
Abstract
Asthma morbidity in pediatric patients can be significantly reduced through the coordinated efforts of asthma care clinicians, families, and schools. The efforts of asthma care clinicians and schools, both individually and collectively, should address the medical and psychosocial needs of the patient. The synergy created by each playing an active role in pediatric asthma management assists the patient in gaining adequate asthma control. In addition to writing asthma action plans for their patients, clinicians can work with schools more effectively by focusing their efforts on the following key actions: promoting asthma-friendly schools; identifying school-aged children with asthma; educating patients and school staff about asthma; assisting patients, families, and schools in reducing exposure to environmental triggers; assisting the school staff in helping students manage their asthma at school; and playing an active role in monitoring and coordinating care with schools and families by working closely with care coordinators/case managers. School-based asthma management programs can assist families and asthma care clinicians in achieving good asthma control for school-aged patients. This article reviews recent research findings and provides guidance for asthma care clinicians on how to enhance a full range of school-based asthma management for their patients.
Introduction
A
Although asthma cannot be cured, it can be controlled through evidence-based care with self-management, use of an asthma action plan that includes appropriate medications, and avoidance of environmental triggers for asthma, such as irritants (smoke, strong chemicals) and allergens (dust mites, warm-blooded pets, mold, and pollen).8 Trigger avoidance should focus on the triggers to which a child is sensitive/sensitized. In 2007, the National Asthma Education and Prevention Program (NAEPP) Expert Panel Report 3 (EPR-3)9 emphasized the importance of focusing on asthma control, and the Guidelines Implementation Panel Report10 stressed the need for implementation of guideline-based care across the clinical and community spectrum. Clinicians, families, and schools are all important links in this chain. For children with severe or difficult-to-control asthma, it may “take a village” to achieve asthma control, and school-based asthma management can be a key component. Several well-designed randomized controlled studies have documented that school-based services, including supervised administration of long-term controller medications at school, can help to address poor adherence to recommended treatment regimens, especially among economically disadvantaged youth with asthma.11–15 The success of school-based programs for asthma management is dependent on a partnership with families and the health-care system.16 Collaboration between community clinicians and school physicians, such as the use of telemedicine technology for communication by physicians in partnerships with schools,17 is an effective approach to ensuring that families receive consistent messages from all asthma care clinicians.18–21
Although many studies have documented excessive school absenteeism caused by asthma,22,23 recent studies have shown that the percentage of attendance among students with asthma can equal that of students without asthma when the former receive evidence-based care that includes school-based asthma services.24,25 Examples of evidence-based school asthma services include having a full-time nurse, or having a school-based health clinic. Conversely, other schools may have no health care personnel available and may use aides or office staff for health services. The variability of school-based asthma services across the United States 26 makes it critical for asthma care clinicians to determine what is happening in their patients’ schools and advocate for appropriate services, if they are not currently available.
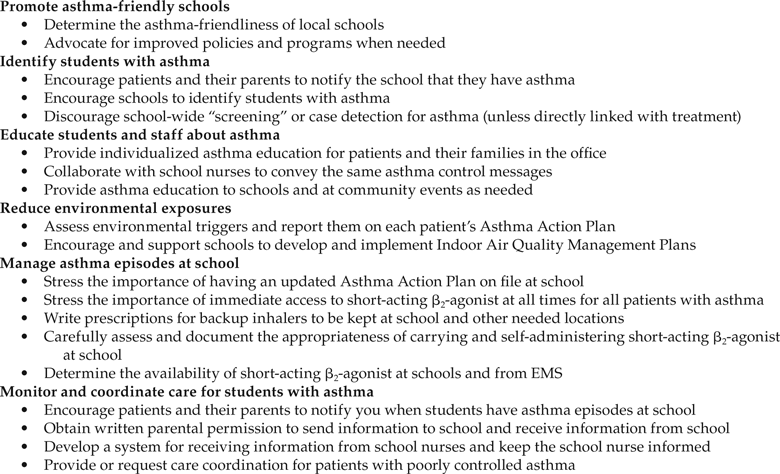
Time can be limited, and it can be difficult for asthma care clinicians to know how they can most effectively assist school-based asthma management programs. Several resources are available that highlight ways in which pediatricians and asthma care providers can support asthma education programs in schools.27,28 This article builds upon these resources and reviews recent research findings in order to provide 6 key actions pediatricians, pediatric pulmonologists, and allergists can take to enhance a full range of school-based asthma management for their patients (Fig. 1).
Promote asthma-friendly schools
Pediatricians, pediatric pulmonologists, and allergists can enhance school-based asthma management efforts and assist their school-aged patients in achieving good asthma control by supporting “asthma-friendly” schools in their communities. Schools can provide a safe and supportive learning environment for students with asthma through the adoption and implementation of policies and protocols that ensure access to appropriate quick-relief medications at school, provide asthma education for students with asthma, require asthma awareness and response training for school staff, ensure that students with asthma have an updated asthma action plan on file at school, and prohibit tobacco smoke at all times.
States, school districts, and schools have received guidance from NAEPP,29 the Centers for Disease Control and Prevention (CDC),30 the Environmental Protection Agency (EPA),31 and several national non-governmental organizations32–38 on creating these supportive environments and becoming more asthma-friendly. Success is more likely when the whole school community takes part in these actions; therefore, guidance is provided for school administrators, teachers, and staff, as well as for students, families, and parents. CDC then assesses school health policies and programs, including those related to asthma management, with the School Health Policies and Programs Study (SHPPS) that provides national in-depth assessment of key school health program components and health topics at the state, district, and school levels. SHPPS 2006 examined many school health policies and programs that support students with asthma39 and NAEPP clarified the most important considerations in the 2008 update of “How Asthma-Friendly Is Your School?,” a document that includes a series of 8 recommendations, presented in the form of questions, that can be used to determine how well a school serves students with asthma (Fig. 2).40 A secondary analysis of SHPPS 2006 data examined the degree to which elementary, middle, and high schools in the United States have policies and programs consistent with the recommendations found in “‘How Asthma-Friendly Is Your School?”26 Adherence to some of the elements was high. For example, 80% or more of schools reported allowing students to carry and self-administer asthma medications. For other recommendations, however, far fewer schools had the recommended policies or programs in place; most notably, less than one-third of schools had a full-time registered nurse (RN). Even the best policies are not always well-implemented. For example, even when schools appropriately permit students to carry a short-acting β2-agonist inhaler, as few as 14% of students with persistent asthma may actually have one at school.11,41
CDC has developed tools to assist schools in their efforts to meet NAEPP recommendations and to become asthma-friendly.42 These tools encourage schools and school districts to conduct systematic, ongoing assessments to evaluate their asthma program strategies and policies and to use this information to improve programs.43 A key component of ongoing assessment is identifying the strength of community collaborations, including partnerships with clinicians, families, and others. To assist in sustainability efforts and further strengthen community collaborations, states and communities are encouraged to highlight schools with these partnerships by providing asthma-friendly school awards to schools that meet all of the recommendations outlined by NAEPP.44–50
Clinicians can play an important role in supporting districts’ and schools’ efforts to become more asthma-friendly by advocating for improved policies and programs when they are needed, including ensuring access to quick-relief medications, having asthma action plans at school, and helping educate teachers and staff about asthma.
Identify students with asthma
Identification of young people with asthma is an important component of school-based asthma management. Key actions clinicians can take include encouraging their patients and caregivers to notify schools that the child has asthma and supporting appropriate and feasible school-based efforts to identify students with asthma. Many school-based efforts have focused on identification of students with “asthma-like” symptoms. Such programs are often referred to as “school-based screening” programs; however, the more appropriate term is case detection. Screening refers to identifying people with disease who are in a preclinical (asymptomatic) state. Screening for asthma is not possible since there is no method of diagnosing the condition in people who do not have symptoms.51 Case detection is the appropriate terminology for most school-based programs, since these programs are attempting to use symptoms and lung function abnormalities to identify young people who are experiencing symptoms but have not received a diagnosis of asthma. Schools can conduct case identification that seeks to identify students who have a previous diagnosis of asthma through the use of existing resources such as health information forms and parent or child reports to school health staff.
School-based case detection (eg, “school-based screening”) has been shown to be feasible and acceptable to students, parents, and schools, but does have limitations. Most strategies have used question-based surveys with or without lung function testing. Although surveys are easy to administer, they are limited by the potential for high false positive rates. Adding lung function testing to these types of surveys may reduce false positive rates, but lung function testing can be difficult and costly to implement. Both of these methods, that is, surveys with and without lung function testing, have been used successfully to identify new cases of asthma as well as cases of previously diagnosed but not well-controlled asthma. However, case detection is only one step in the process needed to improve asthma outcomes. Numerous opportunities exist for lapses in care that prevent attainment of improved asthma outcomes following successful case detection. Research indicates that many young people identified by school-based case detection are never evaluated by a clinician.52 Many who are evaluated are not prescribed controller medications. Lastly, many who are prescribed controller medications are not adherent to the regiment. Previous studies have shown that school-based case detection can identify students with asthma who need further care, but no prior study has collected long-term outcomes to determine whether case detection remains effective in reducing asthma symptoms in the face of these other barriers. For this reason, a recent American Thoracic Society workgroup recommended against population-based case detection until better evidence of its long-term effectiveness and/or cost-effectiveness is available.53
In the absence of a clinical trial, a recent study evaluated the cost-effectiveness of school-based case detection in a simulated population of low-income, urban, elementary-age children using surveys alone or in combination with lung function testing.54 No methodology was found to be cost-effective. The most efficient strategy used a survey to identify only children with previously diagnosed but not well-controlled asthma. Identifying new cases was not cost-effective because the predicted value of case detection was relatively low and the morbidity of asthma experienced by new cases was relatively low compared with children with previously diagnosed asthma. This last finding was corroborated by a large school-based case-detection study that showed that new asthma cases experienced fewer symptoms and much less health care use than students with previously diagnosed asthma.11
Stronger linkages between case detection, treatment, and long-term adherence could, however, yield future cost-effective approaches.54 One existing program that incorporates some of these key elements is the Breathmobile program that ties case detection and identification with treatment through the use of a mobile asthma clinic that partners with schools. Jones et al.55 reported that most students with persistent asthma in the Breathmobile program were able to achieve control within 3–6 visits. However, maintaining control was more difficult, for only 39% of patients exhibited control at >90% of subsequent visits. While this program strengthens linkages between identification and treatment, it also requires significant resources. For many school systems or communities, the high capital costs of the Breathmobile may limit its appeal. Because the cost-effectiveness of this program has not been systematically evaluated, it is difficult to know whether the trade-off between stronger linkages and higher costs is worth the investment.
Key actions for asthma care clinicians.
Until stronger linkages exist between case detection and treatment, clinicians should discourage school-wide “screening” for new cases of asthma. However, it remains important for schools to identify young people who are diagnosed with asthma. SHPPS 2006 found that 81.9% of schools are identifying students with chronic conditions such as asthma or diabetes.49 School nurses typically review health and emergency forms for a parental report of asthma along with medication order forms for short-acting β2-agonist orders. However, some young people with asthma and their parents may know that they have asthma, but many do not report the diagnosis to school staff. Furthermore, using short-acting β2-agonist orders to identify students can be problematic because research indicates that in some populations very few students with asthma have these orders at school.11 School nurses may also identify students by noting those who go to the health room with wheezing, coughing, or shortness of breath and report having asthma. These case identification systems identify students with more severe asthma and those with poorer control.
Pediatricians, pediatric pulmonologists, and allergists can support these efforts to identify students with asthma by encouraging patients and their parents to notify the school that they have asthma, and supporting appropriate school-based case identification activities.
Educate students and school staff about asthma
Asthma self-management education is also a critical component of effective care for children with asthma. Clinicians can support school and district efforts by providing asthma education to patients and their caregivers in the office setting, and when feasible by offering their expertise in asthma education to school-based staff in order to ensure consistent messaging around asthma education. Children with asthma need to learn how to manage their asthma, and appropriate asthma education should include activities that help young people obtain the knowledge and develop the skills they need to ensure successful asthma management. This includes knowing what their asthma triggers are, recognizing early signs and symptoms of asthma, knowing what to do if they experience symptoms, and using asthma equipment such as peak flow meters and inhalers. School nurses can monitor peak flow and inhaler techniques in a real-life situation and provide immediate instruction when a technique needs improvement. Since most young people spend almost one-third of each day in school, schools can provide an optimal setting for supporting and reinforcing asthma self-management education that is offered in the clinician’s office. In fact, SHPPS 2006 found that 78.7% of schools provide instruction on self-management of chronic health conditions, such as asthma and diabetes.56 Health-care providers can work with schools to ensure that consistent health messages are provided to young patients and their families.
Some school asthma education programs have reported difficulty engaging children’s primary care physicians.57–59 Asthma care clinicians can support their patients’ receipt of consistent asthma education messages by communicating with patients’ school nurses and primary care physicians about the educational programs and messages being provided at the clinical care setting; and, whenever possible, by offering to assist with or guide asthma education efforts for parents, schools, and at community events.
Several community organizations, including local chapters of the American Lung Association, the Asthma and Allergy Foundation of America, and some local asthma coalitions, offer asthma education programs in some schools for students, families, and school staff. Clinicians can query the school about the programs they currently have in place and support these programs by encouraging their patients and families to participate in them, and by encouraging schools to provide space and time for these programs.60 It is important to make offers that are likely to be effective and useful to schools within their existing framework for staff and student education.61 Providing staff support to co-teach a small-group, evidence-based program like Open Airways62 is usually more effective than giving a one-shot lecture to a large number of students.
Providing school-based asthma education can improve young people’s knowledge of asthma, self-efficacy, and self-management behaviors.63 Clinician leadership and support of asthma education for students, school staff, and parents can help ensure consistent messaging and response.
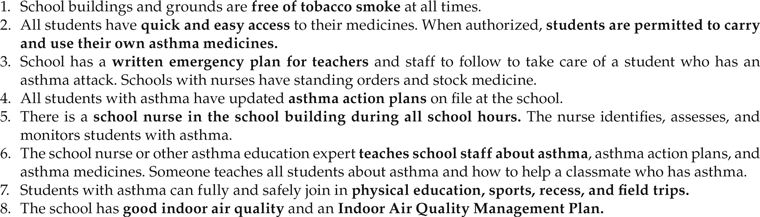
Recommendations from “How Asthma-Friendly Is Your School?” National Asthma Education and Prevention Program. http://www.nhlbi.nih.gov/health/public/lung/asthma/friendhi.htm.40
Reduce environmental exposures
NAEPP guidance stresses the need to control environmental exposures at home and at school and asthma care clinicians can provide patients and their families with the information needed to assist them in better addressing the needs of school-aged youth with asthma. Controlling environmental exposures includes actions for specific students that are based on their sensitivities and for school-wide improved indoor air quality (IAQ). In order to help address individual sensitivities, many states have developed and adopted uniform asthma action plans with check-off boxes to make it easy for clinicians to inform school personnel about the potential impact of the school environment on students’ management of their asthma.
Observational studies have shown that poor IAQ in schools is associated with illness, absenteeism, and decreased academic performance and that poor IAQ triggers asthma episodes.64–66 Children and adults who are exposed to poor IAQ can experience nausea, dizziness, headaches, sleepiness, fatigue, upper respiratory infections, and irritated eyes, nose, and throat. These symptoms can reduce student and staff productivity.67,68
A secondary analysis of SHPPS 200669 found that having a formal school IAQ management program was positively associated with having policies, using strategies, and requiring staff training to promote good IAQ. The goals of an IAQ management plan are to address, through no-cost or low-cost solutions, any existing IAQ problems; to create awareness among school staff so that staff can work to prevent IAQ problems; and to address IAQ problems as they occur (rather than waiting until the problem escalates). Priorities for IAQ management programs most often include the heating, ventilation, and air-conditioning systems; moisture and mold control; pest management; cleaning and maintenance; materials selections; and pollution source control. The US EPA has developed the Indoor Air Quality Tools for Schools Program70 and provides tools and technical assistance, including annual training on developing and implementing an IAQ management program. Numerous school districts across the country report improved IAQ and favorable student outcomes, including reduced asthma morbidity and improved school attendance after implementing the EPA’s Tools for Schools Program.71–73 District-wide programs have been developed when an “asthma champion” has taken the lead to convince a superintendent of the benefits or when “sick schools” have been identified. The active reporting and quick response to student, parental, or staff air quality concerns promoted by Tools for Schools yields high satisfaction and program expansion in many communities. The National Education Association strongly supports Tools for Schools and it educates union members about the program via print, conferences, and its online NEA Academy.74
Manage asthma episodes and attacks at school
Asthma action plans, asthma protocols (both everyday management and emergency asthma and allergy protocols), trained health staff, and access to short-acting β2-agonist are required for the management of asthma episodes at school. A written asthma action plan is the critical communication tool for effective asthma management during the child’s school-related activities.8 All school-aged children with asthma should have a written asthma action plan, developed by their asthma care clinician, on file at school. Asthma action plans need to be readily accessible during all school-related activities.8 The asthma action plan should be individualized to support full participation in school-related activities, to identify asthma triggers and help prevent environmental exposures to them, to direct the patient or school nurse to adjust medications in response to particular signs, symptoms, and/or peak flow measurements, and to state when and how to seek medical help.8,75
The asthma action plan for use at school can be the same document as the one for home use if it includes triggers in the school environment (eg, classroom pets) and the medication sequence for quick relief of asthma episodes. Many states and communities have standard asthma action plans that are appropriate for all settings. These standard plans can assist families, schools, and child care providers to find information quickly; they can also be used to increase the proportion of children with required forms at school.76 Standard forms can be downloaded from state asthma program Web sites or they can even be completed online.77–79 Asthma care clinicians can also keep a supply of standard plans at the office. Asthma educators and other office support staff can ensure that updated plans are in the medical record, given to the child and family, and sent to schools and other appropriate settings. Office support staff can also ensure that parents have signed appropriate release-of-information forms to facilitate communication to and from the school.
In order to enhance efforts, schools should ensure that a properly trained health service staff/designee is available at all times to access and administer medication according to individualized asthma action plans and standardized emergency protocols during the school day and during all school-related activities, regardless of time or location.80 Many states and school districts have developed asthma manuals, and the National Association of School Nurses provides training to school nurses to support appropriate asthma management at school. Updated standard protocols have been developed by NAEPP to assist school districts and schools when a student does not have an asthma action plan at school81 or when a school nurse is not available.82 Immediate access to short-acting β2-agonists is critical to reducing asthma morbidity and to preventing mortality.83 Short-acting β2-agonists can be carried by the student, or kept in the school health office or another location. Inhalers may be provided by the family or by the school or another community asthma partner.76
Asthma-friendly schools permit students to quickly manage asthma symptoms or episodes by permitting students to carry and self-administer quick-relief bronchodilator medication when approved by clinicians, parents, and school nurses. Clinicians can fully support the schools’ and districts’ efforts by carefully assessing and writing recommendations for students who are developmentally qualified and physically able to carry and administer medication to treat acute symptoms or to prevent exercise-induced bronchospasm.80 NAEPP has developed assessment criteria that include student, family, school, and community factors for clinicians to consider before making these recommendations.84
Although they take longer and are no more effective than inhalers with holding chambers, some schools have nebulizers and stock albuterol provided by community asthma partners.85 Students who are permitted to carry inhalers may not always have one when it is needed. In some communities, emergency medical services (EMS) may not carry albuterol. The importance of a personal backup inhaler kept in the health office is especially critical in schools that do not provide stock short-acting β2-agonist for emergencies.
Asthma care clinicians can support schools by stressing the importance of immediate access to short-acting β2-agonist at all times for all patients with asthma, and by writing prescriptions for backup inhalers and spacers to be kept at school and other necessary locations. Clinicians should carefully assess and document the appropriateness of carrying and self-administering short-acting β2-agonist at school.84 If schools do not have a stock supply of short-acting β2-agonist, clinicians can help to determine the availability of short-acting β2-agonist from EMS or assist with obtaining stock medications.86–88
Monitor and coordinate care for students with asthma
When asthma is under good control, symptoms are unusual, activity is not limited, and sleep is not interrupted by asthma. Students with asthma require monitoring to identify those without good control and the asthma care clinician is a key partner schools rely upon to assist in asthma management efforts. When students with asthma are identified at school, by school health services staff, the lack of good symptom control must be communicated to families and asthma care clinicians. Further, clinicians must be ready to respond by working with schools and districts to fully address the needs of students with asthma. Some students may need care coordination or case management services, which include a range of client-centered services that link clients with health care, psychosocial, and other services. Care coordination may be provided by a nurse, a social worker, a respiratory therapist, or an asthma educator who is employed by a medical office, a community, or public health asthma program, a health insurer, a school, or another organization. Care coordinators work closely with families, school nurses, and asthma care clinicians.
NAEPP clarifies the need for clinicians and schools to focus on asthma control and provides age-specific criteria for doing so.10 From a clinician’s perspective, for some students school-based monitoring is especially useful because school absences have been shown to be a better predictor of poor control (NAEPP criteria) than emergency department visits or hospitalizations,89 the traditional avenues for determining patient adherence to treatment regiments. SHPPS 2006 found that 78.7% of schools provide tracking of students with chronic health conditions.56 The extent of tracking is, however, unknown. Ideally, school-based tracking includes monitoring absences from school, calculating the percentage of absenteeism, tracking visits to the school health office due to asthma, reporting and tracking asthma symptoms, noting non-participation in physical education class due to asthma, and tracking early dismissals or 911 calls from school due to asthma.43
Information gained from such monitoring and tracking is important for families, schools, and clinicians. School nurses can use these data to identify which students have poorly controlled asthma so that more intensive interventions can be targeted to these students; they can also use the information to support efforts to evaluate the effectiveness of a school-based program.90 Schools can also assist families and clinicians by informing them when indicators of poor asthma control are identified at school. Parents can give written permission for schools to send standard “Dear Doctor” letters that report such events as health room visits or absenteeism.25,91
For most students with asthma, successful monitoring and tracking can be accomplished by having 5 things at school:
1. a written Asthma Action Plan
2. short-acting β2-agonist medication (backup inhaler if student carries med)∗
3. order/information exchange forms∗∗
4. a peak flow meter∗
5. a holding chamber/spacer∗
Schools with effective programs and full-time school nurses can also assist clinicians by actively assessing asthma control through student self-report questionnaires (eg, Asthma Control Test92) and through reassessing students every 3–6 months. Peak flow monitoring is considered by school-based asthma experts to be especially useful at school.93 Although symptom monitoring has been shown to be equally effective for individuals that are good perceivers of airway obstruction, school nurses and other staff may not know which students are poor perceivers. Peak flow measurements also assist with decisions about sending students back to class. Schools can also monitor inhaler skills with In-Check Dials® and peak expiratory flow meters for children with moderate or severe persistent asthma who have a history of severe exacerbations, and schools can report low readings to families and clinicians. In-check Dials® are handheld inspiratory flow measurement devices designed to accurately simulate the resistance of popular inhaler devices such as MDIs, DPIs, Turbuhaler®, and Diskus®. In-check Dials® can be used to train patients to use more or less inspiratory force to achieve their optimal flow rate and thereby the best deposition of medication into the lungs.94–96
All of the methods described are useful in monitoring a student’s level of asthma control. Clinicians can work with school districts to develop or revise communication systems that are conducive to sharing this and related information between the school and asthma care clinicians and also to develop forms that can improve efficiency. Many clinicians find that fax reports, with strict precautions for confidentiality, from the school nurse to the office nurse or asthma educator work well.85
When it is determined that a student does not have good asthma control, clinicians and school health services staff should work together to adequately coordinate their care. Coordination and follow-up of medical treatments are components of medical case management. Care coordination services ensure timely, coordinated access to medically appropriate levels of health and support services and continuity of care through ongoing assessment of clients’ and key family members’ needs and personal support systems. Medical case management includes treatment adherence counseling to ensure readiness for and adherence to complex asthma regimens. Critical activities for adequate care coordination include: (1) initial assessment of service needs; (2) development of a comprehensive, individualized service plan; (3) coordination of services required to implement the plan; (4) client monitoring to assess the efficacy of the plan; and (5) periodic reevaluation and adaptation of the plan as necessary over the life of the client. It includes all types of case management, including face-to-face meetings, phone contact, and any other forms of communication.97 Students with asthma need periodic follow-up visits with their asthma care clinician, and schools can facilitate these appointments.10 Usually, extensive care coordination services are needed only by students whose asthma is not under good control with the usual support systems.
Care coordination uses a chronic-care model that includes the 8 common characteristics of effective educational and behavioral asthma interventions98 and can be provided by health plan chronic disease managers, asthma educators, nurses,25,99–104 social workers,105 and others.106–109 Schools with school-based, or school-linked health centers (SBHC) offer additional services; and SBHC users are more likely to receive multiple components of good asthma care.110 Markers of asthma morbidity in pediatric patients, including frequent school absences, poor adherence to medication regiments, and inadequate or inappropriate medical care utilization, are often multifactorial, with numerous physical and psychosocial aspects. These factors, in addition to parental beliefs about chronic illnesses and medications, can be addressed by care coordinators.111,112 Asthma care clinicians should identify a source for care coordination when asthma control is not achieved with guideline-based medical care and basic asthma education services. Some communities may be able to use asthma registries or other shared electronic medical records to promote communication and coordination.
Care coordination may also be needed by students having difficulty adhering to prescribed medications. Long-term controller medications, primarily inhaled corticosteroids, are the cornerstone of preventing exacerbation among children with persistent asthma.75 When poor adherence is suspected by a clinician, school-based supervised therapy for inhaled steroids has been shown to be a good option for children whose asthma is not well controlled.11,12,14 This may be especially important for inner-city populations where ICS are especially underused, with median usage rates of only 32% among blacks, compared with 51% for white populations.113
Clinicians should be full participants in care coordination efforts for students with asthma. Asthma care clinicians need to ensure that updated asthma action plans and medication order forms are sent to schools. Further, clinicians can train office staff to obtain parental signatures on release-of-information forms at regularly scheduled follow-up visits; and keep a supply of appropriate school forms in the office. With parental permission, clinicians can request that schools notify them when a student’s asthma may not be under good control (eg, frequent quick-relief bronchodilator use).
Conclusion
Asthma morbidity in pediatric patients can be significantly reduced through the coordinated efforts of asthma care clinicians, families, and schools. The inability to fully participate in physical activity; fatigue and poor academic performance due to nighttime awakenings; frequent early dismissal from school; excessive school absenteeism; and frequent visits to the school health office and also to a physician’s office affect the quality of life of the pediatric patient and his family. The efforts of asthma care clinicians and schools, both individually and collectively, should address the medical and psychosocial needs of the patient. The synergy created by each playing an active role in pediatric asthma management assists the patient in gaining adequate asthma control.
In addition to writing asthma action plans for their patients, clinicians can focus their efforts on the following key actions: promote asthma-friendly schools; identify school-aged children with asthma; educate patients and school staff about asthma; assist patients, families, and schools in reducing exposure to environmental triggers; assist school staff in helping students manage their asthma at school; and play an active role in monitoring and coordinating care with schools and families (Fig. 1). Although it takes some initial time investment, school-based asthma management programs can assist families and asthma care clinicians in achieving good asthma control for school-aged patients.
Author Disclosure Statement
The findings and conclusions on this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the U.S. Environmental Protection Agency.
Key Resources
• Expert Panel Report 3: Guidelines for the diagnosis and management of asthma www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
• Printable Plan: www.nhlbi.nih.gov/health/public/lung/asthma/asthma_actplan.pdf
• Nursing protocol for students without asthma action plans: www.nhlbi.nih.gov/health/prof/lung/asthma/sch-emer-actplan.pdf
• Steps to follow for an asthma episode when a nurse is not available: www.nhlbi.nih.gov/health/prof/lung/asthma/no-nurse.pdf
Strategies for Addressing Asthma within a Coordinated School Health Program:
www.cdc.gov/HealthyYouth/asthma/strategies.htm
Indoor Air Quality Tools for Schools Program:
www.epa.gov/iaq/schools/
State asthma programs and/or state asthma coalitions:
• Community Action to Fight Asthma: www.calasthma.org/home/
• Minnesota Department of Health: www.health.state.mn.us/divs/hpcd/cdee/asthma/ActionPlan.html
• New York State Department of Health: www.health.state.ny.us/diseases/asthma/pdf/4850.pdf
Asthma-Friendly Schools Initiative: www.lungusa.org/lung-disease/asthma/in-schools/asthma-friendly-schools/about-afsi/
Open Airways for Schools: www.lungusa.org/lung-disease/asthma/in-schools/open-airways/open-airways-for-schools-1.html
Footnotes
∗If schools do not provide a stock supply of short-acting β2-agonist and holding chamber and peak flow meter for multi-student use, then each student needs one at school.
∗∗Can be included in the written asthma action plan.