
Abstract
Men and women differ in outcomes following mild traumatic brain injury (TBI). In the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) study, we previously found that women had worse 6-month functional outcome (Glasgow Outcome Score Extended [GOSE]), health-related quality of life (HRQoL), and mental health following mild TBI. The aim of this study was to investigate whether those differences were mediated by psychiatric history, gender-related sociodemographic variables, or by care pathways. We analyzed sex/gender differences in 6-month GOSE, generic and TBI-specific HRQoL, and post-concussion and mental health symptoms using three sets of mediators: psychiatric history, sociodemographic variables (living alone, living with children, education and employment status/job category), and care-pathways (referral to study hospital and discharge destination after emergency department); while controlling for a substantial number of potential confounders (pre-injury health and injury-related characteristics). We included 1842 men and 1022 women (16+) with a Glasgow Coma Score 13-15, among whom 83% had GOSE available and about 60% other 6-month outcomes. We used natural effects models to decompose the total effect of sex/gender on the outcomes into indirect effects that passed through the specified mediators and the remaining direct effects. In our study population, women had worse outcomes and these were only partly explained by psychiatric history, and not considerably explained by sociodemographic variables nor by care pathways. Factors other than differences in specified variables seem to underlie observed differences between men and women in outcomes after mild TBI. Future studies should explore more aspects of gender roles and identity and biological factors underpinning sex and gender differences in TBI outcomes.
Introduction
Traumatic brain injury (TBI) is a global health problem and a significant cause of disability. 1 Men and women differ in TBI epidemiology: men have a higher likelihood of sustaining a TBI, experience it at younger age, and have a higher percentage of TBIs due to motor-vehicle and work-related accidents, while women more often sustain TBI due to falls and intimate partner and domestic violence. 2 -4 Apart from TBI characteristics, differences in outcomes following TBI have also been described. 5
Biological (“sex”) and sociocultural (“gender”) aspects strongly interact in humans, and differences in the context of health outcomes in humans are rarely the product of exclusively sex or gender, but rather their combined effect. 6 To emphasize that it is difficult to disentangle biological and sociocultural components, we will use the term “sex/gender” and “men” and “women.”
The existence and the extent of the differences in outcomes after TBI varies between studies and depends on TBI severity, 7 -9 age, 10,11 and type of outcomes. 7,12 Studies exploring sex/gender differences in outcomes following TBIs classified as moderate/severe mainly showed absence of differences or better outcomes in women. 7,8,13 Following mild TBI, the majority of studies indicate worse psychological and global functioning outcomes in women. 7,9,10 In a European cohort of TBI patients (Collaborative European Neurotrauma Effectiveness Research in TBI [CENTER-TBI]), we found worse functional outcomes, generic and specific health-related quality of life (HRQoL), and more severe post-concussion, depression, anxiety, and post-traumatic stress symptoms in women 6 months after mild TBI, particularly in the age group younger than 45 and for some outcomes in the age group 65+. 14 The differences remained significant after controlling for pre-injury health and injury-related characteristics.
Injury characteristics do not seem probable mechanisms of the observed differences, since men generally sustain more severe mild TBIs and more extracranial injuries and show more pathology on computed tomography (CT) than women. Nevertheless, there is a difference in prevalence rates of psychiatric disorders, 15 with women having higher rates of anxiety and mood disorders, 16 which are the most prevalent disorders worldwide. 17 Pre-injury psychiatric history is the strongest risk factor for post-injury disorders, 18 and therefore can represent vulnerability for appearance of symptoms and lower health-related quality of life after a TBI. 12 Differences in brain morphology, cerebral blood flow, and levels and role of sex steroids may also impact the processes after TBI in a sex-specific manner. 10,19
Apart from biological differences, sociocultural expectations and roles can produce gender-specific stressors, thus interfering with the recovery after TBI. 10,20 -22 In many societies, women are expected to take over the role of primary homemaker and caregiver for children, and men of primary wage earner. In Europe, women are more likely to suffer from poverty, 23 to live alone, to take care of children, to be highly educated, and to be unemployed. 24 Sociodemographic factors are relevant, because they have been shown to be associated with health outcomes and HRQoL in different populations. 25 -27 These factors can have an age-dependent impact due to hormonal variations and changes in roles, responsibilities, and stressors over a life-time. 10,28 Lastly, differential trauma triage and management of TBI can also play a role in functioning following TBI. In the CENTER-TBI study, we found that women with mild TBI had a higher likelihood of direct admission to hospital (trauma center), and a lower likelihood of admission to intensive care in analyses adjusted for pre-injury and injury characteristics. 14 However, the impact of differences in care pathways on the long-term outcomes following mild TBI is unclear.
Possible explanations of differences in post-TBI outcomes between men and women have rarely been tested. Mediation analysis is used to quantify the extent to which the relationship between two variables, such as association between sex/gender and outcomes, can be explained by one or more intermediate variables, while controlling for other relevant factors. We hypothesized that the observed sex/gender differences in outcomes following mild TBI could be partly explained by psychiatric history, sociocultural and gender-role related factors, and acute management of mild TBI. In addition, the importance of these mechanisms may differ across age groups.
Therefore, we aimed to study whether the differences in outcomes after mild TBI, overall and in different age groups, were mediated by: 1) psychiatric history; 2) sociodemographic variables (living alone, living with children, education, and employment status/job category); and/or 3) differences in care-pathways (referral to study hospital and discharge destination after emergency department [ED]).
Methods
Study population
The study population consisted of patients from the prospective multi-center observational CENTER-TBI study (Core data, version 2.1). Data were collected from December 2014 to December 2017 in 63 centers across Europe and Israel. The study was registered with
Inclusion criteria for the core study were a clinical diagnosis of TBI, presentation within 24 h after injury, and an indication for CT scanning. 29 The core dataset included three strata that are differentiated according to care path: patients seen in the ED and then discharged; patients primarily admitted to the intensive care unit (ICU), and patients primarily admitted to the hospital ward. 30
For this study, we selected patients aged 16 years or older, and classified as having mild TBI based on baseline Glasgow Coma Score (GCS) 13 to 15. Sex was recorded on medical forms at admission. Sociodemographic variables, medical history, and clinical and injury characteristics were assessed at admission. The results of first CT scanning reviewed centrally by CENTER-TBI researchers were selected for the analyses.
Ethical approval
The CENTER-TBI study (European Commission [EC] grant 602150) has been conducted in accordance with all relevant laws of the European Union (EU) if directly applicable or of direct effect and all relevant laws of the country where the recruiting sites were located, including but not limited to, the relevant privacy and data protection laws and regulations (the ‘‘Privacy Law’’), the relevant laws and regulations on the use of human materials, and all relevant guidance relating to clinical studies from time to time in force including but not limited to the International Conference on Harmonisation (ICH) Harmonised Tripartite Guideline for Good Clinical Practice (CPMP/ICH/135/95; ‘‘ICH GCP’’) and the World Medical Association Declaration of Helsinki entitled ‘‘Ethical Principles for Medical Research Involving Human Subjects.’’ Informed consent by the patients and/or the legal representative/next of kin was obtained, accordingly to the local legislations, for all patients recruited in the core data set of CENTER-TBI and documented in the e-CRF. Ethical approval was obtained for each recruiting site. The list of sites, ethical committees, approval numbers, and approval dates can be found on the study website
Outcomes at 6 months
Glasgow Outcome Scale Extended (GOSE)
The GOSE 31 assesses global functional outcome following TBI. It provides eight ordinal categories of outcome: dead (1); vegetative state (2); lower severe disability (3); upper severe disability (4); lower moderate disability (5); upper moderate disability (6); lower good recovery (7); and upper good recovery (8). GOSE was assessed at 6 months by either a questionnaire or a telephone interview. When it was assessed outside the time window (range 5–8 months), it was imputed based on all GOSE measurements available. 32 For the analyses, GOSE was dichotomized to incomplete (GOSE <8) and complete (GOSE = 8) return to pre-injury level of functioning.
Short Form Health Surveys (SF-12v2; SF-36v2)
SF-12v2 with 12 items and SF-36v2 with 36 items 33 are self-reported and generic measures of HRQoL. The results can be summarized as mental (MCS) and physical (PCS) component scores ranging from 0 to 100. MCS and PCS were based on a SF-12v2 score, and when there was no SF-12v2 score, the score was derived using corresponding items from available SF-36v2 questionnaires.
Quality of Life after Brain Injury-Overall Scale (QOLIBRI-OS)
The QOLIBRI-OS 34 is a brief TBI-specific index of HRQoL that covers physical condition, cognition, emotions, daily life, personal/social aspects, and current situation/future prospects. The total score is on a scale that ranges 0–100.
Rivermead Post-Concussion Symptoms Questionnaire (RPQ)
The RPQ 35 measures cognitive, somatic, and emotional symptoms that are compared with the pre-injury level. It contains 16 items that can be answered with 0 = not experienced, 1 = no more of a problem (than before the injury), 2 = mild problem, 3 = moderate problem, or 4 = severe problem. When calculating the total score, the category “no more of a problem (than before)” is treated as 0, and it has a score range of 0-64.
Patient Health Questionnaire (PHQ-9)
The PHQ-936 measures symptoms of depression. It contains nine items using a 4-point Likert scale (from 0 = not at all to 3 = nearly every day), and it has a score range of 0–27.
Generalized Anxiety Disorder 7-item scale (GAD-7)
GAD-737 measures symptoms of anxiety. It comprises seven items that can be answered from 0 = not at all to 3 = nearly every day, and it can have a score range of 0–21.
Post-Traumatic Stress Disorder (PTSD)
Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (PCL-5). PCL-538 measures symptoms of PTSD according to DSM-5 criteria. It consists of 20 items that can be answered with 0 = not at all to 4 = extremely, and it has a score range of 0–80.
For QOLIBRI-OS and SF-12v2 higher values indicate better quality of life/more favorable outcomes, and for RPQ, PHQ-9, GAD-7, and PCL-5 higher values indicate more severe symptoms/less favorable outcomes.
Exposure, baseline covariates and mediator variables
Figure 1 shows the examined mediation model for 6-month outcomes. Sex/gender was considered as the “exposure” (i.e., a variable associated with outcome) and it was coded as binary variable (men vs. women).
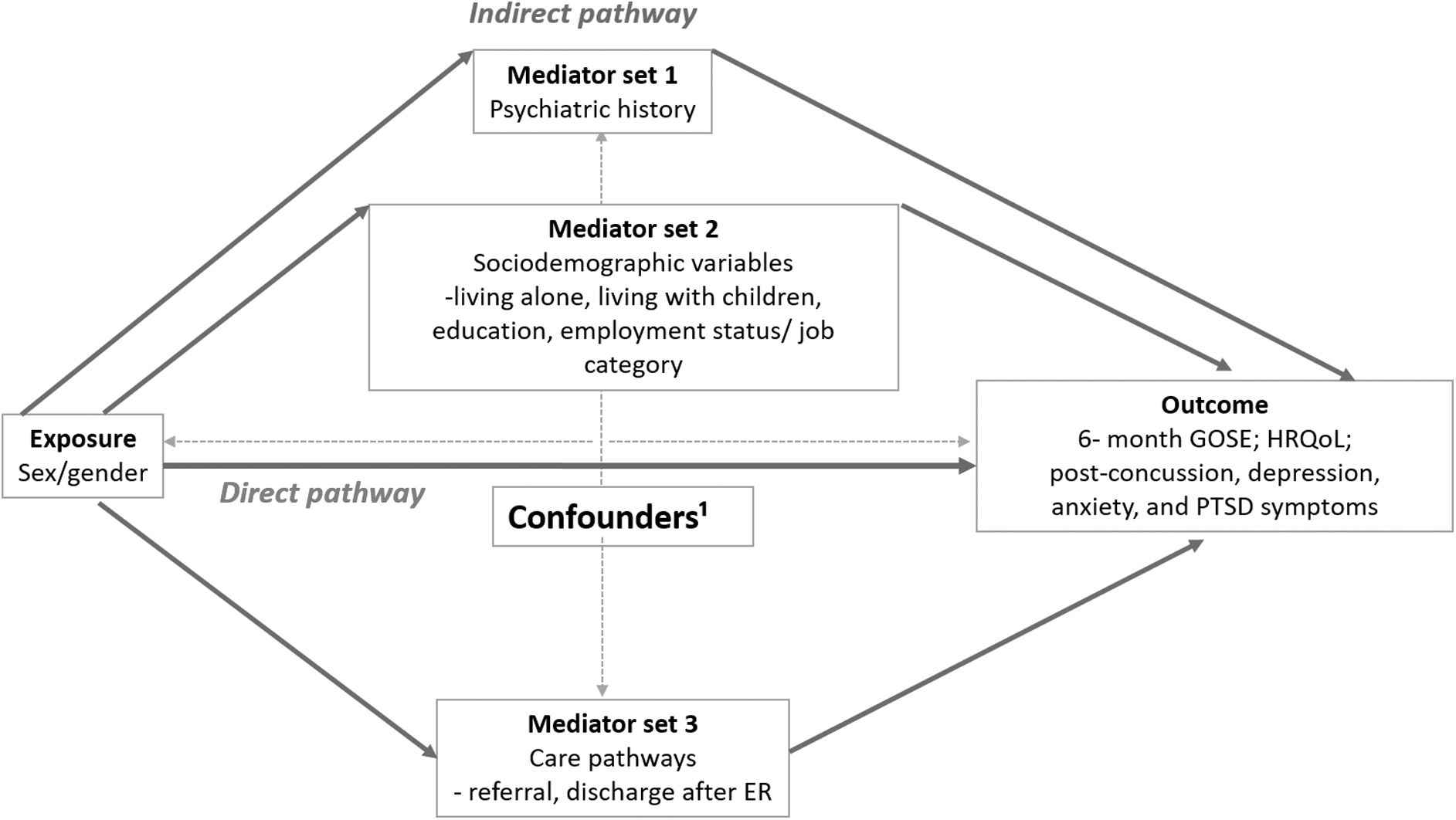
The proposed mediation model with direct and indirect pathways (via psychiatric history, sociodemographic variables and care pathways). 1 Age, pre-injury physical health, cause of injury, baseline Glasgow Coma Score (GCS; 13-15), baseline pupillary reactivity; hypoxia; hypotension, Injury Severity Score (ISS), Marshall CT score, subarachnoid hemorrhage, epidural hematoma. CT, computed tomography; ER, emergency room; GOSE, Glasgow Outcome Scale Extended; HRQoL, health-related quality of life; PTSD, post-traumatic stress disorder.
Psychiatric history included self-reported medical history of anxiety, depression, sleep problems, schizophrenia, substance abuse, or other disorders at admission. Care pathway mediators were selected based on previous analyses of differences between men and women. 14 Referral was categorized to primary (direct transfer to the study hospital) and secondary (transfer from another hospital to the study hospital). Discharge destination from the ED was defined based on discharge home, admission to intensive care unit or operating room, and other admission (hospital ward, other hospital) after ED. Gender-related sociodemographic mediator variables were assessed at admission: living alone (yes/no); living with children (yes/no); education (in years); and employment status/job category (unemployed; student; retired; professional/manager; associate professional/technician; clerk/sales and service worker; skilled manual worker or machine operator; other manual worker). Jobs indicated in the category “other” were classified into existing categories using European Skills/Competences, qualifications and Occupations, 39 and service workers were categorized with clerk/sales workers, and machine operators with skilled manual workers. Sheltered/ special employments was categorized under other manual worker. For age analyses, smaller categories were merged: for age group 16-45 “retired” was merged with “unemployed”; for 45-65 “student” was merged with “unemployed”; for >65, all working categories were merged together, and “unemployed” was merged with “retired.”
To control for confounding between exposure and outcome, exposure and mediator, and mediator and outcome, we conditioned on: age; pre-injury physical health (no systemic disease; mild systemic disease; severe of life-threatening systemic disease); cause of injury (fall or other unintentional injury; motor vehicle accident; violence, suicide attempt or other); baseline GCS (range 13-15); baseline pupillary reactivity (both reactive/one or both unreactive); hypoxia (yes/no); hypotension(yes/no); Injury Severity Score (ISS); first Marshall CT score (no visible pathology; cisterns present with 0-5 mm midline shift, cisterns compressed or absent with 0-5 mm midline shift; midline shift >5 mm, evacuated lesion, non-evacuated mass lesion); subarachnoid hemorrhage on CT (yes/no); and epidural hematoma on CT (yes/no).
Statistical analysis
Descriptive statistics for TBI characteristics, mediators, treatment, and outcome variables were presented separately for men and women using percentages for categorical variables and median with interquartile range for continuous outcomes. Differences were tested using non-parametric tests (e.g., chi-squared and Mann-Whitney U test; Table 1; Supplementary Table S1).
Men and Women with Mild TBI (GCS 13-15): Baseline Characteristics, Psychiatric History, Sociodemographic and Care Pathway Variables, and 6-Month Outcomes
GCS, Glasgow Coma Scale; IQR, interquartile range; ED, emergency department; ICU, intensive care unit; GOSE, Glasgow Outcome Scale Extended; GAD-7, Generalized Anxiety Disorder 7-item scale; ISS, Injury Severity Score; MCS, Mental Composite Score; PCL-5, Post-Traumatic Stress Disorder Checklist for DSM-5; PCS, Physical Composite score; PHQ-9, Patient Health Questionnaire 9-item; QOLIBRI-OS, Quality of Life after Brain Injury-Overall Scale; RPQ, Rivermead Post-Concussion Symptoms Questionnaire; SF12v2, Short Form Health Survey 12 item; TBI, traumatic brain injury.
We performed mediation analyses by fitting natural effect models for nested counterfactuals using the medflex 40 package in R. This method decomposes the total effect of an exposure on an outcome into 1) the natural indirect effect (i.e., the effect of the exposure on the outcome that is due to its effect on the mediator[s]); and 2) natural direct effect (i.e., the effect of the exposure on the outcome that is not due to its effect on the mediator[s]). 40 We chose this method because the decomposition method is valid even in the presence of an interaction effect between the exposure and the mediator(s) on the outcome (which can be explicitly modeled), and it allows consideration of multiple mediators simultaneously. 40,41 The models were fitted using the “imputation-based approach” implemented in the medflex package, which requires fitting a model for the outcome mean. 40 Robust standard errors with sandwich estimator were used to account for the uncertainty inherent to the imputation model.
For each outcome, three joint mediation analyses were performed: one with psychiatric history, one with all sociodemographic variables, and one with all care pathways as specified mediators (Fig. 1). We analyzed the following 6-month outcomes: GOSE, disease-specific HRQoL (QOLIBRI-OS), generic (SF12) mental and physical HRQoL, post-concussion symptoms (RPQ), depression (PHQ-9), anxiety (GAD-7), and PTSD (PCL-5). For each analysis, we reported estimates (regression coefficients) of direct and indirect effect of sex/gender. For models with significant indirect effect, we calculated the mediated proportion by dividing the indirect effect by the total effect, and multiplying by 100. We also performed separate analyses in different age groups: 16-45, 45-65, 65+ years (see the online Supplementary Material).
In addition, we performed sensitivity analyses where we also modeled interactions between exposure and mediators in their effect on the outcomes. Results from these analyses were similar and are reported in the Supplementary Figures S1–S3. Because these models included interaction effect, we reported pure direct effect, pure indirect effect, and mediated interaction (estimate for exposure-mediator interaction).
Mediation analyses were performed in multiple imputed datasets with missing information in covariates and mediators imputed based on an imputation model with sex/gender, and all confounder, mediator, outcome, and auxiliary variables using the R package mice. 42 Exposure values did not have missing values, and unobserved outcome values were not imputed. The results of the mediation analyses were pooled over 10 imputed datasets using the mitools 43 package.
Estimates (regression coefficients) for direct and indirect effects of sex/gender for continuous outcomes are presented in forest plots. Direct and indirect effects for dichotomized complete return to pre-injury functioning (GOSE = 8), obtained in logistic regressions, are reported for women (men as reference category) on a scale of odds ratios.
Results
About two-thirds of patients (64%) with mild TBI were men. Women with mild TBI were older (median 58 years vs. 50 [Q1 32, Q3 65]), had higher GCS (79 % vs. 75% with GCS 15), lower percentage of abnormalities on CT (42.5% vs. 47%), and epidural hematoma (5% vs 10 %), and lower total body injury severity (ISS; 9 [4, 16] vs. 13 [8, 19.]) than men (Table 1; Supplementary Table S1). They sustained more TBIs due to falls (61% vs. 52%), and fewer due to motor vehicle accidents (33% vs. 36%) and violence (6.0% vs. 12.5%); and had worse pre-injury physical (50.0% vs. 58.5% with no systemic disease) and psychiatric health (18% vs. 12% with history of psychiatric disorders; Table 1; Supplementary Table S1).
Fewer women were admitted to ICU or operating room (17% vs. 27%), and more were discharged home (34% vs. 25%). Women had slightly lower years of education (13 [10, 16] vs. 13 [11, 16], p = 0.015), were more often retired (37% vs. 25%), less often had job occupation of skilled manual worker (4% vs. 13%) or other manual worker (7% vs. 12%), and slightly more often of professional/manager (15% vs. 13%). Women more frequently lived alone (27.0% vs. 20.5%; Table 1). Characteristics of men and women in different age groups are presented in Supplementary Table S2.
Mediation analyses
Mediation via psychiatric history
There was a significant indirect effect of sex/gender mediated by psychiatric history (“indirect effect”; Fig. 2) for all outcomes except physical HRQoL (SF-12v2 PCS -0.06 [-0.16, 0.05]): disease specific HRQoL (QOLIBRI-OS; -0.75 [-1.20, -0.30], proportion mediated 16%); generic mental HRQoL (SF-12v2 MCS -0.47 [-0.75, -0.19], proportion mediated 17%), post-concussion (RPQ; 0.36 [0.12, 0.60], proportion mediated 9%), depression (PHQ-9; 0.22 [0.09, 0.36], proportion mediated 16%), anxiety (GAD-7; 0.17 [0.06, 0.27], proportion mediated 14%), and post-traumatic stress symptoms (PCL-5; 0.39 [0.13, 0.65], proportion mediated 18%). Differences in outcomes were partly explained by psychiatric history, but to a small extent compared with other factors (proportion mediated 9% -18%).
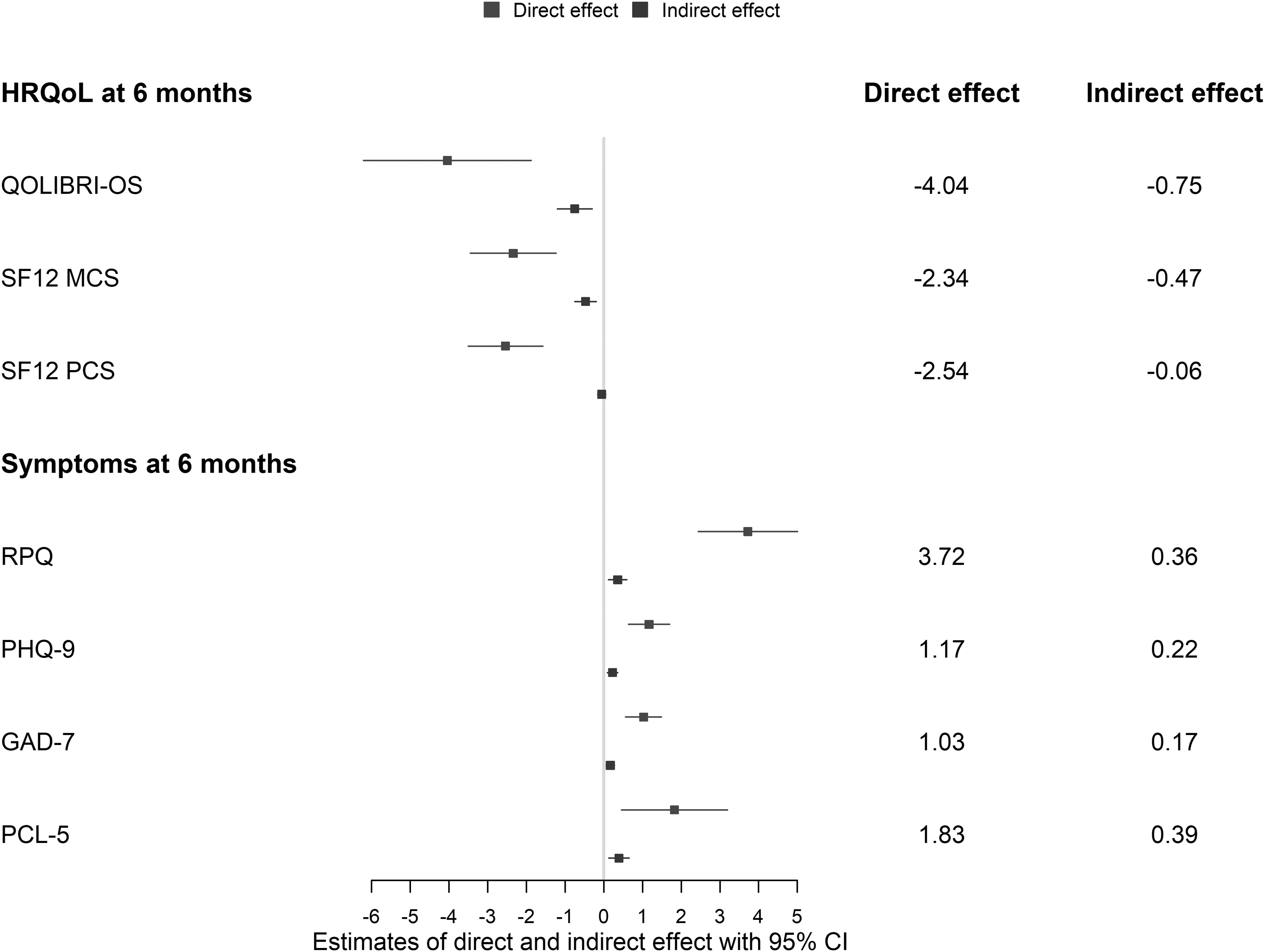
Mediation analyses: Estimates (regression coefficients with 95% confidence intervals) of direct effect of sex/gender and indirect effect via psychiatric history on outcomes following mild TBI: specific (QOLIBRI-OS; n = 1633) and generic (SF12V2; n = 1614) health-related quality of life (HRQoL), and post-concussion (RPQ; n = 1606), depression (PHQ-9; n = 1568), anxiety (GAD-7; n = 1562), and post-traumatic stress (PCL-5; n = 1570) symptoms. QOLIBRI-OS, SF-12v2: higher values better HRQoL. RPQ, PHQ-9, GAD-7, PCL-5: higher values more severe symptoms. QOLIBRI-OS, Quality of Life after Brain Injury-Overall Scale; SF12V2, generic short form health survey; RPQ, Rivermead Post-Concussion Symptoms Questionnaire; PHQ-9, Patient Health Questionnaire; GAD-7, Generalized Anxiety Disorder 7-item scale; PCL-5, Post-Traumatic Stress Disorder Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
The effect of sex/gender not mediated by mental health problems (“direct effect”; Fig. 2) was significant for all outcomes: disease-specific HRQoL (QOLIBRI-OS, -4.04 [-6.21, -1.88]), mental HRQoL (SF-12v2 MCS; -2.34 [-3.45, -1.24]), physical HRQoL (SF-12v2 PCS; -2.54 [-3.50, -1.58] ), and post-concussion (RPQ; 3.72 [2.44, 5.01]), depression (PHQ-9 1.17 [0.64, 1.70]); anxiety (GAD-7 1.03 [0.56, 1.49]); and post-traumatic stress symptoms (PCL-5; 1.83 [0.46, 3.20]).
Logistic regression showed a small indirect effect of sex/gender mediated by psychiatric history (0.96 [0.94-0.99], proportion mediated 9%), and substantial direct effect of sex/gender (0.65 [0.54-0.99]), indicating lower likelihood of women for having better functional outcomes due to other factors.
Analyses in different age groups showed the largest significant indirect effect of sex/gender via psychiatric history in the age group 65 and older, indicating that worse outcomes in older women compared with men were to a considerable degree mediated by psychiatric history: proportion mediated 29% for post-concussion symptoms, 27% for post-traumatic stress symptoms, 25% for anxiety, 24% for depression, 20% for disease-specific and mental HRQoL, 19% for GOSE (Supplementary Fig. S4-S6; Supplementary Table S3).
Joint mediation via gender-related sociodemographic variables
The mediation analyses showed a negligible indirect effect of sex/gender jointly mediated by gender-related sociodemographic variables (“indirect effect”; Fig. 3) for disease specific HRQoL (QOLIBRI-OS; -0.11 [-0.74, 0.51]); generic HRQoL (SF-12v2 MCS -0.06 [-0.34, 0.21]; SF-12v2 PCS -0.05 [-0.31, 0.21]), post-concussion (RPQ; 0.07 [-0.24, 0.38]), depression (PHQ-9; 0.04 [-0.11, 0.18]), anxiety (GAD-7; -0.01 [-0.14, 0.11]), and post-traumatic stress symptoms (PCL-5; -0.01 [-0.36, 0.33]). Therefore, the differences between men and women in 6-month outcomes following mild TBI were not explained by gender-related sociodemographic variables.
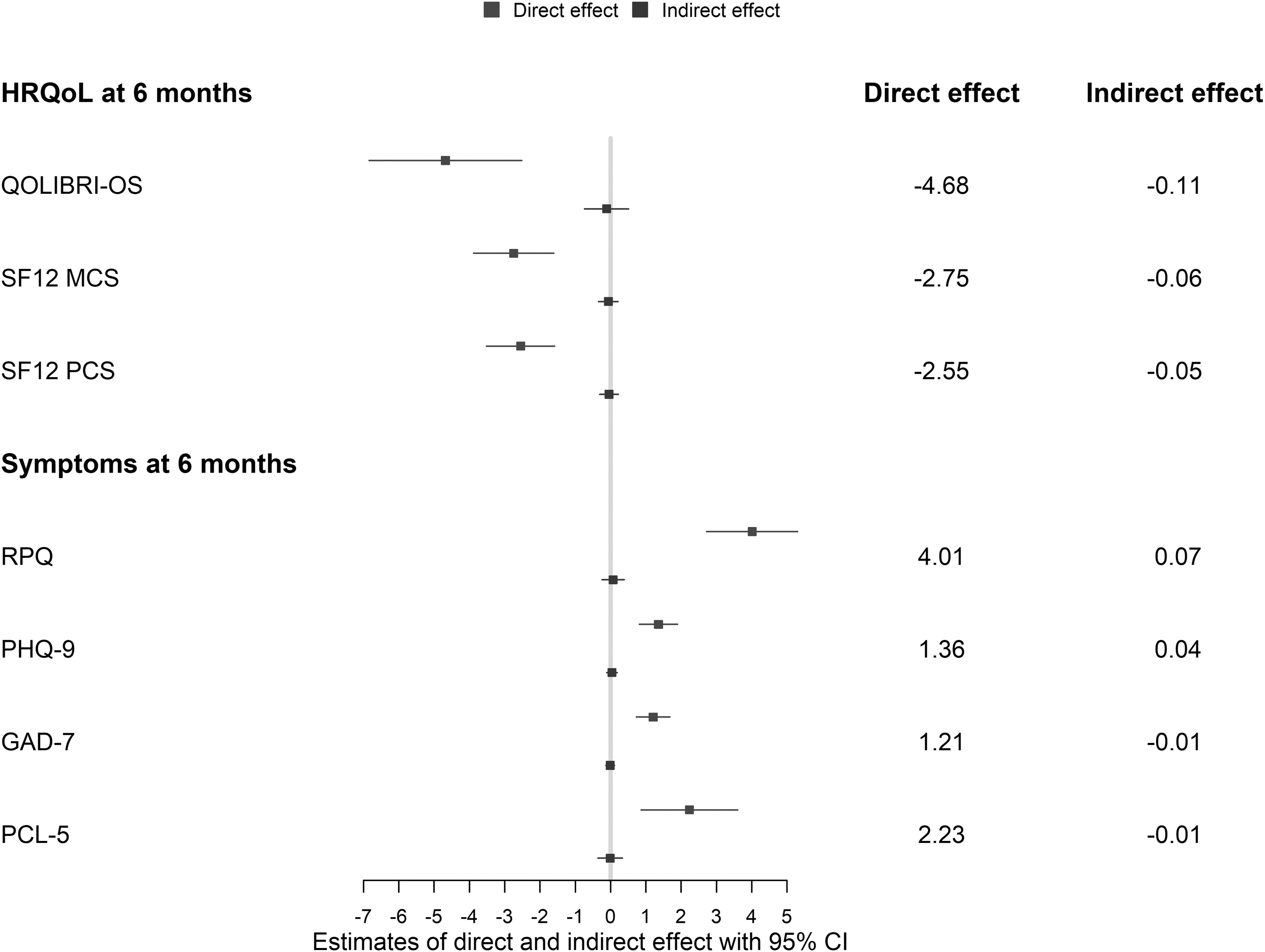
Mediation analyses: estimates (regression coefficients with 95% confidence intervals) of direct effect of sex/gender and indirect effect via sociodemographic variables on outcomes following mild TBI: specific (QOLIBRI-OS; n = 1633) and generic (SF12V2; n = 1614) health-related quality of life (HRQoL), and post-concussion (RPQ; n = 1606), depression (PHQ-9; n = 1568), anxiety (GAD-7; n = 1562), and post-traumatic stress (PCL-5; n = 1570) symptoms. QOLIBRI-OS, SF-12v2: higher values better HRQoL. RPQ, PHQ-9, GAD-7, PCL-5: higher values more severe symptoms. QOLIBRI-OS, Quality of Life after Brain Injury-Overall Scale; SF12V2, generic short form health survey; RPQ, Rivermead Post-Concussion Symptoms Questionnaire; PHQ-9, Patient Health Questionnaire; GAD-7, Generalized Anxiety Disorder 7-item scale; PCL-5, Post-Traumatic Stress Disorder Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
The effect of sex/gender that was not mediated by sociodemographic variables (“direct effect”; Fig. 3) was significant for all outcomes: disease-specific HRQoL (QOLIBRI-OS, -4.68 [-6.84, -2.52]), mental HRQoL (SF-12v2 MCS; -2.75 [-3.88, -1.61]), physical HRQoL (SF-12v2 PCS; -2.55 [-3.51, -1.59]), and post-concussion (RPQ; 4.01 [2.72, 5.30]), depression (PHQ-9; 1.36 [0.82, 1.90]), anxiety (GAD-7; 1.21 [0.74, 1.68], and post-traumatic stress symptoms (PCL-5; 2.23 [0.86, 3.60]).
Logistic regressions showed no indirect effect of sex/gender on complete return to pre-injury level of functioning (GOSE = 8; n = 1161/2376) mediated via sociodemographic variables (odds ratio [OR] 1.02 [0.98, 1.06] for indirect effect). The effect of sex/gender not mediated by these characteristics was significant (GOSE = 8; OR 0.61 [0.51, 0.74] for direct effect), indicating lower likelihood of complete return to pre-injury level of functioning for women due to other factors than the sociodemographic variables specified.
Subgroup age analyses showed the largest (albeit not statistically significant) indirect effect of sex/gender via sociodemographic factors in the group 65 and older, suggesting that worse outcomes among older women were partially mediated by sociodemographic factors. In contrast, in the age groups 16-45 and 45-65, there was a small (insignificant) indirect effect of sex/gender via sociodemographic factors in the opposite direction (Supplementary Fig. S7-S9).
Joint mediation via care pathways
The mediation analyses showed no indirect effect of sex/gender jointly mediated by care pathways (“indirect effect”; Fig. 4) for disease-specific HRQoL (QOLIBRI-OS, 0.07 [-0.12, 0.26]), generic HRQoL (SF12 MCS; 0.06 [-0.05, 0.17]; SF12 PCS -0.02 [-0.11, 0.08]), and post-concussion (RPQ; -0.07 [-0.19, 0.04]), depression (PHQ-9; -0.01 [-0.06, 0.03]), anxiety (GAD-7;-0.02 [-0.06, 0.03]), and post-traumatic stress symptoms (PCL-5; -0.06 [-0.18, 0.06]). Thus, the differences between men and women in 6-month outcomes following mild TBI could not be explained by different care pathways.
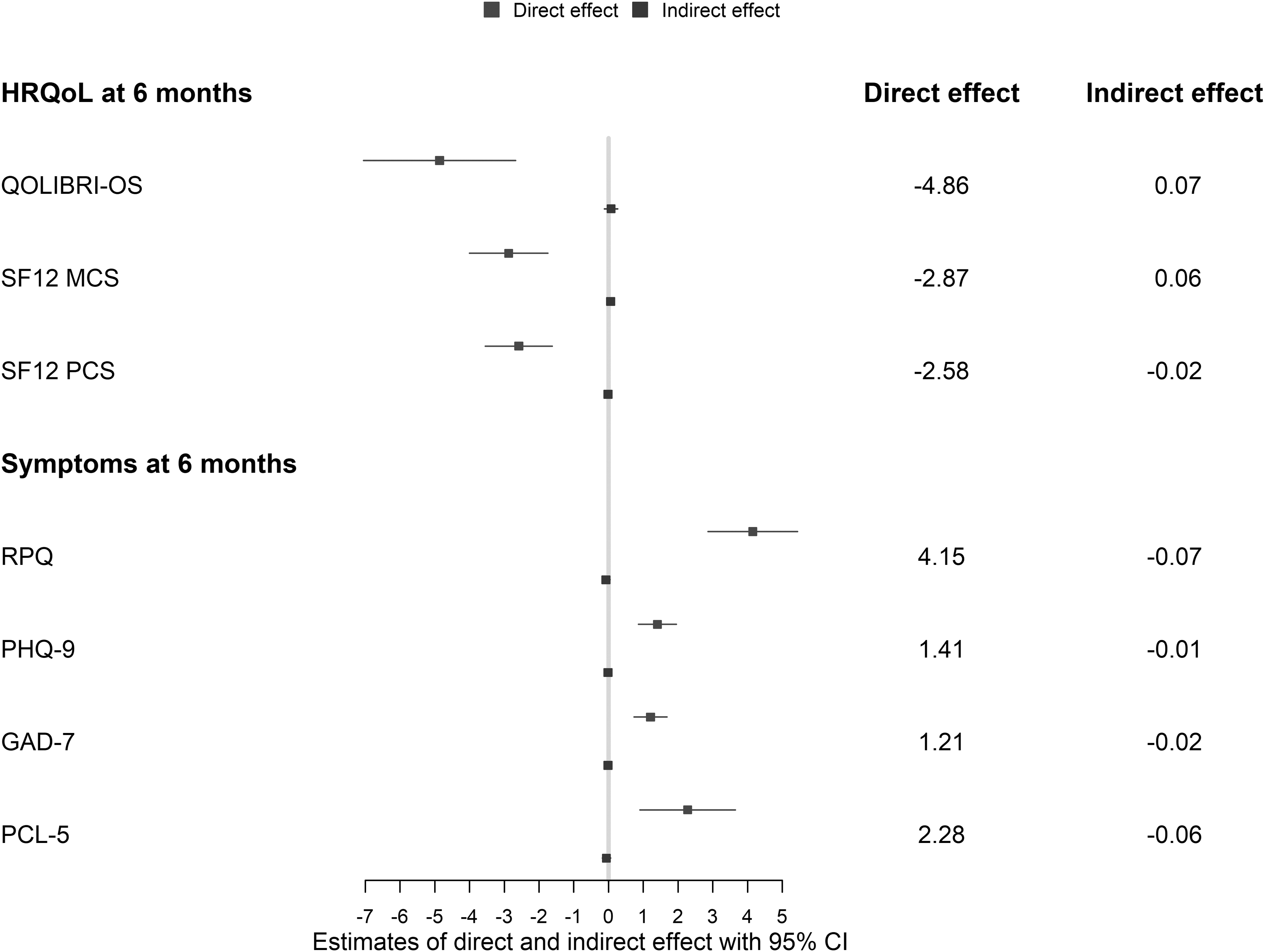
Estimates (regression coefficients with 95% confidence intervals) of direct effect of sex/gender and indirect effect via care pathways on outcomes following mild TBI: specific (QOLIBRI-OS; n = 1633) and generic (SF12; n = 1614) health-related quality of life (HRQoL), and post-concussion (RPQ; n = 1606), depression (PHQ-9; n = 1568), anxiety (GAD-7; n = 1562), and post-traumatic stress (PCL-5; n = 1570) symptoms. QOLIBRI-OS, SF-12v2: higher values indicate better HRQoL. RPQ, PHQ-9, GAD-7, PCL-5: higher values indicate more severe symptoms. QOLIBRI-OS, Quality of Life after Brain Injury-Overall Scale; SF12V2, generic short form health survey; RPQ, Rivermead Post-Concussion Symptoms Questionnaire; PHQ-9, Patient Health Questionnaire; GAD-7, Generalized Anxiety Disorder 7-item scale; PCL-5, Post-Traumatic Stress Disorder Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
The effect of sex/gender not mediated by care pathways (“direct effect”; Fig. 4) was significant for all outcomes: disease-specific HRQoL (-4.86 [-7.05, -2.68]), mental HRQoL (SF-12 MCS; -2.87 [-4.00, -1.74]), physical HRQoL (SF-12 PCS; -2.58 [-3.55, -1.62]), post-concussion (RPQ; 4.15 [2.87, 5.44]), depression (PHQ-9; 1.41 [0.87, 1.95]), anxiety (GAD-7; 1.21 [0.74, 1.68]), and post-traumatic stress symptoms (PCL-5; 2.28 [0.91, 3.65]).
Logistic regressions showed that a small proportion of the effect of sex/gender was mediated by care pathways, very slightly increasing likelihood of complete return to pre-injury level of functioning (GOSE = 8, 1161/2376) for women (1.03 [1.00 - 1.06]). The direct effect of sex/gender was significant, indicating lower likelihood of complete return to pre-injury level of functioning for women (0.60 [0.50-0.73]) due to other factors than care pathways.
In all age groups, the indirect effect of sex/gender via care pathways was negligible (Supplementary Fig. S10-S12).
Discussion
Women show worse functional, health-related quality of life and mental health outcomes following mild TBI. 14 We explored whether these differences were mediated by psychiatric history, gender-related sociodemographic variables, and care pathways. Our results showed that differences in 6-month outcomes were not mediated by gender-related sociodemographic variables (i.e., living alone, living with children, education and employment status/job category), nor by specified care pathways (i.e., hospital referral and discharge destination after ED). Differences in all outcomes except for physical HRQoL were partly mediated by psychiatric history, but the proportion mediated was small. Therefore, other factors than differences in the sociodemographic and care pathway variables explored in this study seem to underlie differences between men and women in outcomes after mild TBI.
History of mental health problems is a risk factor for poor outcome after mild TBI. 44 -46 Generally, women and men have comparable prevalence of psychiatric disorders; however, prevalence of the most frequent mood and anxiety disorders is higher in women. Recent studies suggest that rates of common mental health disorders have increased in women and remained stable in men in the last decades, with younger women at particular risk. 47,48 We found that psychiatric history partly explained worse outcomes in women in all domains except physical health-related quality of life; nevertheless, the sex/gender differences still largely remained unexplained by this factor. In the age group 65 years and older, psychiatric history explained a higher proportion of the women's worse outcomes compared with other age groups. These results, together with the recent finding of sex differences in symptoms after mild TBI but not after orthopedic injury, 12 suggest that symptoms after TBI are not (completely) the result of differences in mental health history.
We selected sociodemographic variables that differed between men and women, and that can be associated with gender roles and with health outcomes. In Europe, women are less likely to be employed, and more likely to take care of children, to live alone, and to finish tertiary education. 24 Overall, these mediators did not substantially explain differences in outcomes between men and women. Only worse outcomes of older women, compared with men of the same age, were to some extent explained by these sociodemographic variables. In contrast to other groups, in the age group 65+, women had lower education and more frequently lived alone.
We had information on employment status and broad job category. In our data, slightly more women were professionals/managers, while more men were manual workers. Because all manager and professional occupations were in the same category, differentiation between higher-status jobs was not possible. That is relevant because women have less access to the highest decision-making positions and higher tertiary education, and are underrepresented on corporate boards in management positions. 49 –52 In addition, women are more likely to be paid less for the same job, and to perform domestic and care giver duties. 53,54 However, we did not have information on salary, hours worked in household, role of a primary wage-earner, and role of a primary caregiver for children/ elderly family members, which can be particularly relevant for younger and middle-age women. 54 Therefore, we could capture gender roles and gender-specific stressors only to a limited extent, 53 which could explain why worse outcomes in women were less explained by specified mediators in age groups 16-65 compared with the 65 years and older. Fulfilling family, household, and work-related duties and being paid less can represent a burden in recovery from a TBI, particularly in young and middle adulthood. 22,55
The role of primary wage earner, and masculine norms such as stoicism, self-reliance, and restrictive emotionality can influence return to work and participation in rehabilitation after a TBI. 56,57 As a consequence, gender identity can impact recovery. 53,58 A qualitative study with men who experienced a TBI demonstrated that gender identity, and in particular masculine norms, motivated men to return to work more quickly and speed up discharge and recovery, which was beneficial for some and detrimental for others. 59 In addition, masculine traits can reduce the likelihood of recognizing and self-reporting health complaints, 60,61 particularly in the domain of psychological functioning. 56 In the general European population, men perceive (or report) better health than women. 24 More detailed measurement of gender identity would contribute to better understanding the underlying mechanisms that cause gender differences in health-related outcomes.
Studies on sex and gender differences in care pathways and their impact on long-term functioning after TBI are scarce. Large retrospective studies of cardiovascular, trauma and critical care patients found that women were less likely to receive ICU treatment. 62 -64 In our data, more women had direct referral to study hospital, and were less triaged to ICU. In studies of treatment and care pathway, it is difficult to completely avoid residual confounding related to medical needs, 64 which could explain observed difference in care pathways. Triage of mild TBI patients to different care pathways is not clearly associated with outcome. 65,66 Because there is no evidence of worse functional outcomes of patients triaged to other destinations, 67 admissions to ICU following mild TBI could often be unnecessary. 66 Additionally, some studies associate ICU admission with increased risk for PTSD 1 year after injury. 68 For some mild TBI patients, however, monitoring in hospital and intensive care can be beneficial to promptly identify any deterioration and to initiate surgery or critical care intervention if necessary. 66 For the functional, HRQoL and mental health outcomes we analyzed, care pathways did not explain differences between men and women.
Biological differences and particularly sex steroids represent another pathway that can mediate sex differences in outcomes. 69 For instance, animal models suggest that the hypothalamic-pituitary-adrenal axis (HPA) axis, which modulates the stress response, 70 and microglia, 71 which influence cerebral inflammation, have sex-specific responses. After TBI, female rodents have shown stronger inflammatory response, 19 greater anxiety and reduction of sociability, 72 and differential stress response 70 than males. Hormonal differences can be of particular importance in explanation of symptoms in pre-menopausal women. 10 Moreover, genetic factors can interact with sex and/or gender on their impact of outcome after TBI. For example, being carrier of an APOE4 allele had negative impact on the GOSE measured 1-5 years after TBI, and the effect was stronger in women compared with men. 73
To our knowledge, this is the first study that explores underlying mechanisms of differences in outcomes after TBI between men and women using a mediation framework. We explored three possible explanatory pathways: one via psychiatric history, one via gender-related sociodemographic variables, and one via care pathways. The method allowed studying joint mediation for both pathways, and including interaction between sex/gender and mediators in their impact on outcomes. We used a large multi-center European cohort of TBI patients and included different domains of functioning after 6 months.
Implications of this study involve informing clinicians and patients about different risks of poorer outcomes following mild TBI in context of sex, gender, and mental health. If supported by future evidence, the results of our and other recent studies 11,12 could be utilized for organizing follow up care, for instance scheduling earlier or more frequent appointments for women and persons with (history of) psychiatric difficulties. Further, other potential sociocultural and biological mechanisms of sex/gender differences should be measured and explored in upcoming TBI research.
This study also has some limitations. Mediation analyses assume complete control for confounding between exposure and mediators, mediators and outcome, and exposure and outcome. We controlled for a substantial number of pre-injury, clinical and injury characteristics. In addition, for each set of mediators, we performed joint mediation with mediators included simultaneously, thus providing additional control for confounding. However, unmeasured confounding remains possible, which might have biased the observed associations. Moreover, some relationships may be non-linear, which can complicate adjustment. 44 We only had information on self-reported medical history of psychiatric disorders, but not a measure of mental health symptoms before/ at the time of injury. We did not adjust for or analyze the impact of interventions and therapies after hospital admission and discharge. Further, as frequently occurs in longitudinal TBI studies, 6-month outcomes were not available in a considerable number of patients, which can compromise validity.74
The subgroup age analyses had lower power. Additionally, age groups (16-45, 45-65, 65+) were rather broad and possibly included persons in different life stages, characterized by different roles, stressors and biological processes. For instance, some previous studies found increased risk of PTSD following mild TBI for women aged 30-39 versus 18-29, 11 and of post-concussion symptoms for women aged 35-49 versus 17-34. 7,12 In our study, the group aged 45-65 likely included both females in pre-menopause and menopause, and groups 45-65 and 65+ included both retired and (un)employed persons. The results are obtained in a European study with a substantial proportion of large trauma centers in urban areas in North-Western Europe. 30,75 Therefore, the generalizability of findings to other areas is limited.
Important indicators of gender roles and identity were not measured in this study. Sex was based on medical forms and will not always correspond to gender (identifying as a woman or a man). We recognize that there is a notable minority of intersex, transgender, and non-binary persons, who are not captured by this dichotomy. We recommend inclusion of self-reports and more measures of gender where practical in future TBI studies.
In conclusion, men and women differ in outcomes following mild TBI, and those differences are only partly explained by psychiatric history, and not explained by gender-related sociodemographic and care pathway differences. Future studies should explore further aspects of gender roles and identity, and biological factors as underpinnings of sex and gender differences in TBI outcomes.
Footnotes
Acknowledgments
We are grateful to all patients and investigators who participated in the CENTER-TBI study.
The CENTER-TBI Participants and Investigators
Cecilia Åkerlund, Karolinska Institutet, Stockholm, Sweden; Krisztina Amrein, University of Pécs, Pécs, Hungary, Nada Andelic, Oslo University Hospital and University of Oslo, Oslo, Norway; Lasse Andreassen, University Hospital Northern Norway, Tromso, Norway; Audny Anke, University Hospital Northern Norway, Tromso, Norway; Anna Antoni, Medical University Vienna, Vienna, Austria; Gérard Audibert, University Hospital Nancy, Nancy, France, University Hospital Nancy, Nancy, France; Philippe Azouvi, Raymond Poincare Hospital, Assistance Publique–Hopitaux de Paris, Paris, France; Maria Luisa Azzolini, S. Raffaele University Hospital, Milan, Italy; Ronald Bartels, Radboud University Medical Center, Nijmegen, the Netherlands; Pál Barzó, University of Szeged, Szeged, Hungary; Romuald Beauvais, ARTTIC, Munchen, Germany; Ronny Beer, Medical University of Innsbruck, Innsbruck, Austria; Bo-Michael Bellander, Karolinska University Hospital, Stockholm, Sweden; Antonio Belli, NIHR Surgical Reconstruction and Microbiology Research Centre, Birmingham, UK; Habib Benali, Assistance Publique–0Hopitaux de Paris, Paris, France; Maurizio Berardino, AOU Città della Salute e della Scienza di Torino–Orthopedic and Trauma Center, Torino, Italy; Luigi Beretta, S. Raffaele University Hospital, Milan, Italy; Morten Blaabjerg, Odense University Hospital, Odense, Denmark; Peter Bragge, Monash University, Victoria, Australia; Alexandra Brazinova, Trnava University, Trnava, Slovakia; Vibeke Brinck, Quesgen Systems Inc., Burlingame, California, USA; Joanne Brooker, Monash University, Melbourne, Australia; Camilla Brorsson, Umeå University, Umeå, Sweden; Andras Buki, University of Pécs, Hungary; Monika Bullinger, Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany; Manuel Cabeleira, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Alessio Caccioppola, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Emiliana Calappi, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Maria Rosa Calvi, S. Raffaele University Hospital, Milan, Italy; Peter Cameron, Monash University, Melbourne, Victoria, Australia; Guillermo Carbayo Lozano, Hospital of Cruces, Bilbao, Spain; Marco Carbonara, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Ana M. Castaño-León, Hospital Universitario 12 de Octubre, Madrid, Spain; Simona Cavallo, AOU Città della Salute e della Scienza di Torino–Orthopedic and Trauma Center, Torino, Italy; Giorgio Chevallard, Niguarda Hospital, Milan, Italy; Arturo Chieregato, Niguarda Hospital, Milan, Italy; Giuseppe Citerio, Università Milano Bicocca, Milano, Italy and ASST di Monza, Monza, Italy; Iris Ceyisakar, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Hans Clusmann, Aachen University, Aachen, Germany; Mark Coburn, University Hospital of Aachen, Aachen, Germany; Jonathan Coles, Cambridge University Hospital NHS Foundation Trust, Cambridge, UK; Jamie D. Cooper, Monash University and The Alfred Hospital, Melbourne, Victoria, Australia; Marta Correia, MRC Cognition and Brain Sciences Unit, Cambridge, UK; Amra Čović, Universitätsmedizin Göttingen, Göttingen, Germany; Nicola Curry, Oxford University Hospitals NHS Trust, Oxford, UK; Endre Czeiter, University of Pécs, Hungary; Marek Czosnyka, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Claire Dahyot-Fizelier, CHU Poitiers, Potiers, France; Paul Dark, Salford Royal Hospital NHS Foundation Trust, Salford, UK; Helen Dawes, Oxford Brookes University, Oxford, UK; Véronique De Keyser, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Vincent Degos, Assistance Publique–Hopitaux de Paris, Paris, France; Francesco Della Corte, Maggiore Della Carità Hospital, Novara, Italy; Hugo den Boogert, Radboud University Medical Center, Nijmegen, the Netherlands; Bart Depreitere, University Hospitals Leuven, Leuven, Belgium; Đula Đilvesi, University of Novi Sad, Novi Sad, Serbia; Abhishek Dixit, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Emma Donoghue, Monash University, Melbourne, Australia; Jens Dreier, Charité – Universitätsmedizin Berlin, Berlin, Germany; Guy-Loup Dulière, CHR Citadelle, Liège, Belgium; Ari Ercole, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Patrick Esser, Oxford Brookes University, Oxford, UK; Erzsébet Ezer, University of Pécs, Pécs, Hungary; Martin Fabricius, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark; Valery L. Feigin, Auckland University of Technology, Auckland, New Zealand; Kelly Foks, Erasmus MC, Rotterdam, the Netherlands; Shirin Frisvold, University Hospital Northern Norway, Tromso, Norway; Alex Furmanov, Hadassah-Hebrew University Medical Center, Jerusalem, Israel; Pablo Gagliardo, Fundación Instituto Valenciano de Neurorrehabilitación (FIVAN), Valencia, Spain; Damien Galanaud, Assistance Publique – Hopitaux de Paris, Paris, France; Dashiell Gantner, Monash University, Melbourne, Victoria, Australia; Guoyi Gao, Shanghai Renji Hospital, Shanghai Jiaotong University/School of Medicine, Shanghai, China; Pradeep George, Karolinska Institutet, Stockholm, Sweden; Alexandre Ghuysen, CHU, Liège, Belgium; Lelde Giga, Pauls Stradins Clinical University Hospital, Riga, Latvia; Ben Glocker, Imperial College London, London, UK; Jagoš Golubovic, University of Novi Sad, Novi Sad, Serbia; Pedro A. Gomez, Hospital Universitario 12 de Octubre, Madrid, Spain; Johannes Gratz, Medical University of Vienna, Austria; Benjamin Gravesteijn, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Francesca Grossi, Maggiore Della Carità Hospital, Novara, Italy; Russell L. Gruen, Medical University of Vienna, Austria; Deepak Gupta, All India Institute of Medical Sciences, New Delhi, India; Juanita A. Haagsma, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Iain Haitsma, Erasmus MC, Rotterdam, the Netherlands; Raimund Helbok, Medical University of Innsbruck, Innsbruck, Austria; Eirik Helseth, Oslo University Hospital, Oslo, Norway; Lindsay Horton, University of Stirling, Stirling, UK; Jilske Huijben, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Peter J. Hutchinson, Addenbrooke's Hospital and University of Cambridge, Cambridge, UK; Bram Jacobs, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; Stefan Jankowski, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK; Mike Jarrett, Quesgen Systems Inc., Burlingame, California, USA; Ji-yao Jiang, Shanghai Renji Hospital, Shanghai Jiaotong University/School of Medicine, Shanghai, China; Faye Johnson, Salford Royal Hospital NHS Foundation Trust, Salford, UK; Kelly Jones, Auckland University of Technology, Auckland, New Zealand; Mladen Karan, University of Novi Sad, Novi Sad, Serbia; Angelos G. Kolias, Addenbrooke's Hospital and University of Cambridge, Cambridge, UK; Erwin Kompanje, Erasmus Medical Center, Rotterdam, the Netherlands; Daniel Kondziella, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark; Evgenios Koraropoulos, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Lars-Owe Koskinen, Umeå University, Umeå, Sweden; Noémi Kovács, University of Pécs, Pécs, Hungary; Ana Kowark, University Hospital of Aachen, Aachen, Germany; Alfonso Lagares, Hospital Universitario 12 de Octubre, Madrid, Spain; Linda Lanyon, Karolinska Institutet, Stockholm, Sweden; Steven Laureys, University of Liège, Liège, Belgium; Fiona Lecky, University of Sheffield, Sheffield, UK, and Salford Royal Hospital, Salford UK; Didier Ledoux, University of Liège, Liège, Belgium; Rolf Lefering, Witten/Herdecke University, Cologne, Germany; Valerie Legrand, ICON, Paris, France; Aurelie Lejeune, Lille University Hospital, Lille, France; Leon Levi, Rambam Medical Center, Haifa, Israel; Roger Lightfoot, University Hospitals Southhampton NHS Trust, Southhampton, UK; Hester Lingsma, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Andrew I.R. Maas, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Marc Maegele, Cologne-Merheim Medical Center (CMMC), Witten/Herdecke University, Cologne, Germany; Marek Majdan, Trnava University, Trnava, Slovakia; Alex Manara, Southmead Hospital, Bristol, Bristol, UK; Geoffrey Manley, University of California, San Francisco, California, USA; Costanza Martino, M. Bufalini Hospital, Cesena, Italy; Hugues Maréchal, CHR Citadelle, Liège, Belgium; Julia Mattern, University Hospital Heidelberg, Heidelberg, Germany; Catherine McMahon, The Walton Centre NHS Foundation Trust, Liverpool, UK; Béla Melegh, University of Pécs, Pécs, Hungary; David Menon, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Tomas Menovsky, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Ana Mikolic, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Benoit Misset, University of Liège, Liège, Belgium; Visakh Muraleedharan, Karolinska Institutet, Stockholm, Sweden; Lynnette Murray, Monash University, Melbourne, Victoria, Australia; Ancuta Negru, Emergency County Hospital Timisoara, Timisoara, Romania; David Nelson, Karolinska Institutet, Stockholm, Sweden; Virginia Newcombe, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Daan Nieboer, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; József Nyirádi, University of Pécs, Pécs, Hungary; Otesile Olubukola, University of Sheffield, Sheffield, UK; Matej Oresic, Örebro University, Örebro, Sweden; Fabrizio Ortolano, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Aarno Palotie, University of Helsinki, Helsinki, Finland, Massachusetts General Hospital, Boston, MA, USA, and The Broad Institute of MIT and Harvard, Cambridge, MA, USA; Paul M. Parizel, University Hospital of Grenoble, Grenoble, France; Jean-François Payen, University Hospital of Grenoble, Grenoble, France; Natascha Perera, ARTTIC, Munchen, Germany; Vincent Perlbarg, Assistance Publique – Hopitaux de Paris, Paris, France; Paolo Persona, Azienda Ospedaliera Università di Padova, Padova, Italy; Wilco Peul, Leiden University Medical Center, Leiden, the Netherlands and Medical Center Haaglanden, the Hague, the Netherlands. Anna Piippo-Karjalainen, Helsinki University Central Hospital; Matti Pirinen, University of Helsinki, Helsinki, Finland; Horia Ples, Emergency County Hospital Timisoara, Timisoara, Romania; Suzanne Polinder, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Inigo Pomposo, Hospital of Cruces, Bilbao, Spain; Jussi P. Posti, Turku University Hospital and University of Turku, Turku, Finland; Louis Puybasset, Pitié -Salpêtrière Teaching Hospital, Assistance Publique, Hôpitaux de Paris and University Pierre et Marie Curie, Paris, France; Andreea Radoi, Vall d'Hebron Research Institute, Barcelona, Spain; Arminas Ragauskas, Kaunas University of Technology and Vilnius University, Vilnius, Lithuania; Rahul Raj, Helsinki University Central Hospital; Malinka Rambadagalla, Rezekne Hospital, Latvia; Jonathan Rhodes, NHS Lothian and University of Edinburg, Edinburgh, UK; Sylvia Richardson, Cambridge Institute of Public Health, Cambridge, UK; Sophie Richter, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Samuli Ripatti, University of Helsinki, Helsinki, Finland; Saulius Rocka, Kaunas University of Technology and Vilnius University, Vilnius, Lithuania; Cecilie Roe, Oslo University Hospital/University of Oslo, Oslo, Norway; Olav Roise, Oslo University Hospital, Oslo, Norway; Jonathan Rosand, The Broad Institute, Cambridge MA Harvard Medical School and Massachusetts General Hospital, Boston MA, USA; Jeffrey V. Rosenfeld, The Alfred Hospital, Monash University, Melbourne, Victoria, Australia; Christina Rosenlund, Odense University Hospital, Odense, Denmark; Guy Rosenthal, Hadassah-Hebrew University Medical Center, Jerusalem, Israel; Rolf Rossaint, University Hospital of Aachen, Aachen, Germany; Sandra Rossi, Azienda Ospedaliera Università di Padova, Padova, Italy; Daniel Rueckert, Imperial College London, London, UK; Martin Rusnák, International Neurotrauma Research Organisation, Vienna, Austria; Juan Sahuquillo, Vall d'Hebron Research Institute, Barcelona, Spain; Oliver Sakowitz, University Hospital Heidelberg, Heidelberg, Germany and Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany; Renan Sanchez-Porras, Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany; Janos Sandor, University of Debrecen, Debrecen, Hungary; Nadine Schäfer, Witten/Herdecke University, Cologne, Germany; Silke Schmidt, University Greifswald, Greifswald, Germany; Herbert Schoechl, AUVA Trauma Hospital, Salzburg, Austria; Guus Schoonman, Elisabeth-Twee Steden Ziekenhuis, Tilburg, the Netherlands; Rico Frederik Schou, Odense University Hospital, Odense, Denmark; Elisabeth Schwendenwein, Medical University Vienna, Vienna, Austria; Charlie Sewalt, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Toril Skandsen, Norwegian University of Science and Technology, NTNU and St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; Peter Smielewski, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Abayomi Sorinola, University of Pécs, Pécs, Hungary; Emmanuel Stamatakis, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Simon Stanworth, Oxford University Hospitals NHS Trust, Oxford, UK; Robert Stevens, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; William Stewart, Queen Elizabeth University Hospital and University of Glasgow, Glasgow, UK; Ewout W. Steyerberg, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands and Leiden University Medical Center, Leiden, the Netherlands; Nino Stocchetti, Milan University, and Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy; Nina Sundström, Umeå University, Umeå, Sweden; Anneliese Synnot, Monash University, Melbourne, Australia and La Trobe University, Melbourne, Australia; Riikka Takala, Turku University Hospital and University of Turku, Turku, Finland; Viktória Tamás, University of Pécs, Pécs, Hungary; Tomas Tamosuitis, Kaunas University of Health Sciences, Kaunas, Lithuania; Mark Steven Taylor, Trnava University, Trnava, Slovakia; Braden Te Ao, Auckland University of Technology, Auckland, New Zealand; Olli Tenovuo, Turku University Hospital and University of Turku, Turku, Finland; Alice Theadom, Auckland University of Technology, Auckland, New Zealand; Matt Thomas, Southmead Hospital, Bristol, Bristol, UK; Dick Tibboel, Erasmus Medical Center, Sophia Children's Hospital, Rotterdam, the Netherlands; Marjolein Timmers, Erasmus Medical Center, Rotterdam, the Netherlands; Christos Tolias, Kings College London, London, UK; Tony Trapani, Monash University, Melbourne, Victoria, Australia; Cristina Maria Tudora, Emergency County Hospital Timisoara, Timisoara, Romania; Peter Vajkoczy, Charité – Universitätsmedizin Berlin, Berlin, Germany; Shirley Vallance, Monash University, Melbourne, Victoria, Australia; Egils Valeinis, Pauls Stradins Clinical University Hospital, Riga, Latvia; Zoltán Vámos, University of Pécs, Pécs, Hungary; Mathieu van der Jagt, Erasmus MC – University Medical Center Rotterdam, Rotterdam, the Netherlands; Gregory Van der Steen, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Joukje van der Naalt, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; Jeroen T.J.M. van Dijck, Leiden University Medical Center, Leiden, the Netherlands and Medical Center Haaglanden, the Hague, the Netherlands; Thomas A. van Essen, Leiden University Medical Center, Leiden, the Netherlands and Medical Center Haaglanden, the Hague, the Netherlands; Wim Van Hecke, icoMetrix NV, Leuven, Belgium; Caroline van Heugten, Oxford Brookes University, Oxford, UK; Dominique Van Praag, Antwerp University Hospital, Edegem, Belgium; Thijs Vande Vyvere, icoMetrix NV, Leuven, Belgium; Roel P.J. van Wijk, Leiden University Medical Center, Leiden, the Netherlands and Medical Center Haaglanden, the Hague, the Netherlands; Alessia Vargiolu, ASST di Monza, Monza, Italy; Emmanuel Vega, Lille University Hospital, Lille, France; Kimberley Velt, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Jan Verheyden, icoMetrix NV, Leuven, Belgium; Paul M. Vespa, University of California, Los Angeles, Los Angeles, California, USA; Anne Vik, Norwegian University of Science and Technology, NTNU, Trondheim, Norway and St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; Rimantas Vilcinis, Kaunas University of Health Sciences, Kaunas, Lithuania; Victor Volovici, Erasmus MC, Rotterdam, the Netherlands; Nicole von Steinbüchel, Universitätsmedizin Göttingen, Göttingen, Germany; Daphne Voormolen, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Petar Vulekovic, University of Novi Sad, Novi Sad, Serbia; Kevin K.W. Wang, University of Florida, Gainesville, Florida, USA; Eveline Wiegers, Erasmus Medical Center-University Medical Center, Rotterdam, the Netherlands; Guy Williams, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Lindsay Wilson, University of Stirling, Stirling, UK; Stefan Winzeck, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK; Stefan Wolf, Charité – Universitätsmedizin Berlin, Berlin, Germany; Zhihui Yang, University of Florida, Gainesville, Florida, USA; Peter Ylén, VTT Technical Research Centre, Tampere, Finland; Alexander Younsi, University Hospital Heidelberg, Heidelberg, Germany; Frederick A. Zeiler, University of Cambridge, Addenbrooke's Hospital, Cambridge, UK and University of Manitoba, Winnipeg, MB, Canada; Veronika Zelinkova, Trnava University, Trnava, Slovakia; Agate Ziverte, Pauls Stradins Clinical University Hospital, Riga, Latvia; and Tommaso Zoerle, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy.
Funding Information
This study was supported by The Netherlands Organization for Health Research and Development (ZonMw). The authors A. Mikolic, S. Polinder, L. Wilson and M. Zeldovich were supported by the European Union 7th Framework Programme (EC grant 602150). Additional support was obtained from the Hannelore Kohl Stiftung (Germany), OneMind (USA), Integra LifeSciences Corporation (USA), and Neurotrauma Sciences (USA).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
Supplementary Figure S10
Supplementary Figure S11
Supplementary Figure S12
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.