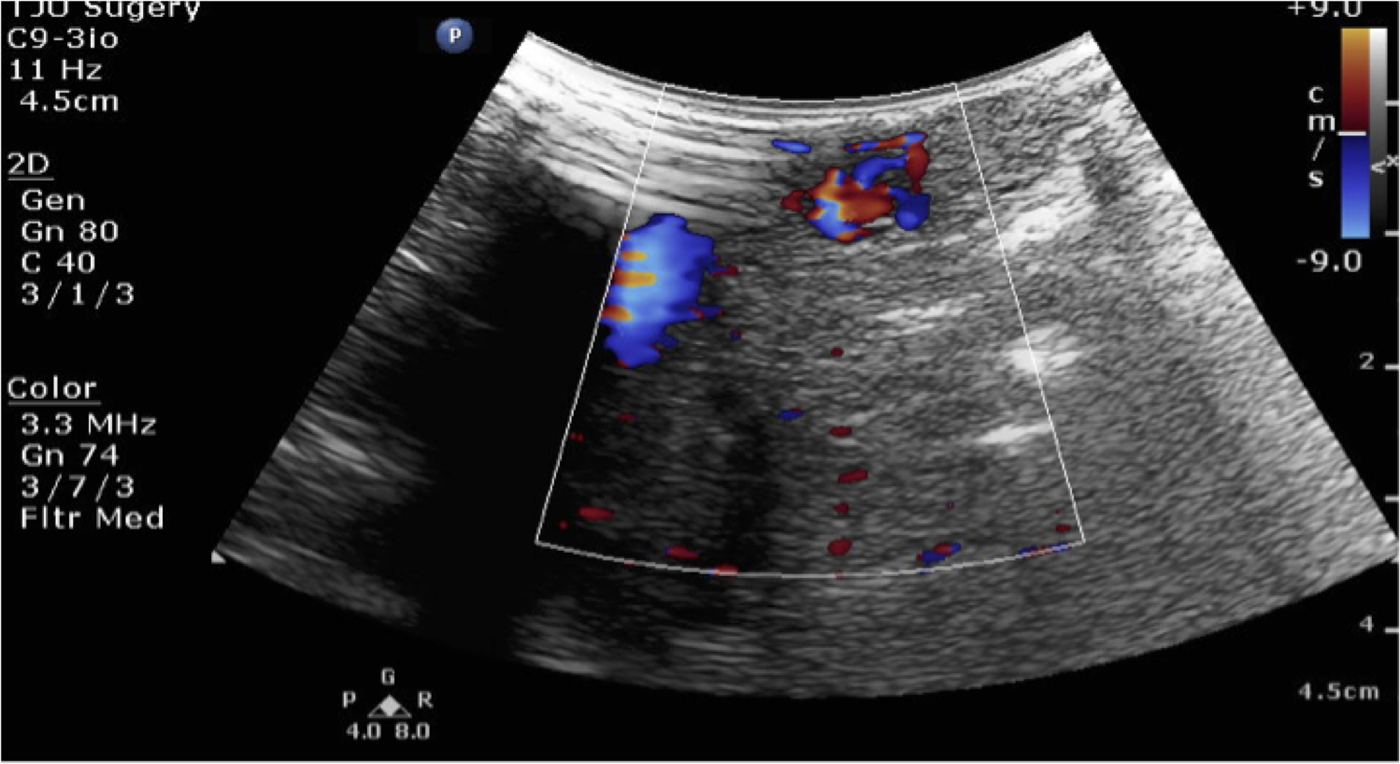
Intraoperative ultrasonography identified a 9 mm hypoechoic hypervascular mass in the neck of the pancreas. No additional lesions were present.
The lesion proved to be a well-differentiated low-grade neuroendocrine tumor that stained positive for insulin expression on immunohistochemistry, with negative margins. Her postoperative hospital course was uncomplicated and she was discharged on postoperative day 7. She remained euglycemic throughout her postoperative course and her seizure medication was discontinued, under the presumption that her seizures were likely because of the insulinoma. During her follow-up visit in the office, she revealed that she was no longer having syncopal events or seizures despite being off her seizure medication, and had begun to lose weight since her operation.
Discussion
The diagnosis of a pancreatic insulinoma can be challenging. Nikfarjam et al. 2 found that the most common presenting symptoms of an insulinoma were nonspecific and included confusion, visual disturbances, diaphoresis, fatigue, and weight gain. These symptoms were often present for 18 months before diagnosis. 2 Syncope and seizures, which were the presenting symptoms for our patient, were found to be present in only 13% and 16% of patients, respectively. 2 The diagnostic criteria of an insulinoma include low blood glucose, elevated serum insulin, and elevated C-peptide levels. CT imaging has been found to be the most successful technique for preoperative localization of an insulinoma, with a sensitivity of 80%. 2 Intraoperative ultrasonography was able to detect the lesion in 82–85% of cases.2,4 Insulinomas have been found to be relatively evenly distributed throughout the head, body, and tail of the pancreas. 2 Insulinomas in the neck of the pancreas, as in our case, represent only 9% of all insulinomas. 2
Prognosis after resection of an insulinoma is generally very good. Bilimoria et al. determined that patients with functional tumors, tumors <4 cm, node-negative tumors, absence of metastasis, and well-differentiated histology had better 5-year survival. 1 Nikfarjam et al. found that patients with resected insulinomas had a 10-year disease-specific survival of 100%. 2 Medical management of insulinomas is almost never chosen as the first-line of treatment because of the potential for malignant transformation of an insulinoma, which has been shown to occur in up to 10% of patients.2,4
The most common procedure to remove a pancreatic insulinoma is enucleation.1,2 Central pancreatectomy is rarely performed. For our patient whose tumor was localized to the neck of the gland, we performed central pancreatectomy with Roux-en-Y pancreaticojejunostomy to preserve maximal pancreatic endocrine and exocrine function. In a study on central pancreatectomy with pancreaticogastrostomy, the most common complication was pancreatic fistula, which was found to occur in up to 36% of patients; however, these fistulas were able to be managed conservatively with drains. 3 Postoperatively, patients were found to be without evidence of pancreatic insufficiency, leading to the conclusion that central pancreatectomy is a safe procedure for benign lesions in the central pancreas. 3
As exemplified in this case report, insulinomas may present with nonspecific symptoms for a long duration of time. Localization is best achieved by CT scan and intraoperative ultrasonography. Central pancreatectomy with pancreaticojejunostomy is a safe option for patients with insulinomas located in the neck of the pancreas.
Footnotes
Author Disclosure Statement
No competing financial interests exist.