
Abstract
Isolated traumatic spinal cord injury (t-SCI) and traumatic brain injury (TBI) represent significant public health concerns, resulting in long-term disabilities and necessitating sophisticated care, particularly when occurring concurrently. The impact of these combined injuries, while crucial in trauma management, on clinical, socioeconomic, and health care outcomes is largely unknown. To address this gap, our secondary retrospective cohort study used data from the Japan Trauma Data Bank, covering patients enrolled over a 13-year period (2006–2018), to elucidate the effects of concurrent t-SCI and TBI on in-hospital mortality. Data on patient demographics, injury characteristics, treatment modalities, and outcomes were analyzed. Multivariate logistic regression analysis was performed to examine prognostic variables associated with in-hospital mortality, including interaction terms between t-SCI severity and TBI presence. This study included 91,983 patients with neurotrauma, with a median age of 62 years (69.7% men). Among the patients, 9,018 (9.8%) died in the hospital. Concomitant t-SCI and TBI occurred in 2,954 (3.2%) patients. t-SCI only occurred in 9,590 (10.4%) patients, whereas TBI only occurred in the majority of these cases (79,439, 86.4%). Multivariate logistic regression analysis revealed age; sex; total number of comorbidities; systolic blood pressure at presentation; Glasgow coma scale score at presentation; and Abbreviated Injury Scale (AIS) scores for head, face, chest, abdomen, cervical-SCI, thoracic-SCI, and lumbar-SCI as significant independent factors for in-hospital mortality. The odds ratio of cervical-SCI × head AIS as an interaction term was 0.85 (95% confidence interval: 0.77–0.95), indicating a negative interaction. In conclusion, we identified 12 factors associated with in-hospital mortality in patients with t-SCI. In addition, the negative interaction between cervical t-SCI and TBI suggests that the presence of t-SCI in patients with TBI may be underestimated. This study highlights the importance of early recognition and comprehensive management of these complex trauma conditions while considering the possibility of concomitant t-SCI in patients with TBI.
Introduction
Traumatic spinal cord injury (t-SCI) refers to damage to the spinal cord, with or without vertebral fractures, caused by an external physical force on the axial skeleton and its ligaments, resulting in partial or total loss of motor, sensory, and autonomic functions, which is rarely reversible. However, in some patients, early decompressive and reconstructive spine surgery can improve neurological deficits. 1,2 Besides causing lifelong suffering for patients and their families, t-SCI incurs high medical and societal costs in both its acute and chronic phases. 3,4 This long-term disability presents challenges to traumatologists, orthopedic surgeons, neurosurgeons, and rehabilitationists, 5 with the associated health care burdens indicating a serious public health and socioeconomic concern. 6
Traumatic brain injury (TBI) is another devastating injury. In particular, a Glasgow coma scale (GCS) score ≤8 indicates severe TBI (s-TBI), posing significant risks of long-term disability and mortality. 3,7 Similarly, moderate and mild TBI can result in lifelong health problems and disability due to irreversible damage to the central nervous system. 8 –10
The cranium and cervical spine are vulnerable to concurrent injuries owing to their close anatomical and biomechanical relationship. Specifically, head impact is particularly likely to cause cervical spine injury, particularly at the cranio–cervical junction. Neurological assessment is essential for diagnosing t-SCI; however, identifying spinal cord damage from physical findings in the presence of s-TBI, where the patient is in a comatose or minimally conscious state, as indicated by a GCS score ≤8, is difficult. 11 Conversely, in the presence of t-SCI, the impact of intracranial injury may be difficult to isolate, which can be problematic in trauma care, particularly in severely traumatized patients on neurocritical care mechanical ventilators. 12 Failure of physicians and nurses to diagnose concomitant injuries accurately in the acute phase can exacerbate the initial damage, risking secondary damage to the nervous system due to misdirected trauma care, 13 because of underestimation of one of the two neurotrauma mechanisms. While several studies have examined the incidence and prevalence of combined craniospinal injuries, 14,15 the impact of these injuries on clinical outcomes, treatment implementation, and rehabilitation capacity remains largely unknown. In addition, recent studies have attempted to elucidate the pathophysiology of multiple traumas by evaluating the interactions between complex injured regions. 16 –18
We hypothesized that examining the interactions between craniocerebral and spinal cord injuries can provide a new perspective on neurotrauma and intensive care. Given its potential for severe sequelae either from the combination itself or from delayed treatment, concomitant craniospinal injury represents a complex trauma, indicating the importance of accurate epidemiological data and characteristics in guiding investigations and patient management.
In this study, we aimed to describe the epidemiological characteristics of concomitant craniospinal injuries and the role of their interaction in the risk of fatal injuries. We also investigated modifiable variables and assessed their impact on in-hospital mortality and permanent disability in these patients.
Methods
Study design and settings
The Japan Trauma Data Bank (JTDB) is a nationwide, multicenter, prospective observational trauma registry that includes all consecutive trauma patients encountered in Japan. It was introduced nationwide in 2003 and registered data from 292 hospitals as of March 2021. The Japanese Association for Surgery of Trauma and Japanese Association of Emergency Medicine established the JTDB to improve and ensure medical care quality in Japan. Data are continuously recorded online through the internet and stored on the data server of the Japan Trauma Care and Research (JTCR). Patients with suspected injuries of Abbreviated Injury Scale (AIS) 19 scores ≥3 are registered in the JTDB, mainly from tertiary care hospitals and emergency centers. The database includes data on age, sex, injury mechanism (eight accident types: car accident, motorcycle accident, bicycle accident, traffic accident [pedestrian], crashes from heights, falls from stairs, falls on the ground, other trauma), time from onset to arrival, preexisting comorbidities, vital signs on arrival, GCS score, 20,21 AIS, 19 Injury Severity Score (ISS), 22 Revised Trauma Score (RTS), 23 and Trauma and Injury Severity Score (TRISS). 24
Institutional members of the JTCR have access to anonymized data in the JTDB. We obtained data from the JTCR, with permission to conduct a secondary retrospective observational study. Anonymized data were not retrieved from the original patient data in the hospital systems.
Study populations
From January 1, 2006 to December 31, 2018, all patients with TBI or t-SCI enrolled in the database were eligible for this study. Cases involving interhospital transfers, burn injury victims, pregnant women, cardiopulmonary arrest at presentation, patients with an ISS of 75, and those with significant missing data (unknown age, sex, GCS score at presentation, or outcome) were excluded from the analysis (Fig. 1). Interhospital transfers were excluded due to changes in patient conditions caused by therapeutic interventions and to avoid potential double counting in registry data. Patients with burn injuries, pregnancies, cardiopulmonary arrest at presentation, and an ISS of 75 were excluded as these conditions differ from the pathologies targeted in this study.
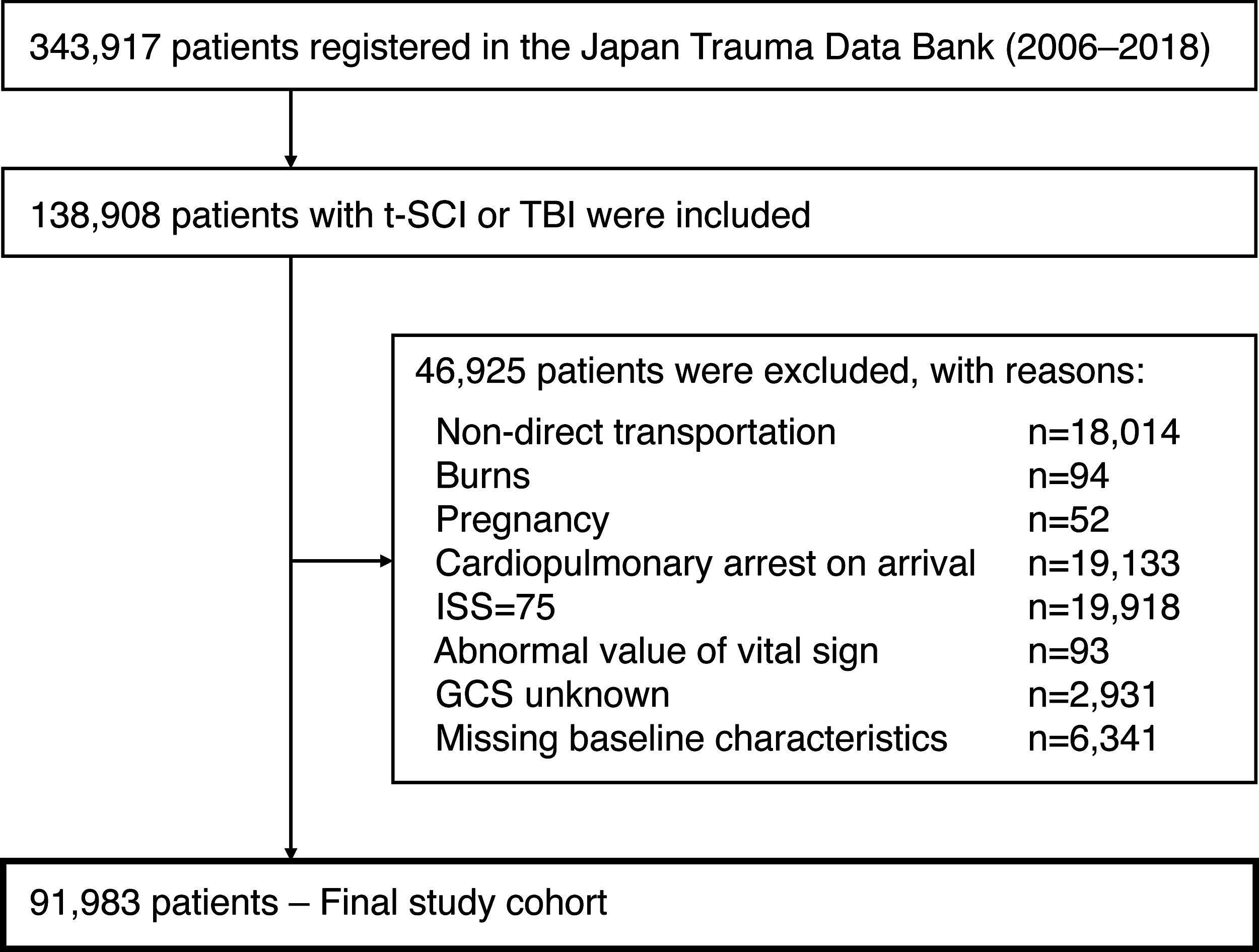
Flow diagram for patient selection. t-SCI, traumatic spinal cord injury; TBI, traumatic brain injury; ISS, Injury Severity Scale; GCS: Glasgow coma scale.
Explanatory variables and definitions
A datasheet with an exclusive set of AIS codes for t-SCIs and spinal fractures was created (Supplementary Table S1). A higher injury level was used for analysis in cases with two or more registered t-SCI sites. The explanatory variables for the multivariable analysis were preselected based on biological plausibility and a priori knowledge. 25,26 The primary end-point was in-hospital mortality.
Statistical analysis
Summary statistics of patient demographic characteristics are presented as medians with numbers, percentages, and interquartile ranges (IQRs), as appropriate. Multivariate logistic regression analysis was performed to examine prognostic variables as possible predictors of in-hospital mortality, with in-hospital mortality used as the objective variable of interest. Crude odds ratios (ORs), adjusted odds ratios (AORs), and their 95% confidence intervals (CIs) for mortality rates were calculated. Potential explanatory variables included age, sex, total number of comorbidities, vital signs at presentation (respiratory rate, heart rate, systolic blood pressure [SBP], and GCS score), and AIS score for each injury site (head, face, neck, chest, abdomen, spine, upper extremity, and lower extremity/pelvis). We subdivided SCI and spinal fractures into cervical-, thoracic-, and lumbar-SCI according to AIS codes to evaluate their interactions with TBI. Multivariate logistic regression analysis included the following three interaction terms in one model: cervical t-SCI × TBI, thoracic t-SCI × TBI, and lumbar t-SCI × TBI. In epidemiology, interaction refers to the situation where the effect of one risk factor (A) on a certain disease outcome is different across strata of another risk factor (B) or vice versa. 27 Multivariate logistic regression analysis was performed using forced entry methods. Explanatory variables for which adjustments were made were physiologically essential or had been identified in relevant previous studies. 25,26 Variance inflation factors (VIFs) were used to check for multicollinearity. 28 Logistic regression analysis was used to estimate the impact of the interaction between t-SCI severity and TBI presence (AIS score ≥3) on in-hospital mortality. In addition, we evaluated the effect size of the cervical t-SCI × TBI interaction term in TBI cases for a more robust analysis. For all statistical inferences, a two-sided p value <0.05 was considered to indicate significance. R software version 4.3.2 (v4.3.2; https://www.r-project.org) was used for all analyses.
Ethical considerations
This study adhered to the principles of the STROBE guidelines and was performed in accordance with the Declaration of Helsinki. 29 The JTDB was approved by the Ethics Committee of the Japanese Society for Trauma Surgery. The approval documents of JTDB and the representative institution can be viewed on the JTDB website (https://www.jtcr-jatec.org/traumabank/dataroom/ethics2.htm). Given the retrospective nature of the study, the requirement for obtaining informed consent was waived. This study was also approved by the Institutional Review Board of Osaka University Hospital (Approval ID No. 16260).
Results
Among 343,917 registered trauma patients in the database, 91,983 patients with neurotrauma were finally included in the present analysis (Fig. 1). The median age of patients was 62 years (interquartile range [IQR]: 38–75 years), and 69.7% of patients were men. The most common injuries were incidental falls on base-level ground (19.5%, n = 17,980) and falls from stairs (16.5%, n = 15,188). At presentation, patients’ median respiratory rate was 20 (IQR: 17–24)/minute, heart rate was 84 (IQR: 72–98) beats/minute, SBP was 138 (IQR: 118–160) mmHg, GCS score was 14 (IQR: 11–15), median ISS was 17 (IQR: 10–25), and median TRISS Ps was 0.94 (IQR: 0.87–0.98). The in-hospital mortality rate was 9.8% (n = 9,018), and the median length of hospital stay was 12 (IQR: 3–31) days (Table 1).
Demographics and Characteristics of Trauma Patients with TBI or t-SCI
TBI, traumatic brain injury; t-SCI, traumatic spinal cord injury; IQR, interquartile range; RR, respiratory rate; HR, heart rate; bpm, beats per minute; SBP, systolic blood pressure; GCS, Glasgow coma scale; BT, body temperature; ORIF, open reduction and internal fixation; AIS, Abbreviated Injury Scale; Ext, extremities; SCI, spinal cord injury; ISS, injury severity scale; RTS, revised trauma score; TRISS, trauma and injury severity score; ps, probability of survival; LOS, length of stay.
Characteristics of t-SCI by age
Histograms in Figure 2 show the age distribution of patients for each t-SCI region. Cervical-SCI incidence was the highest in older people, at all severity levels, and involved a high incidence of relatively low-energy trauma, including falls on base-level ground and falls from stairs (Table 1). In addition, cervical-SCI showed a low incidence among younger patients. Thoracic-SCI incidence was distributed evenly among both young and older patients, regardless of severity. The most common injury mechanism for thoracic-SCI was fall from a height (34.8%, n = 280). Severe lumbar-SCI tended to affect younger patients more frequently, and 54.1% (n = 362) of patients were injured by falling from a height, which was similar to that for thoracic-SCI in that a high-energy injury mechanism was more commonly involved. The characteristics of all analyzed neurotrauma patients were evaluated within the lower age quartile (age <38 years) and the upper age quartile (age >75 years) (Supplementary Table S2, Supplementary Table S3). In the lower age quartile, the incidence of concomitant t-SCI and traumatic TBI was 1.6% (357/22,848). This group predominantly experienced high-energy trauma mechanisms and tended to have torso trauma. Contrastingly, in the upper age quartile, the incidence of concomitant t-SCI and TBI was higher at 3.1% (687/22,418). The mechanisms of injury in this group were more often low energy, such as falls on level ground or from stairs, compared with the younger group.
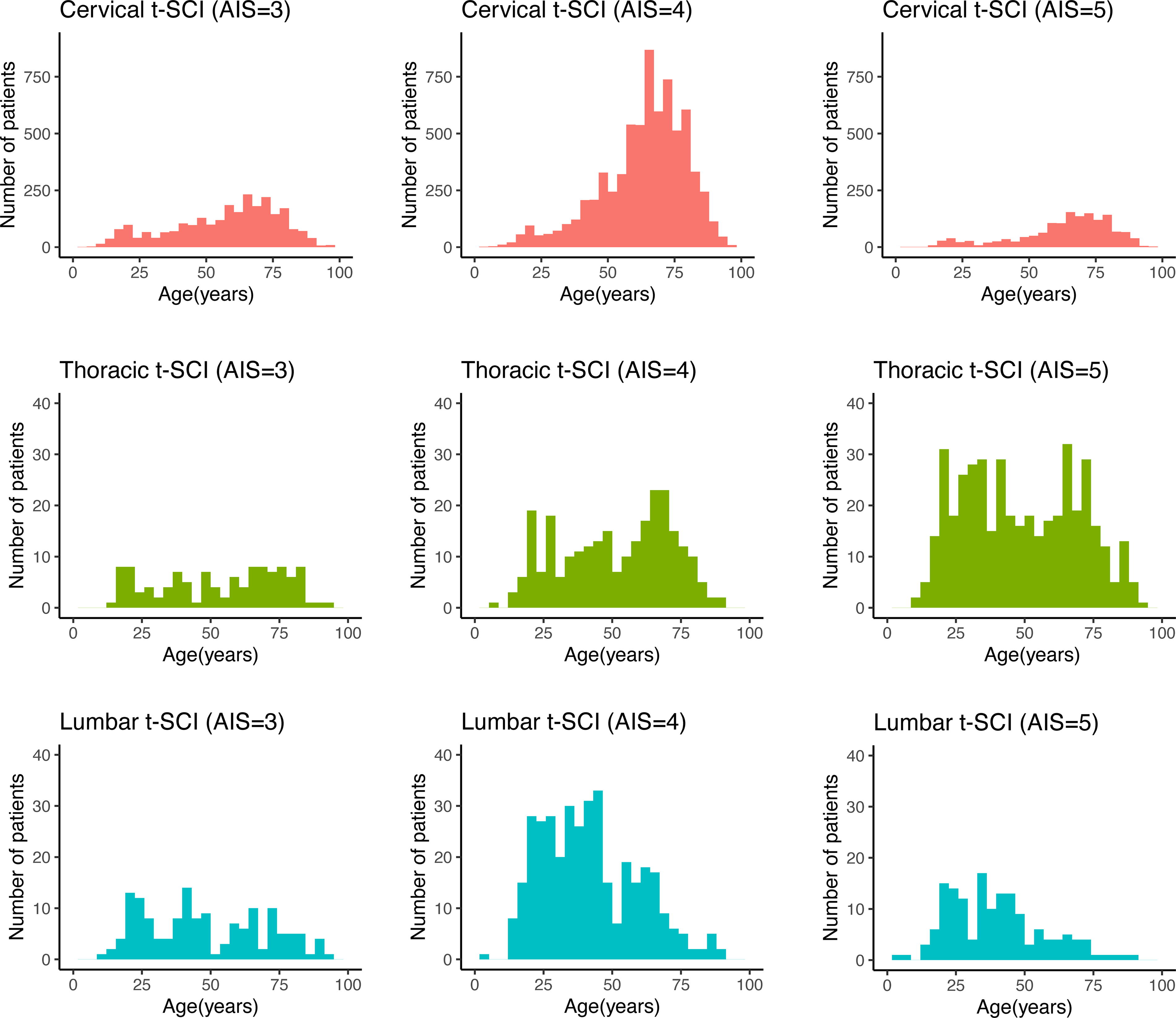
Age distribution by traumatic spinal cord injury category. Patient age distribution by dividing t-SCI into cervical, thoracic, and lumbar spinal cord subgroups. The X-axis indicates age, and the Y-axis indicates the number of patients. t-SCI, traumatic spinal cord injury; TBI, traumatic brain injury.
Association between spinal fracture and SCI
Despite the presence of SCI, no associated spinal fractures were identified in 84.2% (n = 9,237) of the cervical-SCI, 53.1% (n = 427) of the thoracic-SCI, and 59.3% (n = 397) of the lumbar-SCI cases. In this population, patients with spinal fractures but no SCI included those with cervical (3,846/5,188; 74%), thoracic (3,394/4,216; 81%), and lumbar fractures (5,212/5,913; 88%) (Table 1).
Rate of concomitant craniospinal trauma
The distribution of isolated TBI, isolated t-SCI, and concomitant craniospinal injury was visualized using a Venn diagram (Fig. 3). Among all patients, 79,439 (86.4%) included isolated TBI cases, 9,590 (10.4%) included isolated t-SCI cases, and 2,954 (3.2%) included concomitant t-SCI+TBI cases.
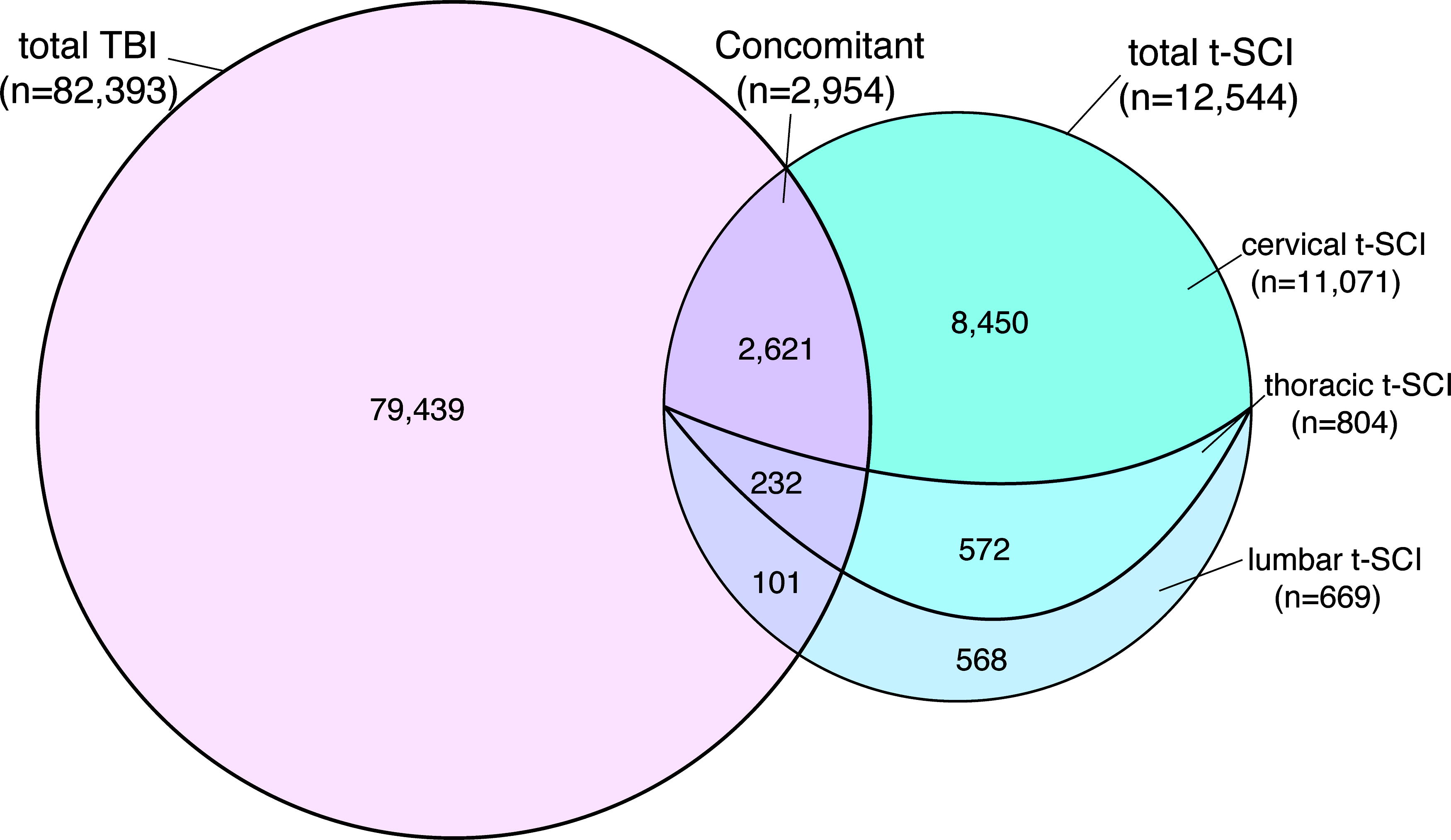
Components of t-SCI and TBI shown in a Venn diagram. t-SCI, traumatic spinal cord injury; TBI, traumatic brain injury.
Of all t-SCI cases, 23.5% (2,954/12,544) included TBI, and 3.6% (2,954/82,393) of all TBI cases included t-SCI. Among concomitant t-SCI+TBI cases, 2,405 (81.4%) included mild TBI (GCS score: 13–15), 243 (8.2%) included moderate TBI (GCS score: 9–12), and 306 (10.5%) included severe TBI (GCS score ≤ 8) (Fig. 4). Furthermore, the distribution of TBI cases was visualized using an alluvial plot, showing that the majority of concomitant injuries occurred with mild TBI (Fig. 5). In addition, the more severe the TBI, the less frequently t-SCI occurred, and most TBI-related deaths involved few t-SCI cases. In the acute phase, among all TBI patients, 4.8% (3,917/82,393) died within 48 h due to severe TBI, and only 0.8% (32/3,917) of these cases also had concomitant t-SCI.
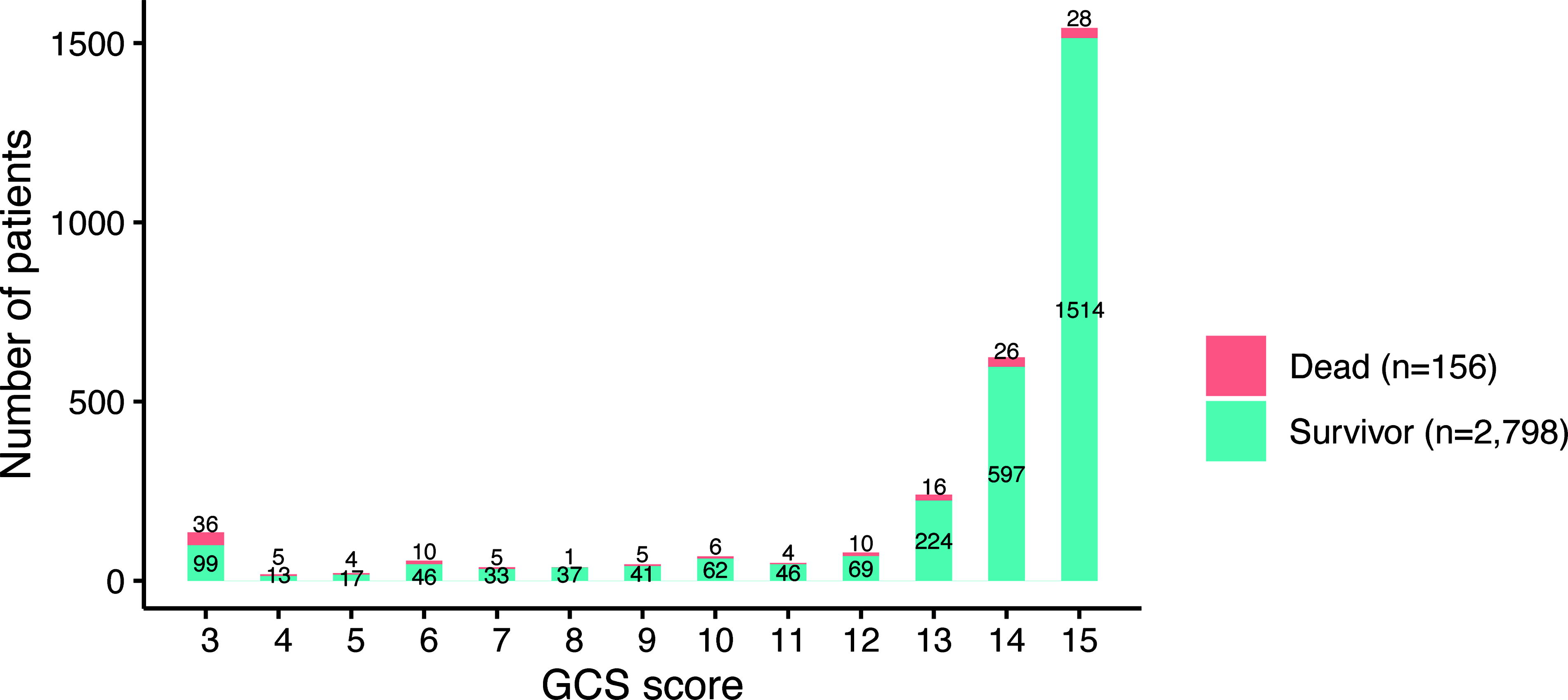
Distribution of GCS score on hospital arrival in patients with concomitant TBI and t-SCI. Distribution of GCS score. The X-axis indicates GCS score, and the Y-axis indicates the number of patients. t-SCI, traumatic spinal cord injury; GCS, Glasgow Coma Scale.
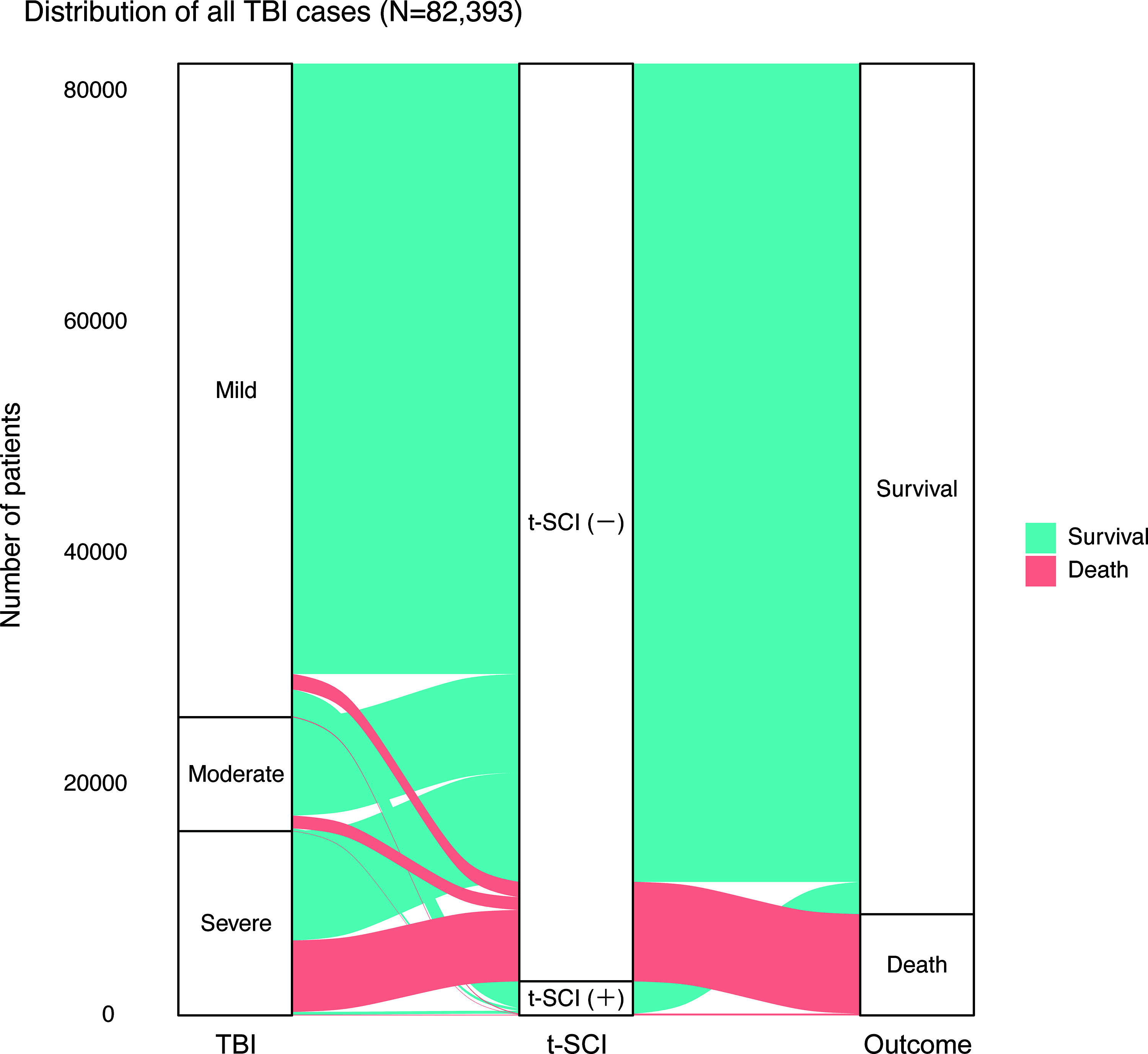
Distribution of all patients with TBI using an alluvial plot. The distribution of all TBI patients (n = 82,393) using an alluvial plot is shown, with the width of the bands representing the number of patients. The green band represents survivors, whereas the pink band indicates deceased individuals. The majority of cases with concomitant t-SCI and TBI were mild TBI. TBI-related deaths were predominantly found in severe TBI cases without t-SCI. TBI, traumatic brain injury; t-SCI, traumatic spinal cord injury.
Among all cervical-SCI cases, 23.7% (2,621/11,071) included concomitant TBI, and 3.3% (2,621/79,439) of all TBI cases included concomitant cervical-SCI.
Impact of concomitant trauma on surgical treatment
Table 2 presents the patient characteristics of the concomitant t-SCI+TBI cases. The median age of these patients was 65 years, and 79.4% of the patients were men. The most common injury mechanisms were falls from stairs (27.9% [n = 824]) and heights (15.9% [n = 470]). The median GCS score was 15 (IQR: 13–15), the median ISS was 18 (IQR: 17–26), and the median TRISS Ps was 0.94 (0.85–0.96). The in-hospital mortality rate was 5.3% (n = 156), and the median duration of hospital stay was 23 days (IQR: 8–45 days). In total, 18.8% (1,806/9,590) of the patients with t-SCI without TBI and 17.4% (513/2,954) of the patients with concomitant t-SCI+TBI underwent spinal surgery. In contrast, craniotomies were performed in 13.3% (10,528/79,439) of TBI cases without t-SCI and in 1.7% (51/2,954) of concomitant t-SCI+TBI cases.
Demographics and Characteristics of Trauma Patients with Concomitant TBI and t-SCI
TBI, traumatic brain injury; t-SCI, traumatic spinal cord injury; IQR, interquartile range; RR, respiratory rate; HR, heart rate; bpm, beats per minute; SBP, systolic blood pressure; GCS, Glasgow coma scale; BT, body temperature; ORIF, open reduction and internal fixation; AIS, Abbreviated Injury Scale; Ext, extremities; SCI, spinal cord injury; ISS, injury severity scale; RTS, revised trauma score; TRISS, trauma and injury severity score; ps, probability of survival; LOS, length of stay.
Factors associated with in-hospital mortality for t-SCI
The in-hospital mortality rates for t-SCI without TBI, TBI without t-SCI, and concomitant t-SCI+TBI were 2.6% (253/9,590), 10.8% (8,609/79,439), and 5.3% (156/2,954), respectively. Multivariate logistic regression analysis results for factors influencing in-hospital mortality in patients with t-SCI (including those with concomitant TBI) are summarized in Table 3. The VIF for multicollinearity was less than 7.0, indicating no multicollinearity in the model. 28 A total of 12 parameters were identified as significantly and independently associated with in-hospital mortality as follows: age; sex; total number of comorbidities; SBP at presentation; GCS score at presentation; and AIS scores for head, face, chest, abdomen, cervical-SCI, thoracic-SCI, and lumbar-SCI. The AOR for in-hospital mortality of cervical-SCI × head AIS interaction was 0.85 (95% CI: 0.77–0.95), indicating a negative interaction. Compared with no cervical-SCI or TBI as a reference, the AOR for in-hospital mortality of cervical-SCI without TBI was 2.34 and that of TBI without cervical-SCI was 1.19, but that of concomitant cervical-SCI+TBI was 2.34 × 1.19 × 0.85, which included the AOR for the interaction term. In addition, the AOR of the interaction term for cervical-SCI × head AIS was 0.87 (95% CI: 0.84–0.90) in the multivariate logistic regression analysis, with in-hospital death as an outcome in TBI cases (Supplementary Table S4). Figure 6 shows how the effect of cervical-SCI AIS severity on in-hospital mortality was affected by head AIS, with a higher severity of cervical-SCI tending to reduce the difference in in-hospital mortality between patients with less and more severe TBI. The GCS score affected the impact of cervical-SCI AIS severity on in-hospital mortality, with a higher severity of cervical-SCI tending to reduce the difference in in-hospital mortality between patients with lower and higher GCS scores (Fig. 7).
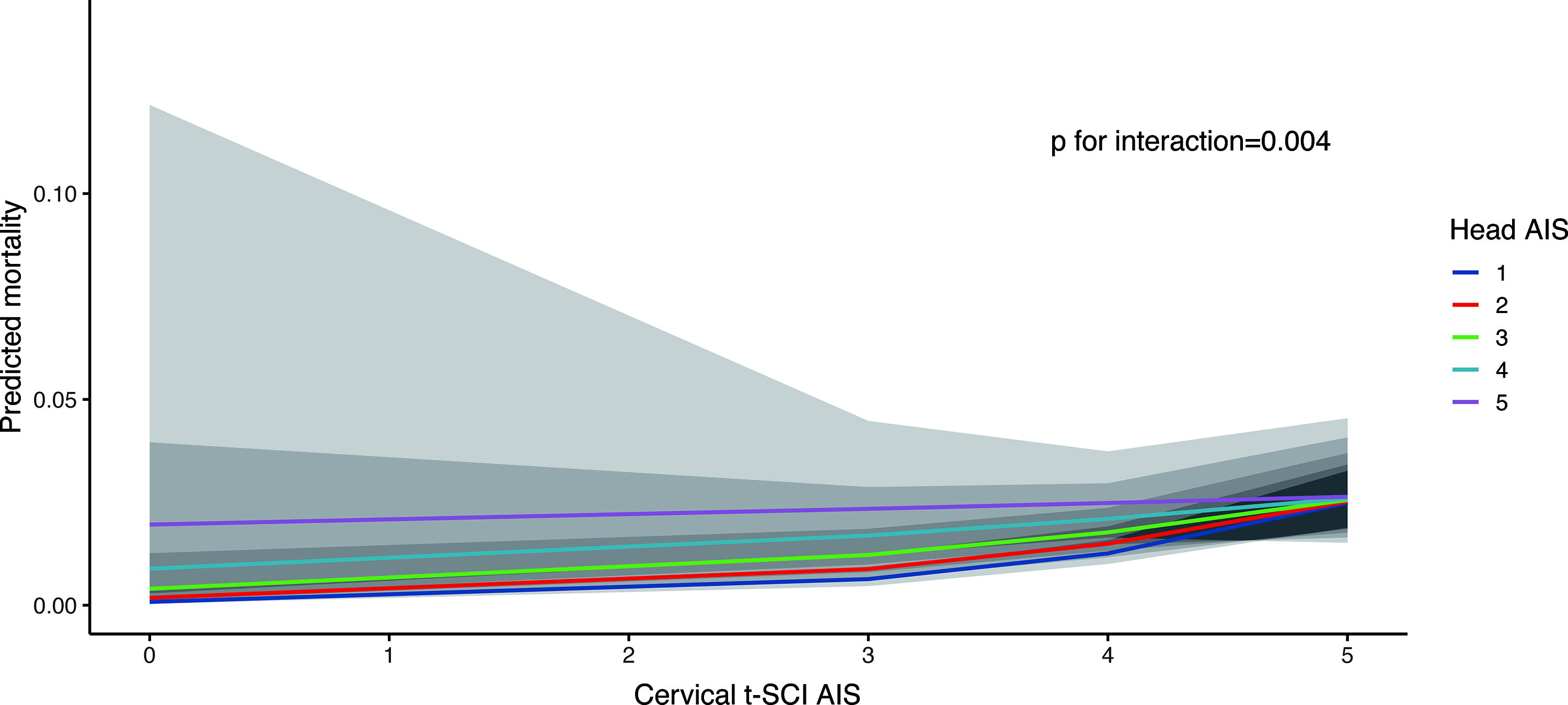
Effect modification of association between cervical-SCI and in-hospital mortality by TBI. The values used in the logistic regression model are as follows: age = 61 years, sex = male, total number of comorbidities = 0, arrival respiratory rate = 20, arrival systolic blood pressure = 139 mmHg, arrival heart rate = 85 beats/min, arrival Glasgow coma scale score = 14, face AIS score = 0, cervical AIS score = 0, chest AIS score = 0, abdominal AIS score = 0, upper extremity AIS score = 0, lower extremity AIS score = 0, thoracic SCI AIS score = 0, lumbar SCI AIS score = 0, cervical spine AIS score = 0, thoracic spine AIS score = 0, and lumbar spine AIS score = 0. SCI, spinal cord injury; TBI, traumatic brain injury; AIS, Abbreviated Injury Scale.
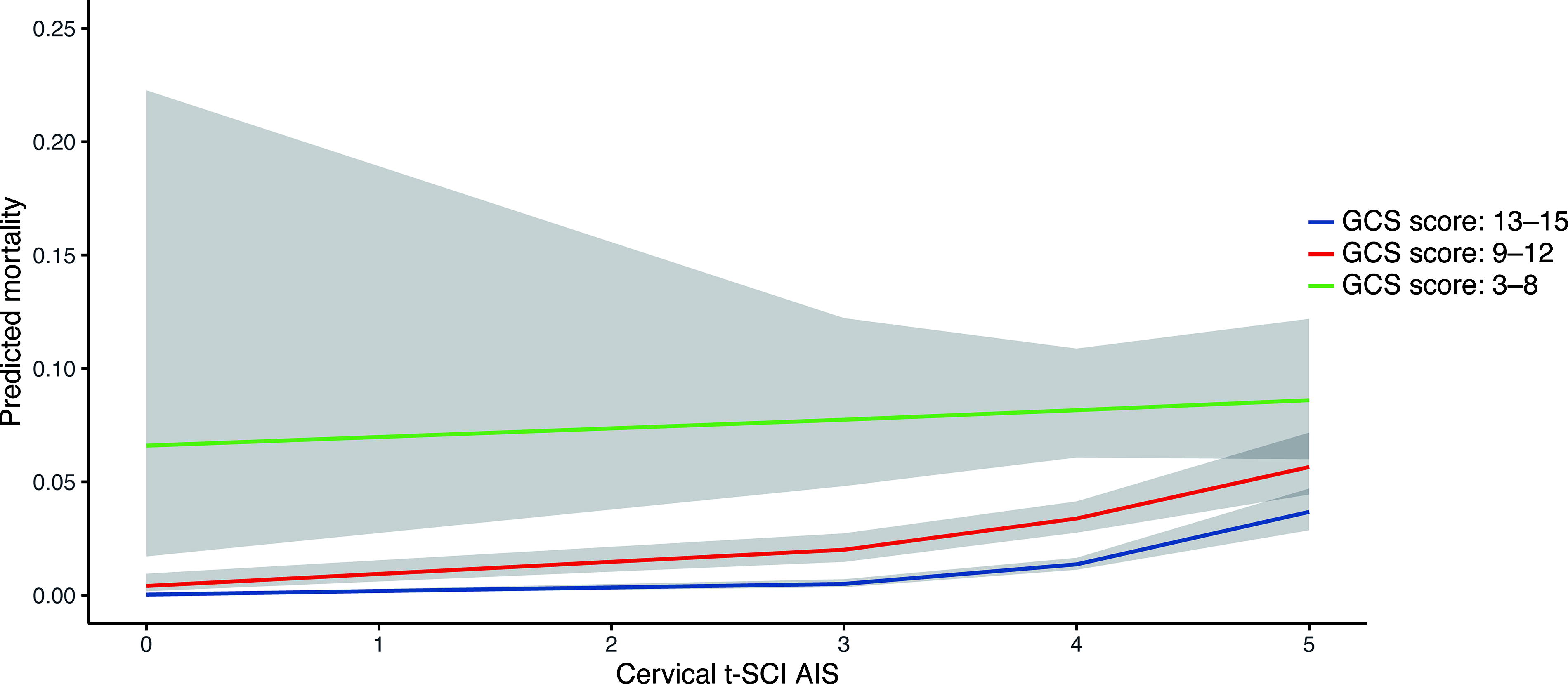
Effect modification by GCS on the association between cervical t-SCI and in-hospital mortality. The following values were used in the logistic regression model: age = 64 years, sex = male, total number of comorbidities = 1, arrival respiratory rate = 20, arrival systolic blood pressure = 131 mmHg, arrival heart rate = 75 beats/min, head AIS score = 0, face AIS score = 0, cervical AIS score = 0, chest AIS score = 0, abdominal AIS score = 0, upper extremity AIS score = 0, lower extremity AIS score = 0, thoracic-SCI AIS score = 0, lumbar SCI AIS score = 0, cervical spine AIS score = 0, thoracic spine AIS score = 0, and lumbar spine AIS score = 0. t-SCI, traumatic spinal cord injury; AIS, Abbreviated Injury Scale.
Multivariate Logistic Regression Analysis with in-Hospital Mortality as the Objective Variable (in t-SCI Cases)
t-SCI, traumatic spinal cord injury; OR, odds ratio; CI, confidence interval; RR, respiratory rate; HR, heart rate; bpm, beats per minute; SBP, systolic blood pressure; GCS, Glasgow coma scale; AIS, Abbreviated Injury Scale; Ext, extremities; SCI, spinal cord injury.
Discussion
This National Trauma Database study presented the epidemiological characteristics of cases of concomitant t-SCI+TBI versus those of isolated t-SCI, including age distribution, injury history, and treatment, in Japan. Furthermore, concomitant t-SCI+TBI was associated with increased in-hospital mortality (AOR: 1.19, 95% CI: 1.09–1.29) compared with that observed for isolated t-SCI. We identified a negative interaction between cervical and head AIS.
The present study has several advantages over previous studies. First, it spanned a 13-year period and analyzed a large dataset. Second, it evaluated the risk factors associated with in-hospital mortality in cases of concomitant t-SCI+TBI by considering the interactions of these conditions. Previously, age, sex, GCS score at presentation, hypotension, bradycardia, and severe TBI have been associated with in-hospital mortality of patients with t-SCI. 26,30 We identified some common risk factors in a model that accounted for interactions between TBI and t-SCI. Furthermore, comorbidities and the presence of severe torso trauma were identified as independent risk factors for in-hospital mortality of these cases in the present study.
Interestingly, the negative interaction between cervical and head AIS for in-hospital mortality was unexpected. Pathophysiologically, the more severe the trauma, the higher the mortality rate. Our study cohort’s distribution of TBI cases showed that most concomitant injuries occurred with mild TBI, and the incidence of t-SCI decreased as the severity of TBI increased, with many TBI patients having no concomitant t-SCI. Although 3.2% of the entire study population had concomitant t-SCI and TBI, this proportion of concomitant injury is lower in severe TBI, supporting the potential underestimation of t-SCI in severe TBI. This underestimation might be due to the trauma diagnosis process. In cases of multiple trauma, CT scans are used to identify injury sites. If a spinal fracture is present, it is easy to consider the possibility of t-SCI. However, when accompanied by impaired consciousness, diagnosing t-SCI based solely on neurological findings becomes difficult. MRI is a definitive tool for diagnosing t-SCI, but if the patient’s overall condition is unstable, performing an MRI may pose a risk to the patient. In clinical settings, spinal MRIs are performed after the patient’s condition stabilizes. 31 For these clinically relevant reasons, we hypothesized that patients with severe TBI and impaired consciousness are less likely to be diagnosed with t-SCI, and thus, its presence is underestimated, leading to lower predicted mortality (with a negative interaction) when more severe t-SCI occurs concomitantly with TBI. This phenomenon is not unique to our cohort but is considered to be a general occurrence in the clinical diagnostic process that could also arise in other trauma cohorts. This finding indicates the importance of considering the possibility of underlying t-SCI in patients with severe TBI and also considering such interactions, which may influence outcomes in clinical research on neurotrauma.
Third, our epidemiological evaluation revealed characteristics, such as the age distribution, injury mechanism, and treatment, of cases of t-SCI compared with those of concomitant t-SCI+TBI cases. In our cohort, the distribution of cervical-SCI was unimodal, with a peak among older people, similar to the epidemiological data from countries with aging populations. 5,32 Contrastingly, thoracic- and lumbar-SCI was characterized by a greater distribution among young people, particularly in the context of crashes from heights and motorcycle accidents. In a previous study, 14 the prevalence of concomitant cervical-SCI in patients with TBI was 6.5% (present study: 3.2%), that of concomitant all t-SCI in patients with TBI was 12.4–12.5% (present study: 3.6%), that of concomitant TBI in patients with cervical-SCI was 40.4% (present study: 23.7%), and that of TBI in patients with all t-SCI was 32.5% (present study: 23.5%). The lower rates in this study may be due to differences in the selected patient populations, which included patients with mild TBI in this study. Concomitant injuries may also have been omitted from the registry data because they did not affect the ISS calculation, as described below.
Finally, our results may be generalizable to other settings. As the JTDB includes many hospitals in Japan, serving metropolitan, urban, and rural areas, and as our results are consistent with those in other settings, such as the TraumaRegister DGU®, 33 our findings may be applicable to different regions and hospitals, both inside and outside Japan.
However, this study also has some limitations. First, as a retrospective analysis utilizing secondary registry data, this study has inherent limitations characteristic of such research designs. Notably, some data elements, such as the American Spinal Injury Association Impairment Scale, timing of surgical interventions, patient frailty index, 34 and ADLs (activities of daily living) after discharge, were not accessible. Furthermore, the exclusion of patients due to missing data (such as age, sex, GCS score upon presentation, or outcomes) may have introduced selection bias. Nevertheless, imputation of these missing values was not pursued as they represent critical variables for the analysis, and the assumption of random missingness could not be assumed. Second, the baseline characteristics differed among the subgroups defined by the injury mode. To address any imbalance associated with such observational research, we performed multivariate analyses; however, multiple unmeasured variables may underlie differences in outcomes, making it difficult to eliminate the influence of observed confounding factors completely. Finally, t-SCI diagnosis may have been underestimated; for example, concomitant SCI may have gone undetected in patients with very severe TBI and a high proportionate risk of death within 48 h. However, this hypothesis cannot be proven unless a prospective observational study is conducted to verify the presence of spinal injuries in the acute phase of severe traumatic brain injury. In addition, the highest AIS in the head and neck region is used to calculate the ISS. Therefore, it is possible that the input for the less severe of the concomitant injuries, either t-SCI or TBI, might be omitted due to it not affecting the ISS calculation.
Conclusions
We evaluated epidemiological characteristics concerning concomitant t-SCI+TBI. Nearly one-quarter of all patients with t-SCI also experienced TBI. Such concomitant injury doubled the in-hospital mortality rate, relative to that of isolated t-SCI. TBI also increased in-hospital mortality relative to t-SCI. Age; sex; total number of comorbidities; SBP at presentation; GCS score at presentation; and AIS scores for head, face, chest, abdomen, cervical-SCI, thoracic-SCI, and lumbar-SCI were associated with in-hospital mortality in patients with t-SCI. We further found an unexpected negative interaction between cervical t-SCI and TBI with a higher severity of cervical-SCI, leading to a reduction in in-hospital mortality between patients with less and more severe TBI cases, suggesting that the occurrence of t-SCI is underestimated in patients with TBI. This research underscores the importance of considering the possibility of concomitant t-SCI in patients with TBI.
Transparency, Rigor, and Reproducibility Summary
As this is a secondary retrospective analysis of the Japan Trauma Data Bank (JTDB) registry data, no preregistration was conducted. The analysis plan was not formally preregistered. Due to the lack of similar previous studies and the inclusion of interactions, all available data were used, and no sample size calculations were made. The JTDB data used in this study are available to researchers in Japan and have been approved by the Japanese Society of Traumatology. Data sharing is not allowed for overseas researchers, as the purpose of the JTDB is to improve trauma care in Japan. This article will be published under a Creative Commons Open Access license and upon publication will be freely available at https://www.liebertpub.com/loi/neu.
Footnotes
Acknowledgments
The authors thank the emergency medical service personnel, nurses, and emergency physicians who participated in the JTDB and the patients who contributed to the success of this study.
Authors’ Contributions
J.T. conceived and designed this study; contributed to the acquisition, analysis, and interpretation of the data; and was responsible for the drafting, editing, and submission of the article. A.K.D. was involved in the conceptualization of this study and contributed significantly to the data analysis, interpretation of the results, and article preparation. W.P. provided his professional opinions on spinal surgery and research on TBI and contributed to the overall research and interpretation of the results. Y.K., K.T., and T.K. performed data extraction and analysis and assisted in the preparation of the article. S.N. and K.K. played a significant role in data analysis and helped to draft the article. T.H., Y.U., T.K., M.O., and K.I. provided advice on the statistical analysis and article preparation. J.O. provided significant inputs for data interpretation and critical appraisal of the article. All authors contributed to the acquisition of data and reviewed, discussed, and approved the final article. J.T. has full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
The authors declare that they have no sources of funding to report.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.