
Abstract
Within the mild traumatic brain injury (mTBI) population, there is heterogeneity both in symptom presentation and recovery patterns. Components of the fear-avoidance model (FAM) may be useful in understanding this heterogeneity. This longitudinal study aimed to identify latent trajectory classes of postconcussion symptoms (PCS) and evaluate how these classes differ on components of the FAM, following mTBI compared with controls. Participants included 185 patients with mTBI and 180 patients with orthopedic injury. PCS, catastrophizing, activity avoidance, somatic focus, depression, participation restrictions and satisfaction were measured 2 weeks, 3, 6, and 12 months post-injury. Multivariate latent class growth analysis identified classes of participants with similar longitudinal trajectories on three variables: cognitive, emotion, and somatic symptoms. Demographic and injury characteristics were used to predict class membership. Class membership was used to predict FAM outcomes. In the mTBI group, Class 1 (C1, 5.9%) had very high maintained symptoms. Class 2 (C2, 20.5%) had high decreasing symptoms. Class 3 (C3, 19.5%) had moderate decreasing symptoms. Class 4 (C4, 54%) experienced low decreasing symptoms. Belonging to class 1 or 2 predicted worse outcomes, including higher catastrophizing, activity avoidance, depression, and participation dissatisfaction. In the control group, two classes were found. Findings highlight the heterogeneity within the mTBI population and the universal disabling impact of person-related behavioral characteristics across medical conditions. Persistent symptoms management and education after mTBI should target those with higher emotion and somatic symptoms, catastrophizing, and depression at 2 weeks post-injury. Interventions targeting catastrophizing, avoidance behaviors, and emotional health may assist in recovery.
Introduction
Traumatic brain injury (TBI) is a leading cause of disability and death worldwide, with approximately 80–90% of TBI classified as mild TBI (mTBI). 1,2 mTBI can cause physical (e.g., vestibular symptoms), cognitive (e.g., attention), and emotional (e.g., depression and anxiety) symptoms. While the prevailing expectation after an mTBI is that these symptoms typically resolve within 3 months, 3 –5 some symptoms may be long lasting, 6 known as persistent postconcussion symptoms (PCS). These can negatively influence the patient’s quality of life and societal participation, causing disability and depression. 7
It has been shown that within the mTBI population, there is heterogeneity both in symptom presentation and recovery patterns. 5,8,9 A study by Keatley et al. 10 assessed 253 patients with mTBI over four time points (after injury, and 1, 3, and 6 months post-injury). Group-based trajectory modeling was used to identify distinct patterns of mTBI recovery, as measured by PCS using scores from the Rivermead Postconcussion Symptoms Questionnaire (RPQ). Four linear symptom trajectories were identified, with three of the groups showing decreasing symptoms over the 6 months. The first group (9.1%) showed minimal acute symptoms, the second group (44.7%) experienced mild acute symptoms, and the third group (32.8%) experienced high acute symptoms, with symptoms in all three groups gradually decreasing over the 6-month period. Group 4 (13.4%) experienced high acute symptoms with increases over time. Using unadjusted multinomial logistic regression analysis, it was found that female sex, history of depression, and history of other psychiatric disorders were associated with membership in the group that experienced higher acute symptoms worsening over time (group 4) compared with the group with mild acute symptoms (group 2). Additionally, a higher level of education and the absence of loss of consciousness (LOC) were protective factors associated with membership in the minimal symptoms group (group 1). Keatley et al. 10 also found significant differences between the trajectory groups in self-reported symptoms of depression, anxiety, pain, and sleep disturbance at 1 month post-injury. With the high acute increasing group (group 4) reporting the highest (least favorable) scores and the minimal acute symptoms group (group 1) reporting the lowest (most favorable) scores on these measures.
While the study from Keatley et al. 10 gives valuable insight into symptom trajectories over a 6-month period, studies show that symptoms can continue for years 6,8 and it would be useful to explore these trajectories up to 12 months or even longer. Additionally, it is important to note that next to symptom improvements, outcomes such as depression, life satisfaction, and disability are also important aspects of recovery. 11,12 Chiang et al. 13 investigated the change trajectories of quality of life, global health outcomes, and PCS of 100 participants over the first year following mTBI. Latent class growth models were conducted sequentially on each of the outcome variables. Findings showed that there was a subgroup of participants with mTBI that did not show improvements in these variables. These change trajectories were associated with older age (≥40 years), unemployment 1 month after injury, and lower education level (≤12 years). Additionally, results indicated that recovery from injury is not a linear process, therefore, future studies should include nonlinear models when assessing recovery trajectories. A limitation of the study 13 was the lack of comparison to a nonhead injury trauma control group. It would be useful to include this comparison group, as symptoms, such as noise sensitivity, fatigue, and poor concentration, reported in PCS are not mTBI specific. 14
Possible predictors of outcomes do not only include demographic and injury factors but a complex interaction between predisposing, precipitating, and perpetuating factors is shown. While biomedical, psychological, and social factors contribute to the understanding of the recovery process after mTBI, in the acute stages after injury, biological and neurological factors are more prominent, whereas in the later stages, their contribution lessens, and psychological and social factors are more important for understanding outcomes. 15 –17 Regarding predictors of PCS, injury-related factors (such as post-traumatic amnesia (PTA), LOC, and Glasgow Coma Scale (GCS) scores) do not reliably predict outcomes, while demographic factors such as gender and age, and pre-injury factors such as mental health issues and concurrent anxiety and depression, are the strongest predictors of PCS. 18 –20 A useful framework to understand the disease process of PCS is the fear-avoidance model (FAM). 21 –23 It posits that if symptoms are catastrophically understood as threatening, then symptom-related fear and anxiety may interfere with recovery. This fear and anxiety may lead to safety-seeking behaviors, including hypervigilance, and avoidance of activities that provoke symptoms (for instance, computer work or busy environments such as grocery stores or restaurants, fitness centers). Avoidance of behaviors can contribute to lower rates of return to work, disability, and depression, thus limiting recovery and maintaining symptoms. 23 –25
While the role of demographic, injury, and mental health predictors in the outcomes of PCS has been shown, heterogeneity in recovery is still seen in this population. Therefore, the examination of latent trajectories of recovery may shed light on the factors contributing to the heterogeneity in mTBI recovery, thereby allowing for identification of those individuals requiring further clinical care. To this end, the present study aimed to understand the distinctive trajectories of symptoms (using the subscales of the RPQ cognitive, emotion, and somatic 26 ) over the course of 12 months by applying multivariate latent class growth analysis (MLCGA). The study aimed to explore the prediction of outcomes (FAM components including catastrophizing, avoidance, depression, participation restriction, and satisfaction) using the symptom (cognitive, emotion, somatic) trajectories. As noted by Chiang et al., 13 not having a nonhead injury trauma control group was a limitation of their study; furthermore, the addition of a nonhead injury trauma group will allow for a more nuanced understanding of the evolution of symptoms in mTBI and distinguish brain-injury specific symptom patterns from general injury-related effects. Therefore, an orthopedic injury control group was also part of this study.
Methods
Design
A prospective, longitudinal, multicenter, observational cohort study was conducted at emergency and neurology departments (ED) of six hospitals in the south of the Netherlands. Recruitment took place from 2017 to 2019 (follow-up until 2020). Ethics approval was received from the medical ethics committee of Maastricht University Medical Center (METC 16-4-209). Self-reported questionnaires were endorsed at 4 time points: within the first two weeks (T1), at 3 months (T2), 6 months (T3), and 12 months post-injury (T4).
Participants
Participants were adults who had sustained an mTBI (mTBI group) or a minor orthopedic injury (control group), diagnosed by a health care professional. Orthopedic injury groups are often used as a comparison group in mTBI studies due to their similarities in demographic, psychosocial, and injury-related factors. The inclusion criteria for the mTBI group were: age 18 years or older, fluent in Dutch, able and willing to provide informed consent, diagnosed by their treating health care professional at the ED using the following: a history of impact to the head, GCS score between 13 and 15 at 30 min post-injury or later upon hospital admission. In case of a GCS of 15, at least one of the following: LOC (≤30 min), PTA (≤24 h), and other transient neurological signs (e.g., focal symptoms). Exclusion criteria were a history of neurological disease or injury (e.g., neurodegenerative disease), a history of psychiatric disorders for which hospitalization was needed, a history of drug addiction or under the influence of illicit substances at the time of injury, and use of psychoactive medication known for cognitive side effects. For the control group, the inclusion and exclusion criteria were the same, except participants were required to have received a diagnosis of minor orthopedic injury in the extremities for which no hospital admission or surgery were necessary (e.g., sprain) from a health care professional at the ED, instead of a diagnosis of mTBI. Additionally, the injury could not involve the head, and no LOC, PTA, nor transient neurological signs were allowed.
Measures
Demographic information
Demographic and injury variables were collected at T1. This information included: age, sex, education level (low [primary school education], middle [secondary school education], or high [university/vocational training]), history of mental health treatment (i.e., psychological, psychiatric, or pharmacological interventions for a mental health condition such as anxiety, depression, etc.), GCS score, LOC, and PTA.
Persistent postconcussion symptoms
The RPQ 27 was used to measure the level and severity of postconcussive symptoms over the last 24 h compared with premorbid levels. The 16 items are assessed on a five-point scale from not experienced at all (0) to a severe problem (4). It is a valid and reliable measure in TBI over time. 2,28 Reference data for a Dutch population of patients with TBI has been provided. 29 Rivera 2 suggested a three-factor structure of the RPQ, namely, cognitive, emotion, and somatic domains which remained stable within 1 year after TBI. The cognitive subscale contains three items with a score ranging between 0 and 12. The emotion subscale contains four items, with a score ranging between 0 and 16. The nine item somatic subscale score ranges between 0 and 36. Higher scores are indicative of higher cognitive, emotion, or somatic symptoms. The reference values published for healthy Dutch speaking adults 29 with percentile scores (from 50% to 95%) ranging between 0–2, 0–4, and 0–6, for the cognitive, emotion, and somatic subscales, respectively, aided interpretation of the findings. For ease of interpretation, the authors used the following classification names to delineate the different percentiles: below 50%—low severity; between 50% and 85%—moderate severity; between 86% and 95%—high severity, and above 97%—very high severity.
Catastrophizing about PCS
The PCS Catastrophizing Scale (PCS-CS) 21 was used to measure the level of catastrophizing thoughts regarding postconcussive symptoms. The PCS-CS consists of 13 items, measured on a five-point Likert scale, with higher scores indicating high intensity of catastrophizing. Reliability and validity were sufficient in mTBI samples. 22,30,31
Fear-avoidance behavior
The Fear of Mental Activities Scale 21 was used to measure the level of fear-avoidance regarding PCS and cogniphobia (fear of mental activity 32 ). The 17 items scale consists of two subscales, namely activity avoidance and somatic focus. 30 Scores are rated on a four-point scale (1 = strongly disagree, 4 = strongly agree) with higher scores indicating stronger fear for mental activities. Reliability and validity of the 13-item scale were acceptable in an mTBI sample. 22,30
Depression
The Hospital Anxiety and Depression Scale (HADS) 33 was used to measure the level of depressive symptoms (depression subscale). The seven-item depression self-rated scores range from 0 to 21, with higher scores indicating higher levels of depression. In patients with TBI, a score of eight or higher is indicative of depression. 34,35 The HADS shows good reliability and validity in a Dutch sample 36 and in a TBI sample. 37
Participation restrictions and satisfaction
The restriction and satisfaction scales of the Utrecht Scale for Evaluation and Rehabilitation-Participation (USER-P) 38 were used to measure disability. The instrument measures three aspects of participation: frequency of behaviors, experienced participation restrictions due to the health condition, and satisfaction with participation. Each sum of scale score is converted to a score ranging from 0 to 100. Higher scores indicate good levels of participation (higher frequency, less restrictions, and higher satisfaction). The USER-P is reliable and valid in patients with brain injury and is often used to assess health-related participation in this population. 39
Procedure
Following the diagnosis of mTBI or orthopedic injury at one of the six recruiting hospitals, potential participants were given information about the study by their treating health care professional. Once a patient expressed interest in the study, the patient’s contact information was forwarded to the researcher. At this point, the researcher checked the inclusion and exclusion criteria and scheduled a first measurement within 2 weeks after the injury. This measurement took place with the researcher at the patient’s home or another location (i.e., university). At this meeting, the informed consent was signed, and the participant completed the questionnaires via an online test environment (T1). After completion of the first measurement, participants received notifications for the upcoming follow-up measurements after 3 months (T2), 6 months (T3), and 12 months (T4), which were also completed via an online testing environment. At T2, T3, and T4, participants were given 4 weeks to complete the questionnaires and received a small gift as a token of appreciation for their participation.
Data analysis
Analyses were conducted using SPSS v.27 for Windows, 40 Mplus Version 7.2, 41 and R Version 4.4.1. 42 MLCGA was performed separately for the mTBI and the control groups across all time points (T1–T4). The RPQ cognitive, emotion and somatic variables were modelled jointly per group. The MLCGA models analyze multivariate change over time to isolate distinct latent classes of individuals with similar trajectories of symptom recovery. Missing data were handled by using the full information maximum likelihood estimation method for the MLCGA, therefore, estimated model parameters were based on all available data.
Five MLCGA models (with 1–5 classes) were estimated for both the mTBI and control group data. The model that fitted the following criteria the best was selected: lowest Bayesian Information Criterion (BIC), Akaike Information Criterion (AIC), and sample-size adjusted BIC, entropy <0.90, Vuong-Lo-Mendell-Rubin adjusted likelihood-ratio test (LRT), and the bootstrapped LRT p < 0.05, and best interpretability (i.e., group sizes >10). For the chosen model, each class represented a group of individuals with a shared symptom recovery trajectory across the variables (cognitive, emotion, somatic symptom domains). Slopes and interactions between slopes were tested for significance. Names were provided to each class based on descriptive methods (using the scores and reference values, aided by visual inspection of the trajectories). To assess the impact of class membership as a function of demographic and injury-related characteristics, the robust three-step method (R3STEP) was used to conduct multinomial logistic regression analysis. 43 The distal outcomes three-step method (DU3STEP [distal with uncertainty] and DE3STEP [distal with equality]) 43 was employed to conduct equality of means tests and to examine the predictive role of the latent classes on the variables of catastrophizing, activity avoidance, somatic focus, depression, participation restrictions, and satisfaction at each time point. 43 Bonferroni corrections for multiple comparisons were applied to the equality of means tests with more than 2 classes.
Results
Group characteristics
The total sample included 365 participants, 185 of whom were diagnosed with mTBI (mTBI group) and 180 were diagnosed with orthopedic injury (control group). In Table 1, participant characteristics are reported for both groups separately. The mTBI group was more often male and their cause of injury was more likely due to a traffic accident, than the control group (see Table 1). The table includes the characteristics for all participants, including the ones with missing data for T2–T4. In the mTBI group, 33 participants had missing data for at least one variable at one time point. Specifically, 22 participants had missing data at T2, 10 participants at T3, and 1 participant at T4. In the control group, 22 participants had missing data for at least one variable at T2 and T3. Of these, 2 participants completed the questionnaires at T4, leaving a total of 20 participants with missing data at T4. See Figure S1 in the Supplementary Data for the participant flowchart. The variable characteristics across the samples are presented in Table S1 of the Supplementary Data.
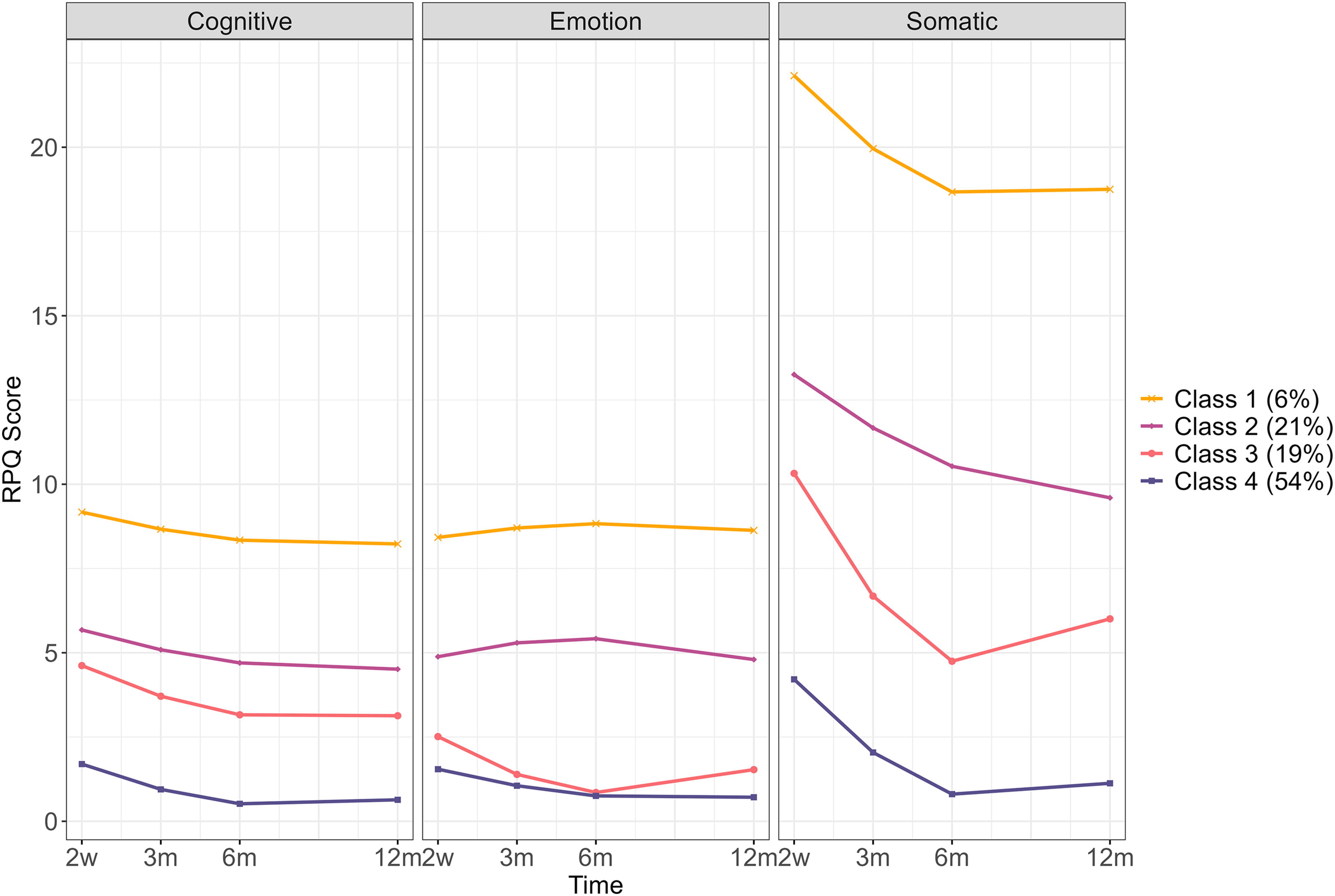
Symptoms Recovery Model mTBI group. 2w = 2 weeks post-injury, 3 m = 3 months post-injury, 6 m = 6 months post-injury, 12 m = 12 months post-injury. mTBI, mild traumatic brain injury; RPQ Score, Rivermead Postconcussion Symptom Questionnaire Score.
Participant Characteristics for Mild Traumatic Brain Injury and Control Groups
Fisher exact test was used.
GCS, Glasgow Coma Scale; LOC, loss of consciousness; PTA, post-traumatic amnesia; SD, standard deviation; –, data are not applicable for this group.
mTBI group
Regression Results Explaining Class Membership in the Mild Traumatic Brain Injury Group
p < 0.05; ** p < 0.001.
Reference class = C4; Edu, education; LOC, loss of consciousness; SE, standard error; PTA, posttraumatic amnesia.
Equality Tests for Means across Classes for the Mild Traumatic Brain Injury Group
AA, Activity Avoidance; HADS-D, Hospital Anxiety and Depression Scale; PCS-CS, Postconcussion Symptoms Catastrophizing Scale; SF, Somatic Focus; USER-P Rest, Utrecht Scale for Evaluation and Rehabilitation-Participation Restrictions Scale; USER-P Sat, Utrecht Scale for Evaluation and Rehabilitation-Participation Satisfaction Scale; df for overall test = 3.
Predictors of class membership
The “low symptoms decreasing” class (C4) was used as the reference class. In Table 2, the results of the multinomial logistic regression (R3STEP) analysis are shown. Females (odds ratio [OR] = 5.68, 95% confidence interval [CI] = 1.30, 24.83), those who had a history of mental health treatment (OR = 16.58, 95% CI = 3.50, 90.93), and those with a low (OR = 2141, 95% CI = 137.2, 33775.1) or middle education (OR = 2586.1, 95% CI = 137.2, 33775.1) were statistically significantly more likely to be in the “very high symptoms maintained” class (C1) compared with the “low symptoms decreasing” class (C4). Higher education was considered a protective factor with extremely low odds of participants being in the “very high symptoms maintained” class (C1) or the “high symptoms decreasing” class (C2).
Outcomes prediction
To assess if the latent classes predicted catastrophizing, activity avoidance, somatic focus, depression, participation restrictions, and satisfaction, at the different time points (T1–T4), equality of mean tests (DU3STEP and DE3STEP) were conducted. The significant differences between classes are presented in Figure 2 for significant overall equality of mean tests (results in Table 3). At 2 weeks (T1), catastrophizing, depression, and participation satisfaction differed significantly between the classes (see Table 3). The “moderate symptoms decreasing” class (C3) had lower catastrophizing than the “high symptoms decreasing” (C2) and “low symptoms decreasing” (C4) classes, and lower depression than C4. The “very high symptoms maintained” (C1) and “high symptoms decreasing” classes (C2) had lower participation satisfaction compared with the “low symptoms decreasing” class (C4) (see Fig. 2).
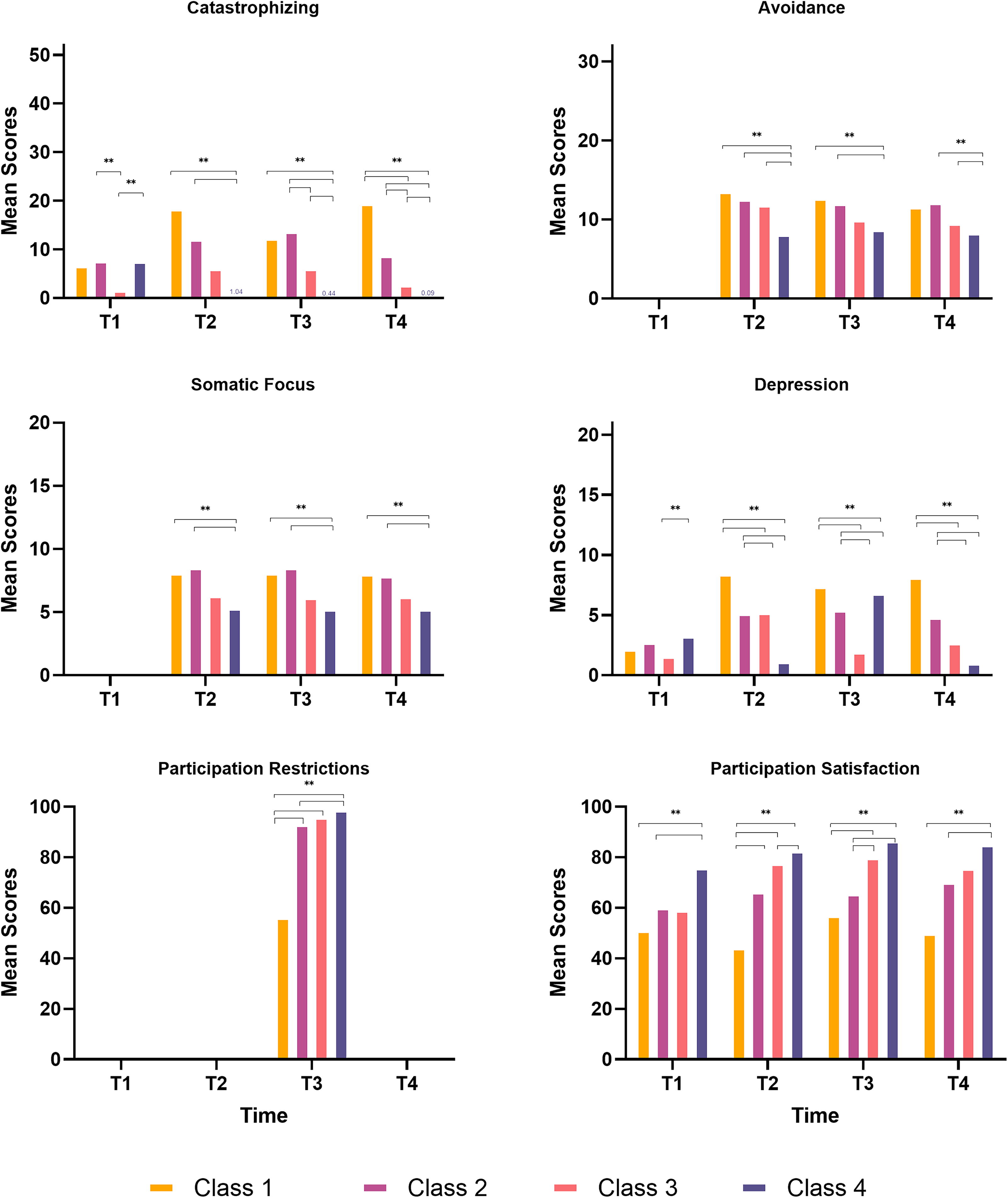
Equality of means tests for mTBI group. T1 = 2 weeks post-injury, T2 = 3 months post-injury, T3 = 6 months post-injury, T4 = 12 months post-injury.
At 3 and 6 months (T2 and T3), class membership was a significant predictor for catastrophizing, activity avoidance, somatic focus, depression, and participation satisfaction (see Table 3). C1 and C2 scored worse (higher scores) on all outcomes compared with C4. C3 showed higher activity avoidance at 3 months, and higher catastrophizing at 6 months, than C4. C1 reported the lowest participation satisfaction at 3 months and, along with C2, at 6 months. At 6 months, C1 also had greater participation restrictions than other classes (see Fig. 2).
At 12 months (T4), C1 and C2 reported higher catastrophizing, somatic focus, depression, and lower satisfaction than C4. Both C2 and C3 had higher activity avoidance than C4, though C1 did not differ significantly (see Fig. 2).
Control group
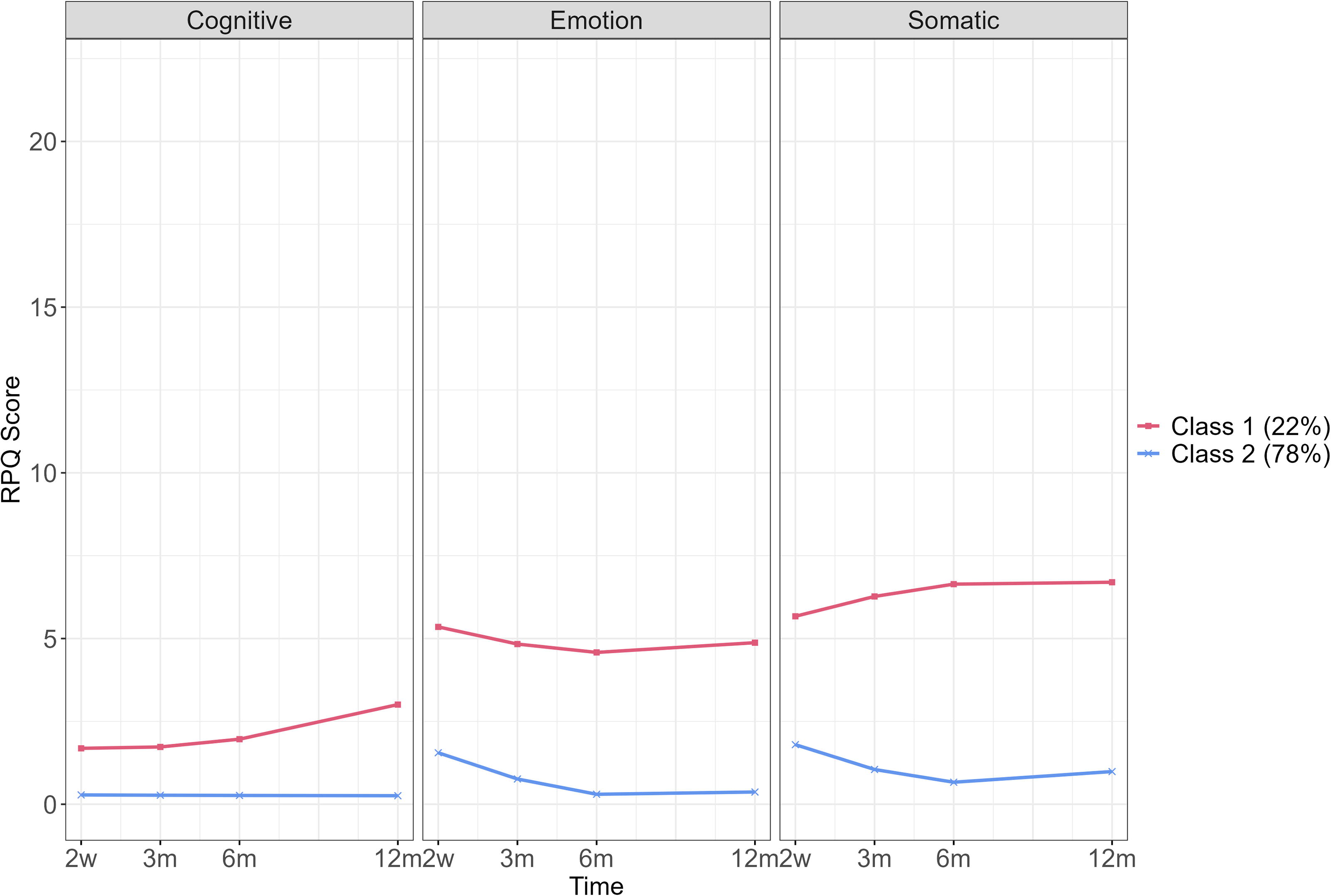
Symptoms Recovery Model control group. RPQ Score, Rivermead Postconcussion Symptom Questionnaire Score; 2w = 2 weeks post-injury, 3 m = 3 months post-injury, 6 m = 6 months post-injury, 12 m = 12 months post-injury.
Regression Results Explaining Class Membership in the Control Group
p < 0.001.
Class 2 is the reference class. Edu, Education; SE, standard error.
Equality Tests for Means Across Classes for the Control Group
AA, Activity Avoidance; HADS-D, Hospital Anxiety and Depression Scale Depression scale; PCS-CS, Postconcussion Symptoms Catastrophizing Scale; SF, Somatic Focus; USER-P Rest, Utrecht Scale for Evaluation and Rehabilitation-Participation Restrictions Scale; USER-P Sat, Utrecht Scale for Evaluation and Rehabilitation-Participation Satisfaction Scale.
Predictors of class membership
The “low symptoms decreasing” class (CC2) was used as the reference class. Table 4 shows the results of the multinomial logistic regression analysis (R3STEP). Participants with a history of mental health treatment (OR = 8.17, 95% CI 2.52, 26.47) were significantly more likely to be in the “moderate symptoms increasing” class (CC1). Having a middle (OR = 0.16, 95% CI 0.07, 0.40) or high (OR = 0.18, 95% CI 0.18, 0.18) education level was a protective factor and associated with a significantly higher likelihood of participants being in the “low symptoms decreasing” class (CC2). No other variables were significant predictors of class membership.
Outcomes prediction
To assess if the latent classes predicted catastrophizing, activity avoidance, somatic focus, depression, participation restrictions and satisfaction, equality of means tests (DU3STEP and DE3STEP) were conducted. The significant differences between classes are presented in Figure 4 for significant overall equality of means tests (results in Table 5). At 2 weeks (T1), catastrophizing, activity avoidance, somatic focus, depression, and participation satisfaction were significantly different between the classes (see Table 5). The “moderate symptoms increasing” class (CC1) had significantly less favorable scores than the “low symptoms decreasing” class (CC2). At 3 months (T2), the latent classes significantly predicted catastrophizing, somatic focus, depression, and participation satisfaction. Again, with the “moderate symptoms increasing” class (CC1) scoring significantly less favorably than the “low symptoms decreasing” class (CC2). At 6 and 12 months (T3 and T4), the class membership significantly predicted catastrophizing, activity avoidance, and somatic focus, with the same pattern as above being shown (CC1 > CC2).
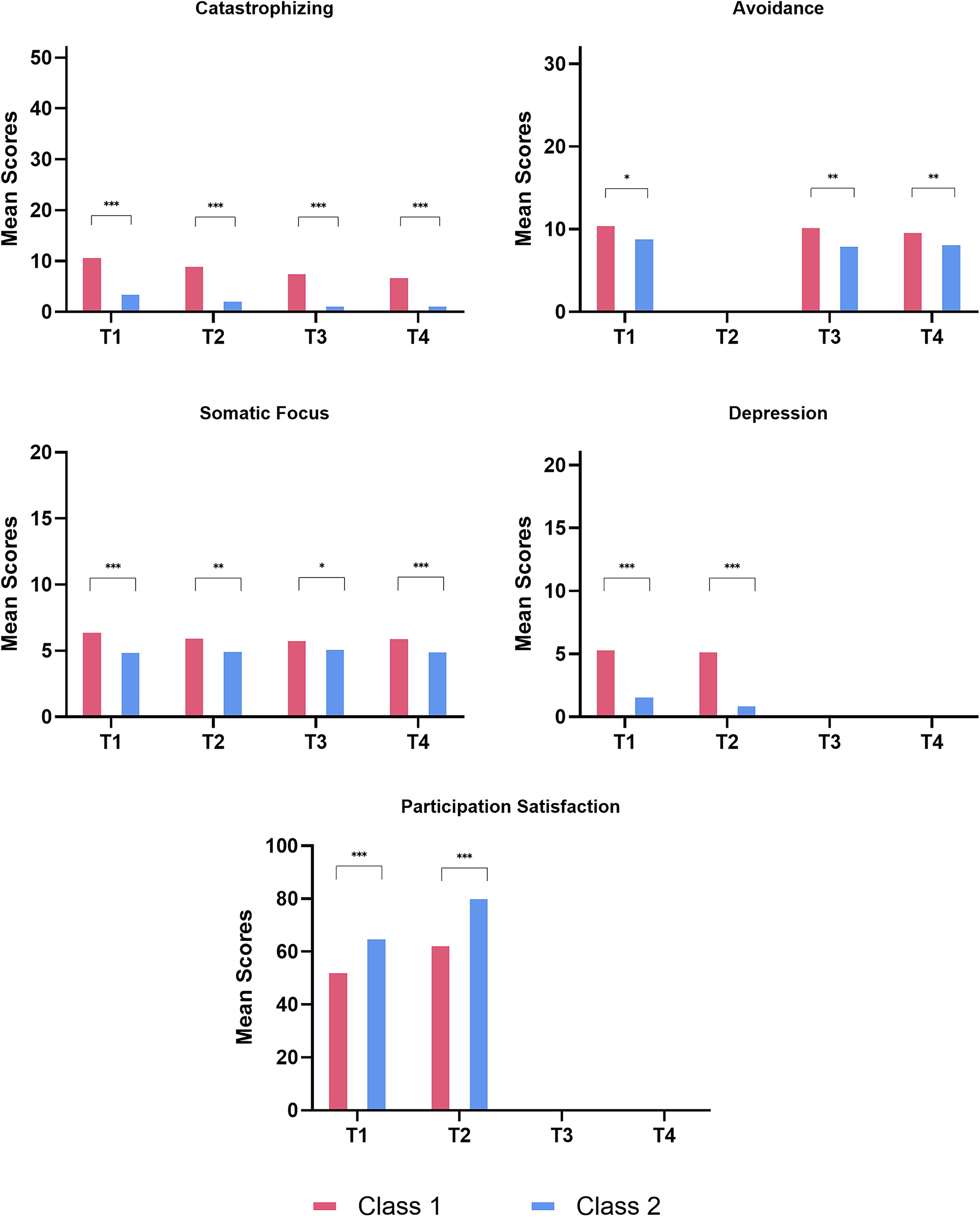
Equality of means tests for control group. T1 = 2 weeks post-injury, T2 = 3 months post-injury, T3 = 6 months post-injury, T4 = 12 months post-injury.
Discussion
This study aimed to investigate the trajectories of symptoms (cognitive, emotion, and somatic) over 12 months using MLCGA in patients with mTBI and orthopedic injury controls. Four distinct classes of patients with mTBI were found, namely, class 1 (C1, 5.9%): “very high symptoms maintained,” class 2 (C2, 20.5%): “high symptoms decreasing,” class 3 (C3, 19.5%): “moderate symptoms decreasing,” and class 4 (C4, 54%): “low symptoms decreasing.” The control group had 2 distinct classes, class 1 (CC1, 22.2%): “moderate symptoms increasing” and class 2 (CC2, 77.8%): “low symptoms decreasing.”
The findings of the present study relate to the previous literature 10 where similar trajectories of symptom recovery over time were found. The present study found a group of participants with very high symptoms that were maintained over the year, unlike the study of Keatley et al., 10 who found a group with high symptoms that continued to increase over time. This contrasting result may be due to the differences in the sample demographics between the papers as the sample in the Keatley et al. 10 study had higher rates of LOC, PTA, history of depression, and other psychiatric disorders, and higher RPQ total scores at baseline. This would suggest that the current sample may include individuals with milder injuries and symptoms.
To our knowledge, this is the first study to use MLCGA to characterize trajectories of recovery using the symptom subscales of the RPQ, 2 namely, cognition, emotion, and somatic symptoms, in a cohort of adults with mTBI compared with controls. Findings showed that in all the domains, the very high symptoms maintained class (C1) experienced the highest symptoms (cognitive, emotion, somatic) of all the classes in the mTBI group. For the cognitive symptoms, a similar pattern over time was seen in all the classes in the mTBI group, such that symptoms steadily declined starting from 2 weeks post-injury. A similar pattern was seen in CC2 of the control group. However, for CC1 in the control group, the opposite pattern emerged over time where symptoms increased steadily compared with the mTBI group. In the mTBI group, C1 and C2 had a similar trajectory for emotion symptoms, where symptoms increased steadily until 6 months, where they reached their peak and then lessened. For C3 and C4, the opposite pattern was shown where emotion symptoms steadily decreased from between 2 weeks until 6 months where they were lowest, and then increased slightly until 12 months. In the control group, both classes (CC1 and CC2) showed a similar pattern to that of C3 and C4 in the mTBI group. Across all of the classes in the mTBI group, somatic symptoms were higher than cognitive or emotion symptoms. A similar pattern was seen across all the classes for somatic symptoms, when symptoms were at their highest 2 weeks post-injury, and then decreased to their lowest point at 6 months, with increases seen at 12 months although scores were lower than at 2 weeks. In the control group, a similar pattern was shown for CC2 as seen in the mTBI group, however, for CC1, the trajectory was the opposite with the lowest scores seen at 2 weeks post-injury, and steadily increasing until 12 months post-injury.
These findings confirm that even at 12 months, there are still some participants who do not fully recover from mTBI symptoms. Additionally, symptoms are not specific to mTBI alone and are found in other patient populations (such as orthopedic injury groups), showing that aspects other than biological factors play a significant role in the persistence of these symptoms not only in mTBI populations but also nonhead injuries as well. The variability of trajectories over time across the three domains (cognitive, emotion, somatic) demonstrates the need to distinguish recovery timelines of each domain. While the cognitive symptoms decline over time in all classes, the peak shown in the emotion symptoms at 6 months, seen in C1 and C2 only, may suggest the influence of secondary factors including psychosocial stressors that may be intertwined with the rise in somatic symptoms seen around this time post-injury. These findings demonstrate the need for targeted holistic treatments focusing on mental health.
In the mTBI group, females, those with a history of mental health treatment, and those with a low or middle education level were more likely to experience higher symptoms that were maintained over time (C1). In the control group, participants with a history of mental health treatment were more likely to be in the symptoms increasing trajectory. In both the mTBI and control groups, high education level was a protective factor. These findings were consistent with previous studies. 10,13
To our knowledge, this is the first study to relate class membership to outcome variables of the FAM model (including catastrophizing, avoidance, depression, and participation restrictions). Findings highlight significant distinctions in psychological and participation-related outcomes across symptom trajectory classes over time. In the mTBI group, at the early stage (2 weeks post-injury), catastrophizing, depression, and participation satisfaction were predicted by class membership. During this initial phase, participation satisfaction was lowest in the very high symptoms maintained class (C1) which may be expected due to the very high symptoms experienced. Interestingly, the moderate symptoms decreasing class (C3) demonstrated more favorable outcomes, with lower catastrophizing and depression. This finding may be explained by the expectations of recovery at 2 weeks post-injury, whereby individuals are often told to expect symptoms but that they should recover. Therefore, if symptoms are worse than expected (such as in the very high and high symptoms groups), individuals may catastrophize more about recovery and the negative meaning behind symptoms, whereas those in the moderate symptoms group are experiencing symptoms aligned to their expectations and therefore catastrophizing is lower. Additionally, depression was lower in the moderate symptoms decreasing class (C3) than in the other classes, although across all classes depression was not at clinically relevant levels (above 8).
Over the medium term (3–6 months), those belonging to classes with higher symptoms (C1 and C2) experienced worse outcomes (higher scores on catastrophizing, activity avoidance, somatic focus, depression, and lower participation satisfaction) than those in classes with low symptoms. At 6 months, those in the very high symptoms maintained class (C1) also experienced greater participation restrictions. At both 3 and 6 months, those in the very high maintained class (C1), experienced clinically relevant scores on depression (above 8). These findings suggest that as expected, individuals that have higher symptom severity also experience negative thoughts about symptoms, intensely focus on symptoms, and avoid activities that may worsen symptoms. This can significantly affect individuals’ overall quality of life, mood, and daily functioning. The findings show that the opposite is also true, such that when symptom severity is lower, individuals do not experience high catastrophizing, somatic focus, activity avoidance, and depression. The above findings are in line with previous literature suggesting that catastrophizing, 22 avoidance behaviors, 23,44 and depression 45 are predictive of symptoms and disability, underscoring the need for holistic, early-intervention approaches that address all aspects of recovery.
At long-term follow-up (12 months), unfavorable outcomes (higher catastrophizing, somatic focus, depression, dissatisfaction) were still seen in classes with higher symptoms (C1 and C2) compared to those with low symptoms. Additionally, higher activity avoidance was experienced by those belonging to the high (C2) and moderate (C3) symptom decreasing classes compared to those with low symptoms. In the control group, those in the increasing symptoms class (CC1) experienced more catastrophizing, activity avoidance, somatic focus, depression, and were less satisfied with participation at the different time points across the 12 months.
The findings of the present study suggest that factors such as catastrophizing and depression at 2 weeks post-injury are predicted by symptom recovery trajectories and patients with these tendencies and higher symptom severity may be at risk for nonrecovery after mTBI. This is in line with recent guidelines suggesting screening for depression after concussion as this is a predictor of concussion outcome. 46 Patients that also have high catastrophizing, somatic focus, activity avoidance, depression, and less satisfaction are more likely to be in the groups with higher symptoms that may be less likely to recover at 12 months. The overlap of factors between the mTBI and control groups, including the history of mental health treatment and education, as well as the components of the FAM demonstrate the importance of these factors in generating nonrecovery risk profiles to assist in early management of these conditions. These findings indicate that treatment in the initial phase should be directed using an holistic approach and that treatment of persistent symptoms between 3 and 6 months should consider targeting catastrophizing, activity avoidance, and somatic focus specifically, to indirectly influence symptom levels, depression, participation satisfaction, and recovery trajectories.
A strength of the present study is that this is the first study to utilize MLCGA with the subscales of the RPQ (cognitive, emotion, and somatic symptoms) and investigate the prediction of the components of the FAM using class membership over time with longitudinal analysis. This adds more information to the profiles of recovery following mTBI and provides further understanding of the heterogeneity in this population. Furthermore, adding these different components may allow for more targeted intervention to prevent or treat persistent symptoms and nonrecovery following mTBI. This study is also the first to add a nonhead injury-related nonhealthy control group, the orthopedic injury group. While this group is not a true control group in the traditional sense, it is an essential control for injury and trauma related confounders (e.g., visiting an Emergency Department after an accident). The addition of the orthopedic injury group allows for comparison of the findings from the mTBI group to the controls and provides further evidence to the universality of these symptoms and the relevance of the FAM components across conditions. Furthermore, while the sample sizes are not overly large, a number of criteria (including bootstrapping resampling and sample-adjusted BIC) were used to ensure that a usable number of clusters that were clinically meaningful were gained from the data, providing understanding of the underlying structure of the current data. A limitation of the study is that participants were those who presented at an emergency department for their injury, and thus they are not representative of all patients with mTBI. Additionally, certain racial and ethnic minorities may be underrepresented in the data due to the data being collected at six hospitals in the Netherlands, therefore the data may not be generalizable to populations with different demographic profiles. Another limitation of the study is that a causative relationship between the variables cannot be established as they are predictive but not causative. Additionally, it is possible that other predictors that were not taken into account in these models may be relevant predictors of these trajectories. Future research could further study the FAM in this population using other analyses techniques to determine the causative relevance of this model.
In conclusion, the present study robustly confirms the heterogeneity in the mTBI population by identifying distinct trajectories of recovery and their associated risk factors. Crucially, it underscores that a substantial subset of individuals does not fully recover after mTBI, with specific risk profiles emerging. Females, individuals with a history of mental health treatment, and those with low to middle education levels are particularly vulnerable to poor recovery outcomes. Additionally, individuals with moderate to very high somatic symptoms, moderate emotion symptoms, and high catastrophizing and depression at 2 weeks are at risk of nonrecovery at 12 months. Furthermore, those with continued high-somatic symptoms, increased emotion symptoms over the medium term (3 and 6 months), and have heightened catastrophizing, activity avoidance, and somatic focus are at risk of higher depression, participation restrictions and dissatisfaction, and nonrecovery.
Importantly, this study highlights actionable insights for clinical practice. The findings emphasize the window of 2 weeks post-injury for identifying at risk individuals. Findings highlight the strong impact of psychological and behavioral factors (such as those in the FAM) in symptom recovery and the relevance of the fear-avoidance dynamics, especially avoidance behaviors, across different health conditions. Additionally, these findings suggest that interventions focusing on components such as catastrophizing and avoidance may be beneficial to individuals experiencing PCS, especially if these symptoms are still present as early as 3 months after injury. This research not only advances our understanding of mTBI recovery, but may also provide a framework for early, personalized, and more effective intervention strategies, indicating that recovery (in general) needs to be seen from an holistic view of health. This approach has the potential to mitigate long-term burden of mTBI on individuals and health care systems alike, offering a roadmap for improved care and better recovery trajectories.
Transparency, Rigor, and Reproducibility Summary
This study and analysis plan was not preregistered. Data for the present study was collected as part of a larger data collection effort investigating outcome after mTBI. A total of 445 patients with mTBI and 475 patients with orthopedic injury were assessed for eligibility in the longitudinal study. A total of 186 patients with mTBI and 181 orthopedic injury controls were included. A total of 185 patients with mTBI and 180 patients with orthopedic injury completed the questionnaires at T1. While sample sizes are not overly large, careful consideration was given to determining the number of usable, clinically meaningful, clusters in the data and a number of fit indices were utilized to this end. No power calculations were done separately for the present study. Blinding of participants and researchers was not relevant as this was a longitudinal prospective cohort study in which participants completed (online) questionnaires. Data acquisition and analyses are reported in the methods section. All equipment and software used to perform the acquisition and analysis are widely available (e.g., SPSS, Mplus) and open access and freely available (in the case of R). Statistical analysis was performed by S.K. and J.S. with relevant qualifications. No replication or external validation studies have been performed or are planned/ongoing at this time to our knowledge. De-identified data from this study are not available in a public archive. Analytic code are available upon reasonable request to the principal investigator at Maastricht University (CvH).
Footnotes
Authors’ Contributions
S.K.: Conceptualization, formal analysis, and writing—original draft. I.W.: Conceptualization, writing—review and editing, and supervision. M.W.: Conceptualization, methodology, investigation, data curation, and writing—review and editing. J.S.: Formal analysis and writing—review and editing. S.S.: Conceptualization, methodology, and writing—review and editing. J.V.: Conceptualization, methodology, and writing—review and editing. M.R.: Conceptualization, writing—review and editing, and supervision. J.v.d.N.: Conceptualization, writing—review and editing, and supervision. C.v.H.: Conceptualization, methodology, writing—review and editing, supervision, project administration, and funding administration.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
The project was funded by The Brain Foundation Netherlands (Hersenstichting) under the grant number: DR-2020-00368.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.