
Abstract
Patients with traumatic brain injury (TBI) are severely injured patients who require timely, efficient, and specialized care. The effectiveness of helicopter emergency medical services (HEMS) for patients with TBI remains unclear. This study aimed to compare the mortality of patients with TBI transported by HEMS and ground ambulance using propensity score-matching analysis, and to analyze the effects of HEMS in various subpopulations. We conducted a retrospective analysis of the Japan Trauma Data Bank. The study period was from January 2004 to December 2018. The participants were divided into two groups: the helicopter group (patients transported by HEMS) and ground group (patients transported by ground ambulance). The principal outcome was death at hospital discharge. In total, 58,532 patients were eligible for analysis (ground group, n = 54,820 [93.7%]; helicopter group, n = 3712 [6.3%]). Helicopter transport decreased patient mortality at hospital discharge (adjusted odds ratio [OR], 0.83; 95% confidence interval [CI], 0.74–0.92). In propensity score-matched patients, the proportion of deaths at hospital discharge was lower in the helicopter (18.76%) than in the ground (21.21%) group (crude OR, 0.86; 95% CI, 0.77–0.96). The mortality rate in the helicopter group was significantly reduced in many subpopulations, especially in cases of severe TBI with a decreased level of consciousness or higher Injury Severity Score (ISS; Japan Coma Scale score 2 [adjusted OR, 0.60; 95% CI, 0.45–0.80] and ISS ≥50 [adjusted OR, 0.69; 95% CI, 0.48–0.99]). Although the study design was non-randomized, our findings in patients with TBI showed that HEMS conferred a mortality benefit over ground ambulance.
Introduction
Traumatic brain injury (TBI) contributes to a substantial number of deaths and permanent disabilities worldwide. 1,2 Significant improvements in the survival of patients with TBI have been achieved through the widespread use of evidence-based guidelines, centralization of care, and advances in neurocritical care. 3 The survival rate considerably increases when care is delivered within the “golden hour.” Factors that allow patients to benefit from the aforementioned developments include improvements in emergency medical services (EMS) and timely transport to specialized trauma centers capable of providing life-saving interventions.
The use of helicopter EMS (HEMS) to transport and treat trauma patients is common in most industrialized nations. Reduced rescue times and increased catchment areas are among the presumable specific advantages of HEMS. However, HEMS availability depends on the weather, time of day, and controlled visual flight rules and comes with a high economic burden. 4 Therefore, recent research has questioned which patients with trauma derive the greatest benefit from such a limited and resource-intensive modality. 4 -6 Patients with minor injuries may not be appropriate candidates for HEMS because the scope for improved outcomes may be limited and the cost is high. 4 -6 Several studies 7,8 have attempted to answer this question; however, only few of them have focused on patients with TBI. Patients with isolated TBI and TBI with injury to other regions need to be examined independently of those with other major trauma, as they are in particular need of expedited transport to trauma centers where specialized neurosurgical and neurocritical care can be provided.
HEMS in Japan provides a rapid transport of victims and a doctor delivery system to initiate treatment for critically ill patients as soon as possible. 9 Therefore, in this study, we examined whether HEMS would be associated with reduced mortality compared with ground EMS (GEMS) in patients with TBI and determined those patients who were most likely to benefit from HEMS to refine on-scene triage and transport guidelines.
Methods
Study design, population, and setting
This was a nationwide retrospective cohort study conducted using the Japan Trauma Data Bank (JTDB). We included patients registered in the JTDB from January 2004 to December 2018 and those with TBI who were transported to a JTDB-participating hospital. TBI was defined using the Abbreviated Injury Scale (AIS) code. 10 We classified patients with TBI according to the head AIS code: 3 (serious), 4 (severe), and 5 (critical). The patients were stratified according to the type of transportation from the accident scene to the hospital (HEMS/GEMS). Those transported by physician-operated ambulances were excluded from this study. There is no other mechanism of transport that started to be used in the study period. We excluded patients who were in cardiopulmonary arrest at the scene, received cardiopulmonary resuscitation at the scene (because of severe trauma), required interhospital transport, or were burn victims (because burns differ from other traumas). 7 -9,11 Patients with cardiopulmonary arrest were defined as those having a systolic blood pressure of 0 mmHg and/or heart rate of 0 bpm on or before hospital arrival. 12 We excluded patients with missing outcome data or variables required for propensity score (PS) matching.
Japan Trauma Data Bank
The JTDB, launched in 2003 by the Japanese Association for the Surgery of Trauma (Trauma Surgery Committee) and Japanese Association for Acute Medicine (Committee for Clinical Care Evaluation), is similar to the trauma databases in North America, Europe, and Oceania. 12,13 In 2018, 272 major emergency medical institutions across Japan were registered in the JTDB. 13 The included hospitals had service levels similar to those of level I trauma centers in the United States. Data were collected via the internet from the participating institutions. The primary data inputs were from physicians and medical assistants who attended an AIS coding course. 12,13 The JTDB records trauma patient data, including age, sex, mechanism of injury, AIS code (1998 version), Injury Severity Score (ISS), vital signs at the scene, date and time series from hospital arrival to discharge, medical procedures (interventional radiology, surgery, and computed tomography), complications, and mortality at hospital discharge. 13 Patients transported to the JTDB-participating hospitals were treated based on the guidelines for managing severe TBI. 14 To reduce traumatic deaths caused by motor vehicle collisions, the Japanese Road Traffic Act was revised in June 2002, imposing severe fines for traffic offenses; since then, fatal collisions caused by drunk drivers decreased. The law also requires children age <6 years to use child seats. 14 There have been no major breakthroughs in the treatment of severe TBI in the past 15 years. 14 The level of consciousness was evaluated using the Japan Coma Scale (JCS) score, which was recorded at the scene, mainly by EMS personnel, for all patients. The JCS score correlates well with the Glasgow Coma Scale; a neurological dysfunction score of 100 points on the JCS is equivalent to 6–9 on the Glasgow Coma Scale. 8 Patients were categorized into four groups based on the JCS score: 0 (Grade 0, alert), 1–3 (Grade 1, delirium), 10–30 (Grade 2, somnolence), and 100–300 (Grade 3, coma).
Ground emergency medical services
GEMS in Japan comprise emergency medical technicians or paramedics trained in advanced life support and pre-hospital trauma life support and firefighters trained in basic life support. The members of the GEMS team are allowed to perform several procedures according to fixed protocols set by the Ministry of Health, Labor, and Welfare, including venous cannulation, crystalloid infusion, early defibrillation, and endotracheal intubation without muscle relaxants for cardiopulmonary arrest. 15 In addition, for trauma cases, the members of the GEMS team have been permitted to administer intravenous drip injections exclusively for patients in a state of shock from 2014. Moreover, they were allowed to administer oxygen or to perform suctioning, the jaw-thrust maneuver, or manual ventilation using a bag-valve-mask for airway management. 16
Helicopter emergency medical services
In Japan, HEMS were first introduced in 2000 and have since spread across many regions. As of May 2021, 54 HEMS have been deployed in 45 prefectures across Japan. 9 In 2018, 29,055 helicopter transfers were recorded, and the number is gradually increasing annually. 9 HEMS operate only during the daytime. The Japanese HEMS are similar to those of European countries and, in most cases, employ a physician-based pre-hospital approach to emergency patients. 8,9
One or two physicians and a nurse are transported to the scene by a helicopter. Most physicians are board-certified in specific fields (acute care, surgery, anesthesiology, or aeromedical services) and have received advanced trauma life support training. 8,9 National and prefectural governments pay the operational charges. 9 In the Japanese emergency system, HEMS cannot be requested directly by patients. The fire department dispatch center that receives the 119 calls determines the necessity of dispatching HEMS. HEMS are based at a tertiary-level emergency hospital and are dispatched according to the information provided during the emergency call from the fire department. GEMS can also request HEMS dispatch based on the results of patient assessment at the scene. In such cases, the GEMS team first rescue the injured patient and subsequently transport them to a location where the HEMS can land safely (the “rendezvous point”). 8,9
Then, the HEMS team provides emergency care, such as endotracheal intubation, chest tube drainage, emergency tracheotomy, or thoracotomy with aortic clamping in the ambulance using various medications. This system is called the “rendezvous system.” After emergency care, the HEMS transport the patient to a tertiary care hospital. 8,9 In this study, a patient using the rendezvous system was reported to be transported by HEMS only if he/she had arrived at the hospital by helicopter.
Study outcomes
The primary outcome was mortality at hospital discharge. The secondary outcomes included surgery for increased intracranial pressure (ICP) and cognitive dysfunction (diagnosed by an in-hospital medical team). Cognitive dysfunction after TBI is defined in the Guidelines for the Management of Severe Head Injury (4th edition) as “impairment in numerous cognitive domains, including executive function, learning and memory, attention and processing speed, among others.” 14
Propensity score matching
We performed a PS-matched analysis because HEMS dispatch was not randomly assigned. Logistic regression analysis was used to estimate the PS for the prediction of transport using the available variables. Confounders were carefully evaluated based on previous reports, 7,8,17 and clinically important confounders were included to estimate the PS. 9 The PS (i.e., the probability of receiving HEMS) for each patient was calculated using multi-variable logistic regression analysis based on the following variables: age (continuous), sex (male/female), year of onset (2004–2006, 2007–2009, 2010–2012, 2013–2015, or 2016–2018), hospital arrival time (daytime (from 8 a.m. to 6 p.m.)/nighttime), JCS score at the scene (Grade 0–3), heart rate at the scene (continuous), systolic blood pressure at the scene (continuous), type of injury (blunt/non-blunt), cause of trauma (motor vehicle accident/fall/others), other severe extracranial injuries (AIS score ≥3) (no/yes), and ISS (continuous).
We performed an area under the receiver operating characteristic curve analysis to predict HEMS use in patients with TBI. One-to-one pair matching between the helicopter and ground groups was performed using nearest-neighbor matching without replacement and a caliper width of 0.02 as the standard deviation (SD) of the PS. Covariate balances before and after matching were assessed by comparing the standardized mean differences (< 10% was considered a negligible imbalance between the groups). In the PS-matched cohort, univariable logistic regression analysis was conducted to assess the association between HEMS use and mortality.
Statistical analysis
Patients were divided into two groups (helicopter and ground). Descriptive data are presented as counts and percentages (categorical variables) or means ± SD (continuous variables for patient background) and medians and interquartile ranges (continuous variables for time). We also assessed the patient background and proportion of surgeries performed for TBI in both groups. The trends across the 3-year periods (2004–2006, 2007–2009, 2010–2012, 2013–2015, and 2016–2018) were assessed using linear trend tests. Outcomes were evaluated using univariable and multi-variable logistic regression analyses for all cohorts to assess the robustness of the results. Based on these analyses, we calculated the odds ratios (ORs) and 95% confidence intervals (CIs).
In the multi-variable logistic regression model, we adjusted for the following variables: age (10-year strata), sex (male/female), year of onset (2004–2006, 2007–2009, 2010–2012, 2013–2015, or 2016–2018), hospital arrival time (daytime/nighttime), JCS score at the scene (Grade 0–3), heart rate at the scene (continuous), systolic blood pressure at the scene (continuous), type of injury (blunt/non-blunt), cause of trauma (motor vehicle accident/fall/others), other severe extracranial injuries (AIS score ≥3) (no/yes), and ISS (continuous) used in the PS calculation, based on previous reports. 7 -9, 17 Subgroup analyses were performed to identify helicopter transport's potential benefits and drawbacks. In each subgroup, multi-variable logistic regression analysis, with adjustment for the aforementioned variables, was performed to assess the independent effect of helicopter use on mortality at hospital discharge. The Wilcoxon rank-sum test was employed to compare the time from dispatch to ED arrival and time from ED arrival to computed tomography scan or surgery. Statistical significance was defined by a two-sided p value < 0.05 or assessed using a 95% CI in all statistical analyses. All statistical analyses were conducted using STATA (version 16; StataCorp LP, College Station, TX).
Ethics approval
This article was written based on the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement for the reporting of cohort and cross-sectional studies. 18 The study design was approved by the Ethics Committee of Osaka University Graduate School of Medicine (approval number: 16260). The requirement for written informed consent was waived owing to the retrospective nature of the study. Personal identifiers are not included in the JTDB records.
Results
A total of 58,532 patients were included, of whom 54,820 (93.7%) were transported by GEMS and 3712 (6.3%) by HEMS (Fig. 1). The patient characteristics are presented in Table 1. The mean ages of patients in the ground and helicopter groups were 58.71 (23.45) and 58.26 (23.34) years, respectively, and the majority of the patients were male (ground group, n = 37,154/54,820 [67.8%]; helicopter group, n = 2784/3712 [75.0%]; Table 1). The most common type of trauma was blunt trauma in the ground (n = 53,418/54,820 [97.4%]) and helicopter (n = 3665/3712 [98.9%]) groups. The systolic blood pressure at the accident scene was lower in the helicopter (140.08 [33.93] mm Hg) than in the ground group (140.52 [34.70] mm Hg). The proportion of patients with a JCS score of 3 (ground group, n = 14,020/54,820 [25.6%]; helicopter group, n = 1278/3712 [34.4%]) and that of those with multiple trauma (ground group, n = 15,427/54,820 [28.1%]; helicopter group, n = 1857/3712 [50.0%]) were higher in the helicopter than in the ground group. The mean ISS was higher in the helicopter (26.15 [11.84]) than in the ground group (20.98 [9.97]). Differences between the two groups were found for all variables, except for the heart rate at the scene, and the helicopter group included more severe patients than the ground group.
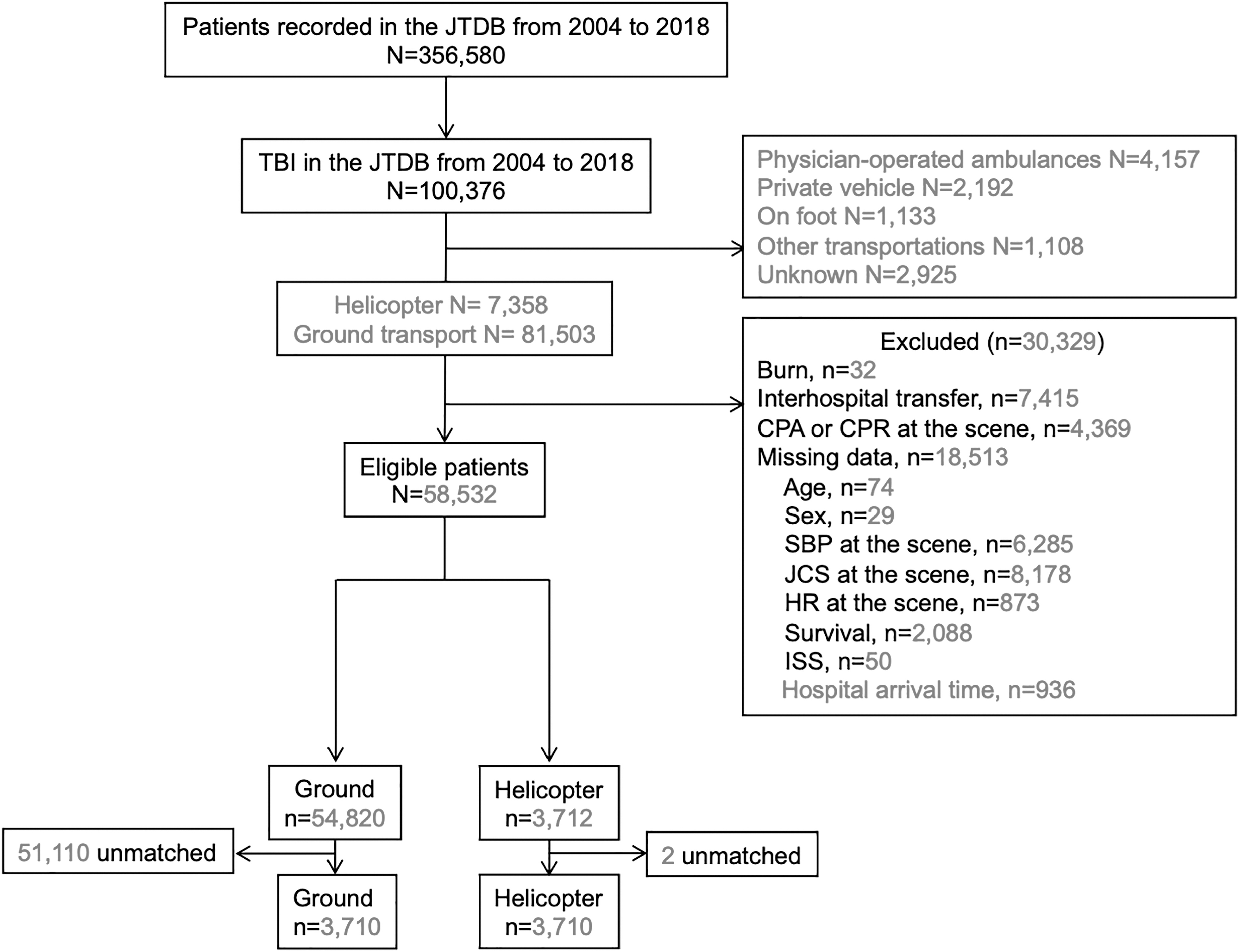
Flow chart of the patients included in this study. JTDB, Japan Trauma Data Bank; TBI, traumatic brain injury; CPA, cardiopulmonary arrest; CPR, cardiopulmonary resuscitation; JCS, Japan Coma Scale; SBP, systolic blood pressure; HR, heart rate; ISS, Injury Severity Score.
Characteristics of Patients with and without Helicopter Transport (All Patients and Propensity Score-Matched Patients)
PS, propensity score; SMD, standardized mean difference; SD, standard deviation; JCS, Japan Coma Scale; BP, blood pressure; HR, heart rate; bpm, beats per minute; ISS, Injury Severity Score; ED, emergency department; IQR, interquartile range; CT, computed tomography.
Although the time from the 119 (Japanese version) call to ED arrival was longer in the helicopter than in the ground group (median, 35 [28–45] vs. 57 [46–71] min), the time from ED arrival to computed tomography scan (median, 28 [20–41] vs. 28 [18–45] min) was similar between the two groups (Table 1). The time from ED arrival to surgery (median, 243 [120–4731] vs. 210.5 [104.5–4594.5] min) was shorter in the HEMS than in the GEMS group (Table 1). During the study period, collision or coma cases decreased over time in both groups. In contrast, the proportion of multiple traumas and surgeries performed in the ground group decreased over time while remaining constant in the helicopter group (Table 2). Table 1 also shows the baseline characteristics of the PS-matched patients. After PS matching, 3712 patients in each group were selected; the area under the receiver operating characteristic curve of the PS was 0.8224. The characteristics of the PS-matched patients were finely balanced with respect to the absolute standardized mean difference.
Temporal Trend in the Patient Background and Proportion of Treatment for TBI during the Study Period
Craterization includes continuous ventricle drainage, intracranial pressure monitors, or burr-hole evacuation.
TBI, traumatic brain injury; IQR, interquartile range; JCS, Japan Coma Scale.
The results of the multi-variable logistic regression analysis and PS matching for the primary outcome are presented in Table 3. The proportion of deaths at hospital discharge was higher in the helicopter (18.75%) than in the ground (13.61%) group (crude OR, 1.46; 95% CI, 1.34–1.60). This finding was reversed in a multi-variable logistic regression model adjusted for measured confounders (adjusted OR, 0.83; 95% CI, 0.74–0.92). In PS-matched patients, the mortality rates at hospital discharge were 21.21% (787/3,710) and 18.76% (696/3,710) in the ground and helicopter groups, respectively. In the PS-matched analysis, HEMS were associated with decreased mortality at hospital discharge (crude OR, 0.86; 95% CI, 0.77–0.96).
Primary and Secondary Outcome Comparisons before and after Propensity Score Matching
OR, odds ratio; CI, confidence interval; ICP, intracranial pressure; PS, propensity score.
Table 3 also shows the results of the multi-variable logistic regression and PS-matched analyses for the secondary outcomes. In PS-matched patients, surgery for increased ICP was less frequent in the helicopter (520/3710 [14.02%]) than in the ground (648/3710 [17.47%]) group (OR, 0.77; 95% CI, 0.68–0.87; Table 3). There was no significant difference in cognitive disorders as complications between the two groups (6.74% [250/3710] vs. 5.9% [221/3712]) (OR, 0.88; 95% CI, 0.73–1.06).
In the subgroup analysis (Fig. 2), the mortality rate in the helicopter group tended to reduce in many subpopulations, especially in severe cases (JCS score 2 [adjusted OR, 0.60; 95% CI, 0.45–0.80] and ISS ≥50 [adjusted OR, 0.69; 95% CI, 0.48–0.99]) compared with the ground group. With regard to the TBI type, HEMS decreased or tended to decrease mortality in almost all types compared with GEMS (Fig. 3).

Subgroup analysis between ground and helicopter groups (all patients). BP, blood pressure; JCS, Japan Coma Scale; HR, heart rate; ISS, Injury Severity Score; OR, odds ratio; CI, confidence interval; N/A, not available.
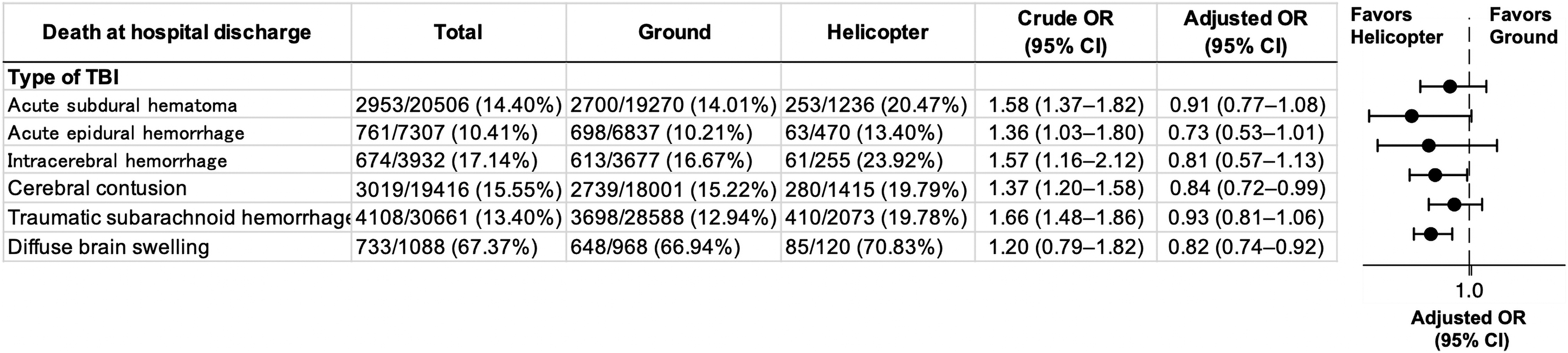
Subgroup analysis based on TBI types between ground and helicopter groups (all patients). TBI, traumatic brain injury, OR, odds ratio, CI, confidence interval.
Discussion
In this retrospective cohort study, we evaluated the effect of HEMS on mortality at hospital discharge in patients with TBI using the nationwide JTDB. Using analyses adjusted for trauma severity, we found that HEMS were significantly associated with decreased mortality at hospital discharge. Subgroup analysis also showed a similar result, especially in cases of severe TBI with a decreased level of consciousness or higher ISS. Our findings, which are based on the largest trauma data bank in Japan, provide sufficient evidence for the use of HEMS in TBI treatment.
The HEMS dispatch system in Japan dispatches HEMS only for critical patients; therefore, the number of patients with high JCS scores on the scene, high ISS scores, and multiple traumas, all of which are indicative of a severe case, were higher in the HEMS than in the GEMS group. The constant trend regarding the proportion of operations in HEMS during the study period highlights the need to properly transport in a severe condition that need to undergo surgery. After adjustment for the severity and nature of injuries, the adjusted OR of mortality was higher in the GEMS than in the HEMS group, not just in the analysis of PS-matched patients alone but also in the multi-variable analysis of the overall cohort.
Our study demonstrated that helicopter transport of patients with TBI was associated with decreased mortality compared with ground transport, which is consistent with the results of a previous study on helicopter transport of patients with TBI to level I/II trauma centers in the United States. 19 HEMS interventions differ significantly between Japan and other countries, particularly the United States. HEMS in Japan are exclusively physician-staffed. The HEMS, typically staffed by experienced emergency care providers, are an integral part of regional trauma systems. 8,9 Thus, the beneficial effect of HEMS in Japan is considered to include a combination of speed, team expertise, timely access to trauma centers for seriously injured patients 20 –23 and the presence of a physician.
Secondary injuries occur within minutes or hours following a primary injury. Although little can be done to reverse the primary brain damage, a secondary brain injury because of exacerbation of cerebral ischemia or hypoxia is potentially preventable. Therefore, pre-hospital care of patients with TBI is critical to prevent secondary brain injury. 24,25 Hypotension, hypoxia, and hypercapnia after TBI have been shown to result in secondary brain injury, leading to increased mortality and disability. 26 Thus, effective pre-hospital assessment and treatment by EMS are vital. 24,25 When ICP increases after TBI, systemic blood pressure rises as a compensatory mechanism to maintain the cerebral perfusion pressure (Cushing reflex). 27,28 In our study population, patients with severe TBI, including those with a decreased level of consciousness or hypertension and bradycardia (representing the Cushing reflex), benefited from HEMS.
The decision to perform a surgery may be affected by many factors, such as the JCS score, each patient's age, type of TBI, computed tomography availability, and the quality of intensive care unit/pre-hospital care. Considering that pre-hospital treatment in GEMS is limited, aggressive treatment, such as airway management or blood pressure control at the scene, would help reduce the need for surgery for increased ICP. These patients required more advanced treatment for stabilization. Patients transported in a physician-staffed helicopter were significantly more likely to be intubated, to require chest thoracostomy tube placement, to receive sedation, or to be treated with vasopressors. 29 A previous study suggested that early stabilization during the pre-hospital stage was associated with a significant reduction in mortality. 30 In this study, it is assumed that HEMS pre-hospital care before definitive treatment was beneficial for reducing mortality and surgery. Therefore, HEMS are a means of transportation and an avenue of treatment.
In our subgroup analysis, insignificant results were found with penetrating TBI and pediatric cases, which may be attributed to the small sample size. However, this finding is consistent with a previous report based on the JTDB, which showed that compared with ground transport, helicopter transport was not associated with reduced mortality in pediatric trauma patients. 17 Therefore, it appears that additional training or equipment is needed in both groups. Therefore, our next step would be to establish evidence for pediatric or penetrating TBI patients through further research.
The time to definitive trauma care strongly influences patient outcomes. 31 Any benefit associated with HEMS would likely be attributed to a reduction in the time from injury to definitive care. However, in this study, the median time from 119 is Japanese version calls to ED arrival was longer in the helicopter than in the ground group. The HEMS team could have performed various procedures at the rendezvous point, resulting in a prolonged preclinical time in patients of the helicopter group. Although the transportation times for HEMS were longer in this study, any benefit noted with HEMS would be logically associated with a decrease in the time from injury to stabilization by helicopter physicians. Therefore, this study does not confirm the efficacy of helicopters in reducing the mortality rate of TBI patients. Rather, it shows that early aggressive intervention, coupled with a sophisticated pre-hospital system that preferentially directs patients to the correct facilities after accurate assessment, may lead to better outcomes.
This study had some limitations. First, the PS-matched analysis carries the risk of residual selection bias. Some differences between the two groups may still exist even after PS matching, particularly if data on important confounding factors were not included in the analysis. In addition, the time interval of 8 a.m. to 6 p.m. excludes a wide variety of brain trauma cases, which could have influenced the outcomes of the study. The PS matching may have excluded many nighttime patients, although the multi-variable analysis covered the entire cohort. As these results were statistically similar, it was thought that they were reasonable. Although mortality after TBI was generally attributed to high ICPs, data on other causes of mortality, such as pneumonia, cardiac arrest, or withdrawal of care, were unavailable in the JTDB. Further, data on clinical symptoms or events, such as pupil size, asymmetry, and reactivity, the use of anti-epileptics, and ICP monitor rates and deterioration, were also unavailable in the JTDB. Second, information on the location of the hospital or transport time before helicopter arrival was not included in the JTDB. In the United States, TBI-related mortality rates are higher in rural areas. 32 Thus, our results may differ if hospital locations were included in the analysis. Compared with other countries, Japan has a smaller land area, and each prefecture is covered by one or more HEMS setups. However, we were unable to determine the influence of regional variabilities in outcomes with HEMS. Moreover, the applicability of this study could be limited in other countries where ground transportation is faster and more reliable than helicopter transportation.
Third, the data in this study primarily involved blunt trauma cases; therefore, the results cannot be extended to penetrating TBI. Further, the incidence of cognitive disorders could have been underestimated in our study as the JTDB includes clinical data until hospital discharge, which means that it focuses mainly on the injury's acute phase. Cognitive symptoms after TBI can be accurately evaluated only after recovering from the altered state of consciousness in the acute phase. Finally, this was an observational study, and other unknown confounding factors possibly exist. Our results could not establish causality and remain limited to associations. The study showed that the “delivery” of a medical professional at the injury site via helicopter can facilitate early initiation of aggressive life-saving care, thus leading to improved outcomes. If these professionals were also effectively delivered by ambulance, the outcomes of ground transportation would have also been improved. Hence, our results should be validated in other cohorts or further randomized trials, including the relative efficacies. Despite these limitations, we presented a large cohort of patients and evaluated preclinical as well as clinical parameters to establish the potential benefits of HEMS compared with GEMS for TBI patients.
In conclusion, the use of the Japanese HEMS for TBI patients was associated with lower mortality rates at hospital discharge.
Footnotes
Acknowledgments
We thank the EMS personnel, nurses, neurosurgeons, and emergency medicine physicians involved in the JTDB. We also thank our colleagues from the Osaka University Center of Medical Data Science, Advanced Clinical Epidemiology Investigator's Research Project, for providing their insight and expertise in this study.
Authors' Contributions
S.H., T. Sobue, and T.K. designed the study and wrote the manuscript. S.H. and T.K. performed the statistical analyses. Y.N., H.O., and T. Shimazu critically revised the manuscript for important intellectual content. All authors have read and approved the final manuscript.
Funding Information
This study was funded by a Grant-in-Aid for Scientific Research (C) from the Japan Society for the Promotion of Science [grant number: 18K08886] and a grant from Zenkyoren (National Mutual Insurance Federation of Agricultural Cooperatives) awarded to S.H. The funders had no role in the study design; collection, analysis, and interpretation of the data; writing of the manuscript; and decision to submit the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.