
Abstract
Observations of short-term changes in the neural health of youth athletes participating in collision sports (e.g., football and soccer) have highlighted a need to explore potential structural alterations in brain tissue volumes for these persons. Studies have shown biochemical, vascular, functional connectivity, and white matter diffusivity changes in the brain physiology of these athletes that are strongly correlated with repetitive head acceleration exposure. Here, research is presented that highlights regional anatomical volumetric measures that change longitudinally with accrued subconcussive trauma. A novel pipeline is introduced that provides simplified data analysis on standard-space template to quantify group-level longitudinal volumetric changes within these populations. For both sports, results highlight incremental relative regional volumetric changes in the subcortical cerebrospinal fluid that are strongly correlated with head exposure events greater than a 50-G threshold at the short-term post-season assessment. Moreover, longitudinal regional gray matter volumes are observed to decrease with time, only returning to baseline/pre-participation levels after sufficient (5–6 months) rest from collision-based exposure. These temporal structural volumetric alterations are significantly different from normal aging observed in sex- and age-matched controls participating in non-collision sports. Future work involves modeling repetitive head exposure thresholds with multi-modal image analysis and understanding the underlying physiological reason. A possible pathophysiological pathway is presented, highlighting the probable metabolic regulatory mechanisms. Continual participation in collision-based activities may represent a risk wherein recovery cannot occur. Even when present, the degree of the eventual recovery remains to be explored, but has strong implications for the well-being of collision-sport participants.
Introduction
Traumatic brain injury (TBI) records 1.6 million to 3.8 million cases annually. 1 Of these numbers, mild TBI (mTBI) represents ∼80–90% of cases. 2 Long-term risks involved with mTBI are neurological disorders, such as mild cognitive impairment and Alzheimer's disease 3 ; psychiatric disorders, such as depression and post-traumatic stress disorder 4 ; and, in certain cases, may include chronic traumatic encephalopathy (CTE).5–7
Sports-related mTBI is documented in athletes playing collision sports, such as football and soccer. 8 It should be noted that 50–90% of sports-related mTBIs go undiagnosed,9,10 which raises serious concerns for athlete well-being. Football and soccer account for most high school sports-related mTBI.11,12 Concerns for the neural health of youth athletes are further highlighted by the observation of changes in neurological behavior without clinically observed impairment. 8 These changes can be explained by asymptomatic (“subconcussive”) head acceleration events (HAEs) that cause silent cognitive deficits or other neurophysiological impairment. 13
Structural health monitoring with multi-modal assessment of effects from repetitive HAEs12,14 points to mechanical stress as a likely cause of asymptomatic injury. Neurological changes have been evidenced biochemically, 15 through modulation of vascular autoregulatory capacity, 16 by alternations in visual working memory,17,18 by changes in functional network connectivity,19–21 and altered measures of white matter diffusivity.22–26 All these measures have been found to be linked to kinematic correlates obtained from on-field telemetry.13,14,27
Given the prevalence of neurophysiological changes with exposure to repetitive HAEs, it is reasonable to assess whether these alterations are associated with longitudinal structural volumetric changes. Existing methods to make such a determination include automated voxel-based morphometry (VBM), using tools such as FSL-SIENA, 28 FSL-VBM,29–32 model-based FSL-FIRST, 33 FreeSurfer-MorphometryStats, 34 and technician-based, manually segmented regional volumetry techniques35,36 (ITK-SNAP v3.837).
Here, a region-based volumetric analysis was conducted on a data set of high-school collision sport athletes (CSAs) known to have experienced repetitive HAEs. Past work has revealed longitudinal region-specific volumetric changes in both gray matter (GM)38,39 thickness, ventricular cerebrospinal fluid (CSF) increase,40–42 and white matter (WM) volumetry 43 in subjects with mTBI. Volumetric measures were evaluated in collision-sport athletes (male football, female soccer) and non-collision-sport peers, including whole-brain WM, 44 ventricular CSF (dCSF), 45 and GM 46 parcellations. Observation of longitudinal changes in regional tissue volumes that are linked to exposure to repetitive HAEs should provide insight as to how accumulation of mechanical strain may produce a metabolic cascade that has potential for longer-term neural health.
Methods
Participants
Eighty-six high-school–aged athletes participated on a voluntary basis, comprising two pools: 57 athletes participating in CSA and 29 athletes participating in non-collision sports (NCA; e.g., track and field, gymnastics, and cross-country). Participants were not excluded from either pool if they had a history of concussion. Participant demographics are provided in Table 1.
Demographics of Participants with a Complete Set of Valid Imaging Data as Collected at Pre/Test Session
All values are: mean ± StdDev, [Min, Max]).
CSA, collision sport athletes; NCA, non-collision sport athletes.
Collision sport athletes
Thirty-eight male (ages, 15–18 years) and 19 female (ages, 14–18 years) athletes, each participating in collision-based sports (M, American football; F, soccer), were recruited from three local high schools over four seasons of play.
Non-collision sports
Fifteen male (ages, 15–18 years) and 14 female (ages, 14–18 years) athletes, each participating only in non-collision sports, were recruited from the same high schools as the CSA participants. This pool served as a control for reproducibility of measurements over time. The Purdue Institutional Review Board approved the study procedures, and participants provided written informed consent before completion of the protocol.
Participant schedule
Imaging sessions and median intervals between sessions are schematized in Figure 1 for both CSA and NCA.

Schedule of longitudinal assessments for participants. Median intervals to each category of assessment are shown for each participant subgroup. (Top) Collision sport athletes (CSA) involved in boys' American football (N = 38) and girls' soccer (N = 19) were imaged at least five times around their competition season (Pre, during off-season conditioning; In1, during first half of the competition season [1–10 weeks after onset]; In2, during second half of the competition season [5–15 weeks after onset]; Post1, 1–2 months after end of the competition season [14–25 weeks after onset]; Post2, 4–6 months after end of the competition season [24–38 weeks after onset]; Post3, a subset of non-senior participants were imaged again 7–9 months after end of the competition season [44–52 weeks after onset]). (Bottom) Non-collision sport athletes (NCA; N = 29, F/M = 14/15) involved in non-collision sports (see Table 1) were imaged twice during competition and conditioning (Test and Retest separated by 1–2 months).
All CSAs underwent at least five magnetic resonance imaging (MRI) sessions around their competition season: Pre, before collision activity onset (i.e., before season-related activity commenced); In1, during the first half of the competition season; In2, during the second half of the competition season; Post1, near-term follow-up session after (1–10 weeks) competition season conclusion; and Post2, long-term follow-up session after (11–23 weeks) competition season conclusion.
For a subset of 21 CSA athletes, a sixth MRI session was conducted: Post3, prolonged follow-up session after (29–37 weeks) competition season conclusion. This imaging session was acquired as the Pre assessment for the subsequent season for persons who were not seniors at the time of Pre, In1, In2, Post1, and Post2. This session was only incorporated in analyses intended to examine the nature of volumetric changes after a prolonged period free of participation-related collision activity. Note that all CSAs were physically active, but not engaged in collision-related activities, before Pre/Post3, because they were all taking part in conditioning activities for their sports.
All NCAs underwent two MRI sessions, Test and Retest, separated in time by 4–13 weeks. All imaging sessions were conducted during training and competition activities to maintain comparable levels of physical activity around each session.
Magnetic resonance imaging data acquisition
All imaging was conducted at the Purdue University MRI Facility (West Lafayette, IN), using a 3T General Electric Signa HDx (Waukesha, WI) with a 16-channel brain array (Nova Medical, Wilmington, MA). To assess the longitudinal stability of anatomical volumes, a high-resolution T1 acquisition (three-dimensional fast spoiled gradient-recalled echo; 1-mm isotropic resolution; repetition time/echo time = 5.71/1.976 msec; flip angle = 73 degrees) was conducted at each session.
Head acceleration events data collection
CSAs were monitored for HAEs in each official practice and game. Telemetry data documenting peak translational acceleration (PTA) for each HAE were collected using one of two systems: the Head Impact Telemetry System (HITS; Simbex, Lebanon, NH), used only for American football athletes, or the xPatch (X2 Biosystems, Seattle, WA), used for both American football and soccer athletes. HITS encoders were used only with Riddell helmets, being placed before the season and examined thereafter only to recharge batteries or replace encoders that had ceased nominal operation. When the xPatch was used, the device was placed on the athlete's right ear using an adhesive patch before each practice or game and collected subsequent to the activity. Regardless of the system being used, a researcher was present at every session (practice or game) to ensure proper function of sensors, as previously described.8,47
Two CSAs were excluded from analysis because of incomplete HAE data: One football athlete ceased participation in the sport during the season; a second football athlete had his HITS encoder fail, and no replacement was available for several weeks.
Magnetic resonance imaging data pre-processing
The top row of Figure 2 depicts the pre-processing pipeline conducted on each anatomical (T1-weighted [T1w] MRI) scan (i.e., for every athlete, at each session) to produce its representation in standard space, whereas the bottom row illustrates the segmentation and tissue mask generation of the standard space template, which is finally used to compute a volumetric measure for a segmented standard-space region of interest (ROI).
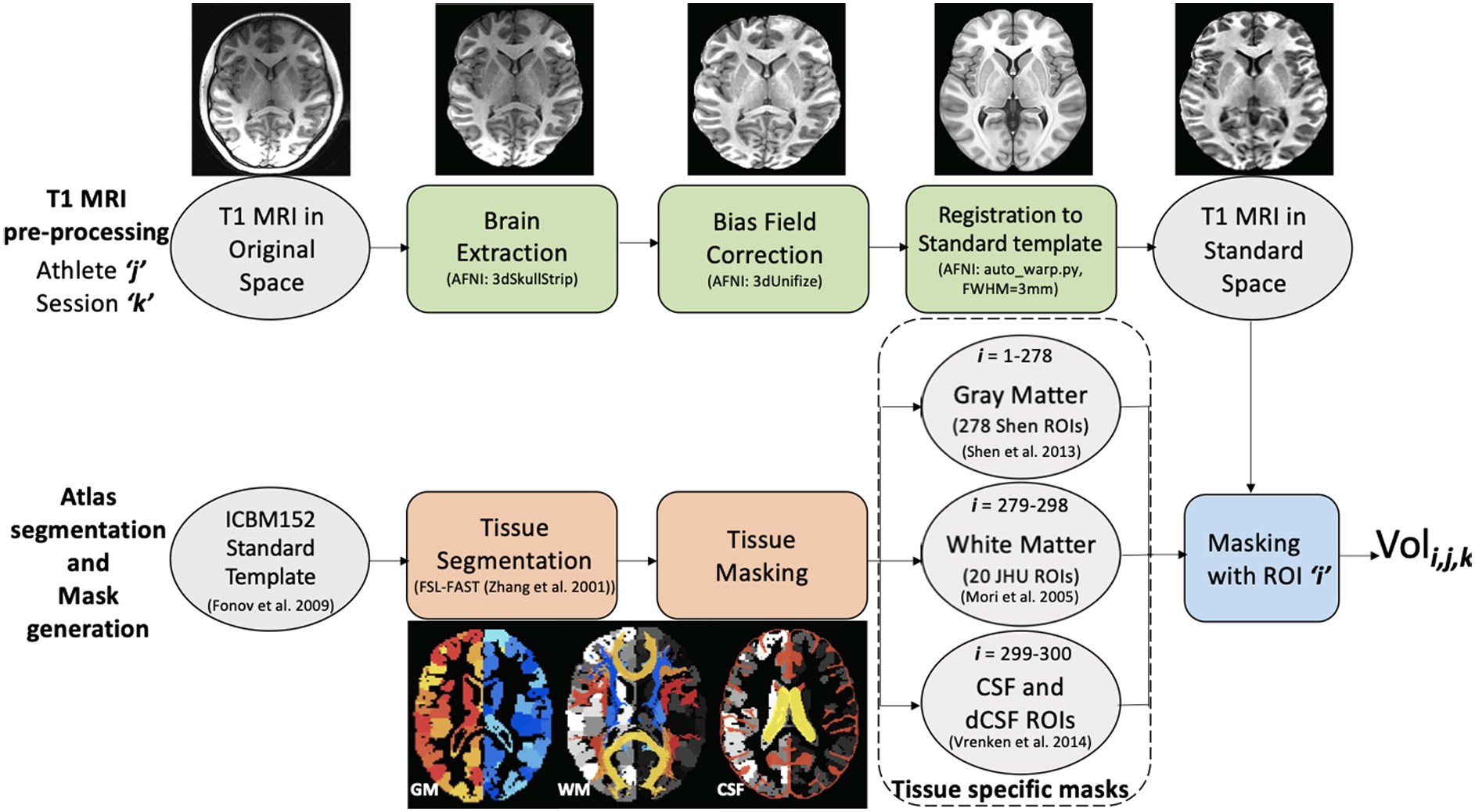
Pipelines for pre-processing, generation, and application of tissue-specific masks to T1w images for calculation of volumetric changes as a function of time. (Top) For each athlete (
Relative volume change computation
Relative volume changes were computed at three levels for each unique athlete session. First, the relative regional volume change (rRVC) was computed on an individual ROI basis, for each ROI associated with a given tissue type. Second, the relative tissue volume change (rTVC) was computed for each tissue type (GM, WM, CSF, and dCSF) by aggregating the relative volume changes in comprising ROIs. Third, relative brain volume change (rBVC) was computed by aggregating over relative tissue volume changes (GM, WM, and CSF) for the given athlete session.
To examine volumetric changes on a normalized region-specific basis, a novel pipeline was implemented. First, the rRVC in the ith ROI was computed for the jth athlete at the kth follow-up session (CSA, In1, In2, Post1, Post2, and Post3; NCA, Retest) with normalization to baseline (CSA, Pre; NCA, Test) volume as:
The brain-wide measure of rTVC for a given athlete session was computed at each session by a weighted sum of the rRVCs obtained for each of the NX ROIs comprising tissue X
The weight
The rBVC was similarly computed as the weighted sum of rTVC over the GM, WM, and CSF tissue masks, where wGM = 0.4262, wWM = 0.3912, and wCSF = 0.1826 represent the relative fraction of the entire brain encompassed by the GM, WM, and CSF masks, respectively, for the MNI-152 nonlinear sixth-generation atlas (ICBM152). 48
Head acceleration event processing
HAE data were pooled over the HITS and xPatch sensors and subsequently pruned by following the windowing and thresholding (≥20 G) procedure of McCuen and colleagues. 47 Note that whereas both devices have been documented to exhibit low average error over large sample sizes,50,51 both devices are also known to exhibit appreciable error levels on an individual measurement basis. 50 No analyses were performed on the basis of singular events.
The count of HAEs exceeding a PTA threshold (PTATh∈{20G, 25G, 30G…95G}) for the jth athlete at the kth (k ∈ {In1, In2, Post1}) follow-up session was computed as:
where Mk represents the total number of HAEs experienced before the kth session, and
Statistical analysis
Analyses were performed in MATLAB (R2020a; The Mathworks, Inc., Natick, MA), using the statistical approaches described in Glantz and colleagues. 52 Independence of test classes is implied when comparing rTVC from different populations (CSA, NCA) and separate sessions, but not for separate tissues, given that they are partitions of the complete brain.
Before conducting analyses across populations, the rTVC values for NCA athletes at Retest were checked for any sex effects using an unpaired two-sample t-test. Thereafter, CSA athlete measures of rTVC were evaluated for sphericity (Mauchly's W) and normality (one-sample Kolmogorov-Smirnov) before a one-way repeated-measures analysis of variance (rANOVA) was used to determine whether longitudinal differences in rTVC for CSA athletes were associated with session. Post hoc t-tests were conducted on a pair-wise basis within the CSA population to identify session-specific changes (paired t-test) and across the CSA and NCA to detect any population differences (unpaired t-test).
Assessment of the correlation of volumetric changes (rTVC) with HAE exposure (across multiple PTA thresholds) was effected by computation of Pearson's r at each session. A linear predictor was subsequently modeled for rTVC as a function of number of HAEs (nHAE) at each session, only for those PTATh for which a significant r was observed. All statistical results from these assessments were corrected for multiple comparisons using the Bonferroni correction.
Localization of region-specific longitudinal changes in rRVC was effected for CSAs on a confidence interval (CI) basis, using the NCA population as a reference. In this case, each ROI in the CSA was assessed on a tissue-level basis to determine whether the average rRVC for the given tissue exhibited a mean change that fell outside the 95% CI for the specific tissue (i.e., rTVC) for the NCA. Thus, two ROI maps were generated for each tissue in CSA, identifying those ROIs for which the average CSA rRVC changes were 1) more negative than the lower 95% CI bound of the rTVC for NCA or 2) more positive than the upper 95% CI bound of the rTVC for NCA. Note that the WM assessment did not reveal any within-season ROIs falling outside the 95% CI and was omitted from further analysis.
Results
Measurements of rTVC were found to be reliable in the control (NCA) population. rTVC values were found to be spherical and normal and were pooled across sex because the Test-Retest evaluation of NCA (rTVCRetest) was not found to differ significantly. Additionally, it is to be noted that rTVCRetest values were not different in mean from zero over the 4- to 13-week time scale.
Mean scores of rTVC for GM and dCSF exhibited significant session-wise differences within CSA and between CSA and NCA. Longitudinal assessment (rANOVA) of rTVC for the CSA population was found to be significant for GM (F(3,168) = 2.91) and dCSF (F(3,168) = 3.13). Post hoc Bonferroni corrected t-tests of rTVC within the CSA population and across the NCA-CSA populations are presented in Table 2.
Comparisons, by Tissue Type, of rTVC as a Function of Group and Session
Values in bold are statistically significant at p < 0.05 after Bonferroni correction.
For each tissue of gray matter (GM), cerebrospinal fluid (CSF), and deep (ventricular) CSF (dCSF), results are presented for both within-group analysis of the collision sport athletes (CSA) and for an across-group analysis of CSA with the non-collision sport athletes (NCA). To evaluate within-group differences for CSA, Bonferroni-corrected paired t-tests were conducted to compare the mean difference in relative tissue volumetric changes (rTVC) on a pair-wise basis between follow-up sessions (In1, In2, Post1, and Post2). To evaluate CSA relative to NCA, Bonferroni-corrected unpaired t-tests were conducted to compare the mean difference in rTVC on a pair-wise basis between the CSA follow-up session and NCA follow-up session (Retest).
Assessments of rTVC for dCSF demonstrated a linear relationship with accumulated repetitive head injury trauma (nHAE) at a PTATh of 50 G. The predictor modeling of rTVC as a function of nHAE for the significant PTATh session is illustrated in Figure 3 with respective 95% CIs.
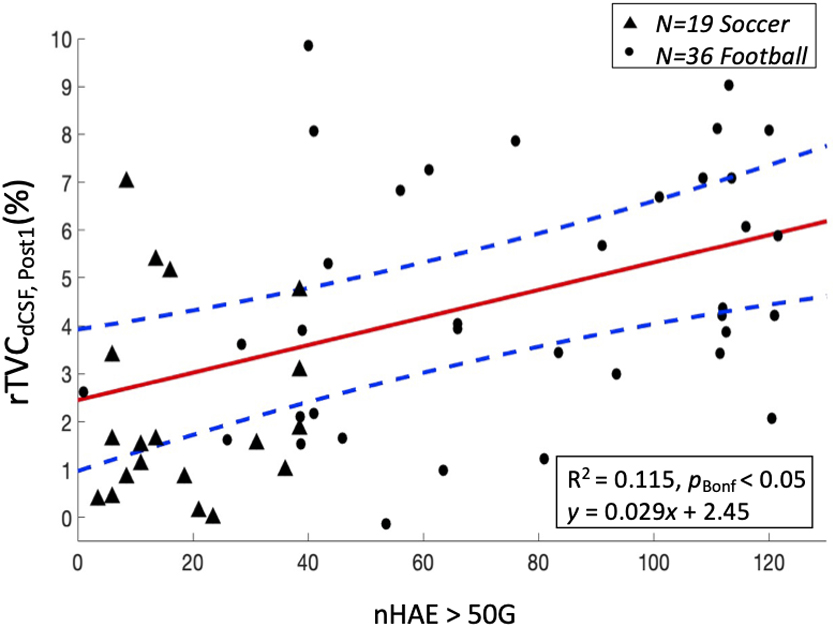
Linear dependence (pBonf < 0.05) at Post1 (N = 55) for percentage relative tissue volume change (rTVC) of ventricular cerebrospinal fluid (dCSF) as a function of the number of head acceleration events (nHAE) exceeding 50 G. Female soccer athletes (N = 19) and male football athletes (N = 36) are represented by solid triangles and solid circles, respectively. Red solid and blue dashed lines represent the mean regression line and corresponding 95% confidence interval. Note: Two football athletes with incomplete HAE data were excluded from this analysis.
Longitudinal volumetric measures of GM ROIs for CSA exhibited a concave up behavior. Values decreased from baseline (Pre) with maximum deviation at end of season, given that collision-based activity ceased (Post1), followed by a neuroplastic return to baseline (Pre) after an extended period of rest (Post3).
Figure 4A illustrates GM ROIs of GM for CSA exhibiting an average rRVC exceeding the upper 95% CI defined by rTVC of GM for NCA. The number of positively deviant ROIs peaked at In1, decreased with time until Post1, and then again increased across Post2 and Post3.
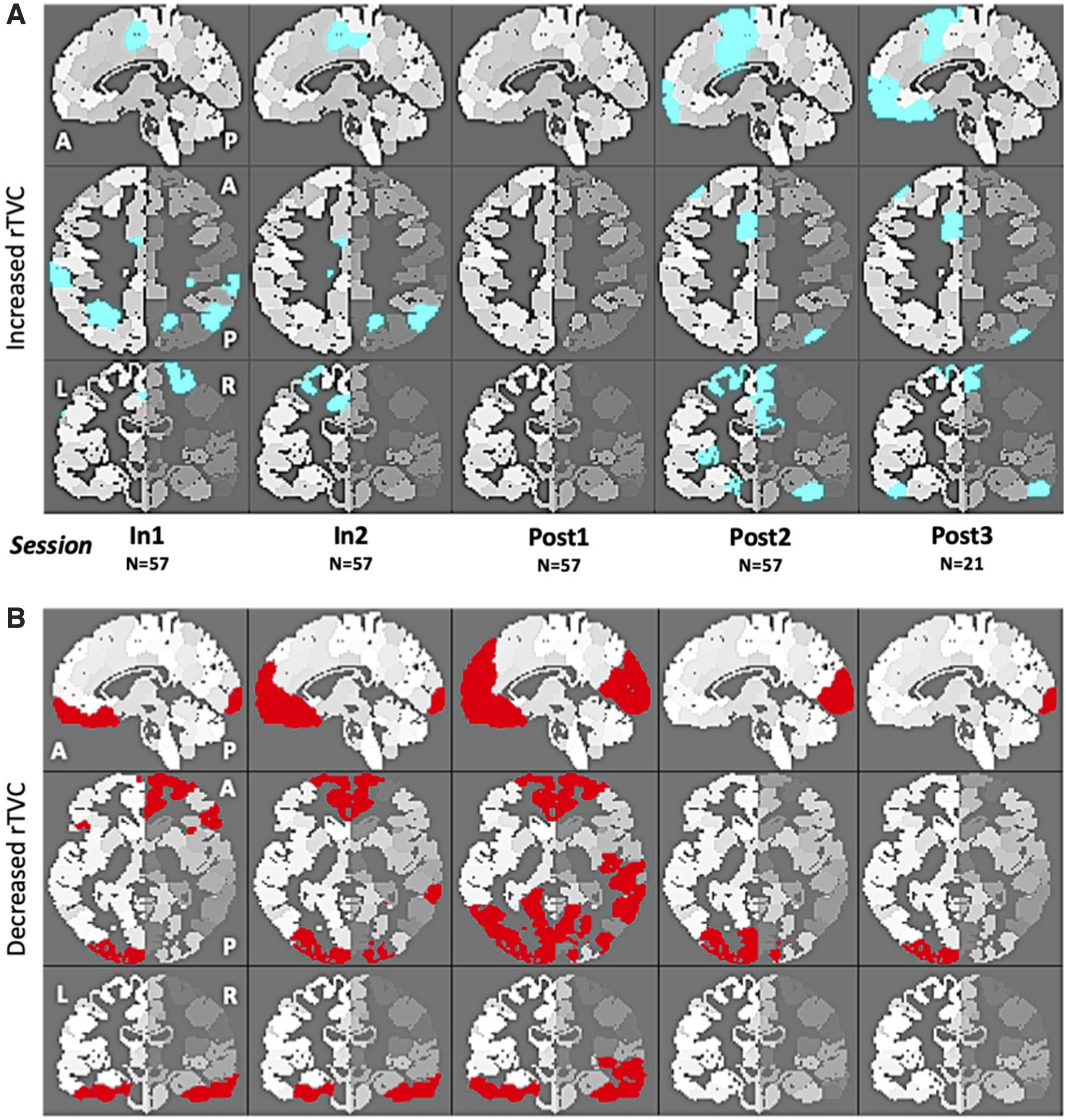
Gray matter regions of interest (ROIs)
46
in collision sport athletes (CSA) at each given imaging session (see Fig. 1) who exhibited an average relative regional volume change (rRVC), relative to Pre, that fell outside the 95% confidence interval (CI) defined from Test-Retest evaluation of non-collision athletes (NCA; N = 29). (
Figure 4B illustrates GM ROIs for CSAs exhibiting an average rRVC falling below the lower 95% CI defined by rTVC of GM for NCAs. The number of negatively deviant ROIs increased longitudinally across sessions In1-Post1, but fell sharply for Post2 and Post3.
Discussion
This investigation characterized and explained variations in brain volume measures from repetitive mTBI experienced by the participation of high-school–aged youth in collision sports (CSA). Using MRI, volumetric changes were assessed across a season of collision-sport participation and compared with the session-to-session variability of age-matched peers who participate only in sports that do not involve purposeful collisions (NCA). Statistically significant rTVCs were observed for GM and dCSF in CSA at the post-season (Post1) measure, relative to measures obtained before the season's onset of collision exposure (Pre). Further, longitudinal volumetric dCSF increases in these athletes were found to be significantly correlated with exposure to repetitive mTBI (i.e., nHAE). Consistent with previous observations of changes in brain health in this population, the changes observed in dCSF did not return to baseline/normative levels until several months after the cessation of collision-based activities (Post2, Post3). Although persistent alterations such as those suggesting accrual of changes year over year were not observed, concern remains for the neural health of CSAs given the relatively long duration of the observed alterations in brain volume.
Documented volumetric changes for CSAs are suggestive of at least transient deleterious alterations to brain physiology brought about by repetitive HAEs. Decreases in GM volume and increases in dCSF volume are not consistent with previous literature quantifying year-to-year normative brain development.53–55 Further, volumetric changes in dCSF were linked to cumulative exposure to repetitive mTBI. Given the intersession intervals, and the subsequent neuroplastic return to baseline after extended rest from collision-based activity, it is unlikely that these observed changes are a consequence of maturation in adolescents. Note that we are here assuming that normative changes for youth athletes over the interval between imaging sessions are captured by our test-retest measures with the NCAs. The observation of significant tissue-level (GM, CSF, and dCSF) population-specific volumetric changes for CSA at Post1 (Table 2) can be reasonably attributed to accumulated physiological changes caused by HAEs, which are expected to be absent (or at least substantially lesser) in NCA.
Near-term post-season measurements of volumetric changes in dCSF for asymptomatic CSAs were predicted by cumulative exposure to repetitive mTBI. The longitudinal tissue-level changes observed in mean rTVC for dCSF were strongly correlated at Post1 with nHAE at a PTA threshold of 50 G (Fig. 3). Regional brain mechanical responses to randomly incident HAE exhibit a primary intersection of induced strain near the center of the brain.56,57 This accumulated strain might explain the observation of localized dCSF increase as opposed to a significant global change in CSF. These findings are not dependent on athlete sex even after considering differences in hit distribution profiles between football and soccer athletes. 58 At this 50-G threshold, these volumetric findings complement previous detection of cerebrovascular reactivity (CVR) 16 and magnetic resonance spectroscopy (MRS) 15 changes for the asymptomatic CSA population. Further, similar PTA thresholds (e.g., 60 G) have been found to induce functional changes in previous biomarker studies involving this CSA population using MRS 59 and working memory functional MRI (fMRI).8,17 These various findings combine to further our understanding of the threshold at which HAEs meaningfully affect brain health.
In contrast, regional variation of GM volumetric measures was sparsely scattered across all areas of the brain. Longitudinal measurements of volumetric changes in GM for CSA primarily showed an increase in parietal cortex (Fig. 4A) coupled with a decrease (Fig. 4B) in temporal, occipital, and pre-frontal cortex. At a regional level, similar longitudinal distributions of deviant ROIs in CSAs have been observed for task-based fMRI, 17 CVR, 60 diffusion tensor imaging (DTI),24–26,61 and neurophysiological impairment. 27 Lack of consistent localization of these GM volumetric changes is likely attributable to player-specific patterns of mTBI history (location, magnitude, and frequency).18,58
Documenting and validating the loci of dCSF and GM volumetric changes should aid future investigations to explore regional alterations in brain physiology. Lack of volumetric changes in WM could be explained by the absence of immediate large-scale axonal loss, 62 sensitivity of MRI as opposed to DTI to detect WM changes, 24 and the relatively long duration for neuroinflammation to manifest as WM degeneration. 63
Future intervention strategies for changes such as those that were here observed require us to explore possible mechanisms governing these volumetric changes. Longitudinal changes in volumetric measures of GM and dCSF (Table 2) reach a maximum 4–8 weeks after the cessation of collision activity and return to normal after 15–20 weeks of rest from collision-related activity. GM changes could be perfusion induced,64–66 with apoptosis of cortical cells peaking only after 1 week post-injury.67,68 dCSF increase could be attributed to improper waste metabolism within the glymphatic system,69,70 leading to a progressive enlargement of the ventricles. The cumulative effect of these asymptomatic volumetric changes could lead to the manifestation of a more gross and recognizable symptomatic pathology.
The exact mechanism of interaction of these tissue-specific volumetric changes and how they play a combined role in explaining asymptomatic repetitive HAE-induced injury remains yet to be quantified, but several hypothesized key pathways linking these neurological observations are presented in Figure 5. Pathologies such as anorexia nervosa71–74 and dehydration75,76 present with similar volumetric observations and therefore might narrow down the actively involved metabolic regulatory mechanisms. The acute edema, neuroinflammation, 24 and oxidative stress 77 from repetitive asymptomatic injuries could possibly lead to reactive astrogliosis, 78 microglial activation, 79 and alteration of astrocyte density and metabolism,80–82 coupled with reduced neurogenesis,83–85 mitochondrial dysfunction,86,87 and excitotoxicity.88,89 Efforts at harmonization of these mechanisms lead us to hypothesize a connection between glymphatic system dysregulation and repetitive mTBI. These mechanisms are possible precursors of large-scale systemic metabolic alterations, arising from accumulation of HAEs over longer periods of collision-based activity.

Hypothesis of pathophysiological mechanisms linking repetitive mTBI (as associated with exposure to HAEs) to observed reversible changes in GM and dCSF volumes. Other disorders (yellow) known to effect similar changes in GM and dCSF, in addition to changes in WM that were not observed herein, are depicted along with key pathways (blue) hypothesized to lead to these neurological observations (green). CSF, cerebrospinal fluid; CTE, chronic traumatic encephalopathy; dCSF, ventricular (or “deep”) cerebrospinal fluid; GM, gray matter; HAEs, head acceleration events; mTBI, mild TBI; TBI, traumatic brain injury; WM, white matter.
Footnotes
Authors' Contributions
T.T. and E.N. conceived the project and designed the protocol. P.K., T.S., D.S., and G.T. were involved in imaging data collection. R.L. and T.L. were involved in HAE data collection and censoring. P.K. performed the rest of the data pre-processing and pipeline development. T.T. and P.K. reviewed and wrote the manuscript.
Funding Information
This work was supported by the Indiana CTSI Spinal Cord and Brain Injury Research Fund, BrainScope Inc./GE-NFL Head Health Initiative, Indiana CTSI Collaboration in Translational Research Grant, Indiana State Department of Health, and Big Ten Academic Alliance.
Author Disclosure Statement
No competing financial interests exist.