
Abstract
Over the past four decades, there have been progressive changes in the epidemiology of traumatic spinal cord injury (tSCI). We assessed trends in demographic and injury-related variables in traumatic cervical spinal cord injury (tCSCI) patients over an 18-year period at a single Level I trauma center. We included all magnetic resonance imaging–confirmed tCSCI patients ≥15 years of age for years 2001–2018. Among 1420 patients, 78.3% were male with a mean age 51.5 years. Etiology included falls (46.9%), motor vehicle collisions (MVCs; 34.2%), and sports injuries (10.9%). Median American Spinal Injury Association (ASIA) Motor Score (AMS) was 44, complete tCSCI was noted in 29.6% of patients, fracture dislocations were noted in 44.7%, and median intramedullary lesion length (IMLL) was 30.8 mm (complete injuries 56.3 mm and incomplete injuries 27.4 mm). Over the study period, mean age and proportion of falls increased (p < 0.001) whereas proportion attributable to MVCs and sports injuries decreased (p < 0.001). Incomplete injuries, AMS, and the proportion of patients with no fracture dislocations increased whereas complete injuries decreased significantly. IMLL declined (p = 0.17) and proportion with hematomyelia did not change significantly. In adjusted regression models, increase in age and decreases in prevalence of MVC mechanism and complete injuries over time remained statistically significant. Changes in demographic and injury-related characteristics of tCSCI patients over time may help explain the observed improvement in outcomes. Further, improved clinical outcomes and drop in IMLL may reflect improvements in initial risk assessment and pre-hospital management, advances in healthcare delivery, and preventive measures including public education.
Introduction
Traumatic spinal cord injury (tSCI) is a major unsolved challenge in medicine. Globally, prevalence of tSCI ranges from 250 to 900 per million, depending on the country, and annual national incidence ranges from 8 to 50 per million. 1,2 In North America, incidence has been largely stable, with 53–54 per million from 1993 to 2012 in the United States 3 and 36 per million from 1995 and 2004 in Canada. 4 Half of these patients suffered a complete lesion, and one third become tetraplegic. 5 To date, therapeutic options remain limited, leaving patients with severe neurological abnormalities that persist for decades until death.
Magnetic resonance imaging (MRI) has gained prominence as an objective measure of tissue injury severity after tSCI. The MRI measure of intramedullary lesion length (IMLL) is believed to accurately reflect the pathological sequelae of both the initial trauma plus the subsequent “progressive hemorrhagic necrosis,” an autodestructive process that causes significant rostrocaudal expansion of edema and hemorrhage during the first 12–24 h and that greatly impacts neurological function. 6,7 With motor-complete tSCI (American Spinal Injury Association [ASIA] grades A and B), the spinal cord injury expands at a rate of ∼900 μm/h, reaching its peak at 24 h. 8 Uncontrolled clinical studies have confirmed the relationship between IMLL, neurological function, and recovery. 9 –11 The IMLL is significantly greater in patients with complete injury compared to incomplete injury. 12,13 When long-term improvement in neurological function is measured by grade conversion in the ASIA Impairment Scale (AIS), each additional 10-mm increase in IMLL drops the likelihood of upward AIS grade conversion by 40%. 14
Large-scale cross-sectional and population-based studies demonstrate noteworthy shifts in the epidemiology of tSCI, especially with regard to age at injury and mechanism. Average age at injury has increased from 28.7 years in the 1970s to 42.2 years during 2010–2014, and vehicular crashes continue to be the leading cause of tSCI overall, but the percentage has declined from 47.0% in the 1970s to 38.1% during 2010–2014, whereas injuries caused by falls have increased over time, particularly among those >45 years of age. 15 Similar trends regarding age and mechanism have been observed in other studies as well. 3,16 –18 Notably, in some of these studies, the trends toward older age and more falls have been accompanied by reduced clinical injury severity at baseline, including increased numbers of motor incomplete injuries. 15,16 In addition, there has been a trend over time toward increasing AIS grade conversion, with 16%, 28%, and 56% of patients exhibiting AIS grade A conversion at 1 year, as reported in 1999, 19 2009, 20 and 2020, 11 respectively.
Shifts in age and mechanism, along with trends toward reduced clinical injury severity at baseline, could potentially be linked to reduced tissue injury severity, as might be revealed by the IMLL. Alternatively, the same trends in age, mechanism, and clinical injury severity could be accounted for by an increase in the most common motor-incomplete lesion, central cord syndrome, which is associated with high rates of AIS grade conversion, 9 and which is not fully characterized by the IMLL. 21 Also, trends toward improvements in AIS grade conversion could potentially be attributable to reduced tissue injury severity or, alternatively, to improved care, including surgical care. 11 Here, we present a longitudinal analysis of tCSCI, which spans 18 years (2001–2018) and involves 1420 patients at a single institution, wherein admission MRIs for each patient were available to characterize tissue-injury severity at baseline.
Methods
Study population
We conducted a retrospective analysis of tCSCI patients managed at the University of Maryland R Adams Cowley Shock Trauma Center, a Level I trauma center, over an 18-year period (2001–2018). We identified 2076 tCSCI patients from the Maryland State Trauma Registry using the International Classification of Disease (ICD), Ninth Revision (ICD-9) codes 806.0, 806.1, and 952.0 (2001–2015) and ICD, Tenth Revision (ICD-10) codes S14.0 and S14.1 (2016–2018).
Management of cervical traumatic spinal cord injury at the trauma center
Patients were transported from the scene of the accident to the trauma resuscitation unit by the emergency medical technicians back-boarded, in a hard cervical collar and chin strap an average of 1.1 h after trauma. 14,22 Three teams of general surgeons surveyed the patients for presence of multiple trauma and need for further resuscitation. Once stable, patients were examined by the neurosurgery team to determine American Spinal Injury Association (ASIA) motor score (AMS) and AIS grade based on the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) criteria. 23,24 ISNCSCI criteria were used to determine whether the tCSCI was complete (AIS grade A) or incomplete (AIS grades B, C, and D). The next step was a multi-planar computed tomography (CT) scan of the cervical spine, which defined injury morphology and was obtained an average of 4.1 h after trauma. 22 Multi-planar, multi-sequence MRI of the cervical spine defined IMLL and presence or absence of hematomyelia and was obtained within an average of 8.4 h after trauma. 14,22 Close to 83% of our cohort had surgical intervention and 17% non-operative management of their traumatic cervical spinal cord injury (tCSCI). The next step was management at the intensive care unit and in preparation for discharge to a rehabilitation facility. 11
Statistical analysis
Data were first evaluated for missingness and presence of outliers, and then described using mean and standard deviation (SD), median and interquartile range, or counts and percentages. We displayed mean values and proportions over the study period graphically.
Time trends for all variables of interest were tested in separate models. We used Poisson regression with an offset for the annual population for binary variables and linear regression for continuous variables. To determine whether observed time trends were independent of trends in demographic and injury-related characteristics, we adjusted individual models with variables that demonstrated significant change over time. The Institutional Review Board of the University of Maryland (Baltimore, MD) approved this study. All analyses were performed using Stata software (version 15; StataCorp LP, College Station, TX).
Results
From 2001 to 2018 in the state of Maryland, 338,922 patients ≥15 years of age sustained trauma, of which 111,346 (32.8%) patients were managed at this Level I trauma center. Considering ICD-9 and ICD-10 codes (see above) as selection criteria, 2076 of 111,346 (1.86%) patients had tCSCI. Detailed review of demographics, etiology, AMS, ISNCSCI, CT, and MRI of these subjects, however, resulted in the exclusion of 656 (31.6%) patients: 205 patients with no evidence of tCSCI on MRI images; 288 patients whose management was primarily based on admission CT scan of cervical spine without obtaining MRI; 142 patients with no documented clinical or imaging studies; 17 patients whose spinal cord signal change was either of bad quality or was attributable to pathologies other than tCSCI, including tumors, discitis, spinal cord vascular malformation, ischemic transverse myelitis, or presence of a syrinx. Additionally, 4 patients had duplicate records. The final sample included 1420 patients with proven MRI tCSCI, as confirmed by two raters (B.A. and K.S.; Tables 1 and 2).
Characteristics of Cervical Traumatic Spinal Cord Injury Patients ≥15 Years of Age and Treated at the R Adams Cowley Shock Trauma Center 2001–2018, n = 1420
AIS, American Spinal Injury Association Impairment Scale; CT, computed tomography; MRI, magnetic resonance imaging; SD, standard deviation.
Adjusted 18-Year Time Trends among Traumatic Cervical Spinal Cord Injury Patients, 2001–2018, n = 1420
Expected value for models 1 and 2, rate ratio for models 3 and 4. 2
AMS, American Spinal Cord Injury Association motor score; MVC, motor vehicle collision; tCSCI, traumatic cervical spinal cord injury.
Demographics
Of the 1420 patients, 1112 (78.3%) were male and 308 (21.7%) were female. Over 18 years, the time trend of sex did not change significantly.
Age
Mean age of patients in 2001 was 43.7 years and in 2018 was 57.3. Time-trend change for age >18 years was significant (p < 0.001; Fig. 1).
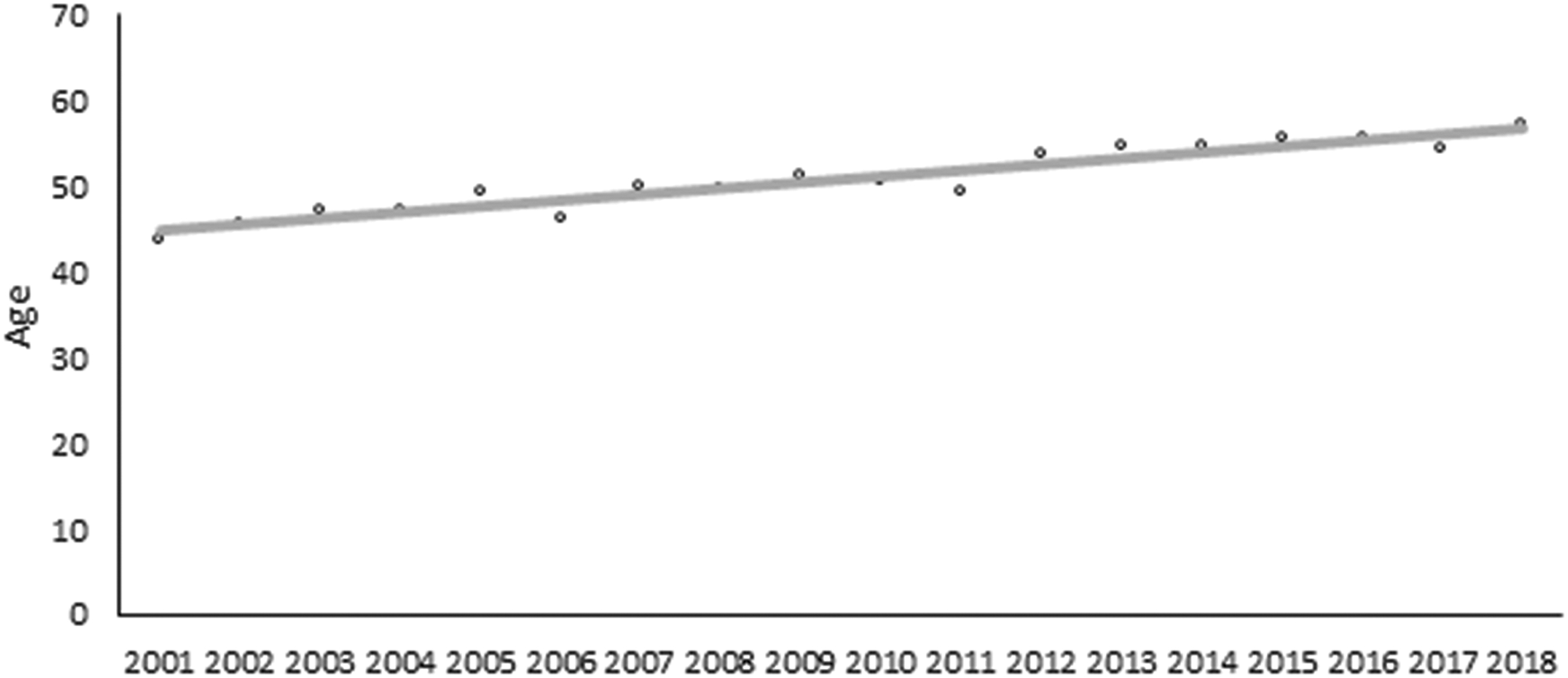
Average age of traumatic cervical spinal cord injury (tCSCI) patients among adult trauma patients treated at the R Adams Cowley Shock Trauma Center 2001–2018, n = 1420; p < 0.001 for increasing trend.
Mechanism
One thousand three hundred six of 1420 (92%) patients suffered tCSCI from three major injury mechanisms: 666 (46.9%) suffered mechanical falls, usually at ground level, 485 (34.2%) motor vehicle collisions (MVCs), and 155 (10.9%) patients sustained tCSCI during sport activities, being either recreational or professional. One hundred fourteen (8%) patients suffered tCSCI from a variety of mechanisms, including violence (69 patients or 4.8%), fall of heavy objects on the head or neck, or penetrating injuries to the neck and cervical spine. The latter included gunshot injuries or penetration by low-velocity sharp objects. From 2001 to 2018, time trend for mechanical falls significantly increased (p < 0.001) whereas tCSCI from MVCs and sport injuries had a downward trend course (p < 0.001 and p = 0.001, respectively; Fig. 2).
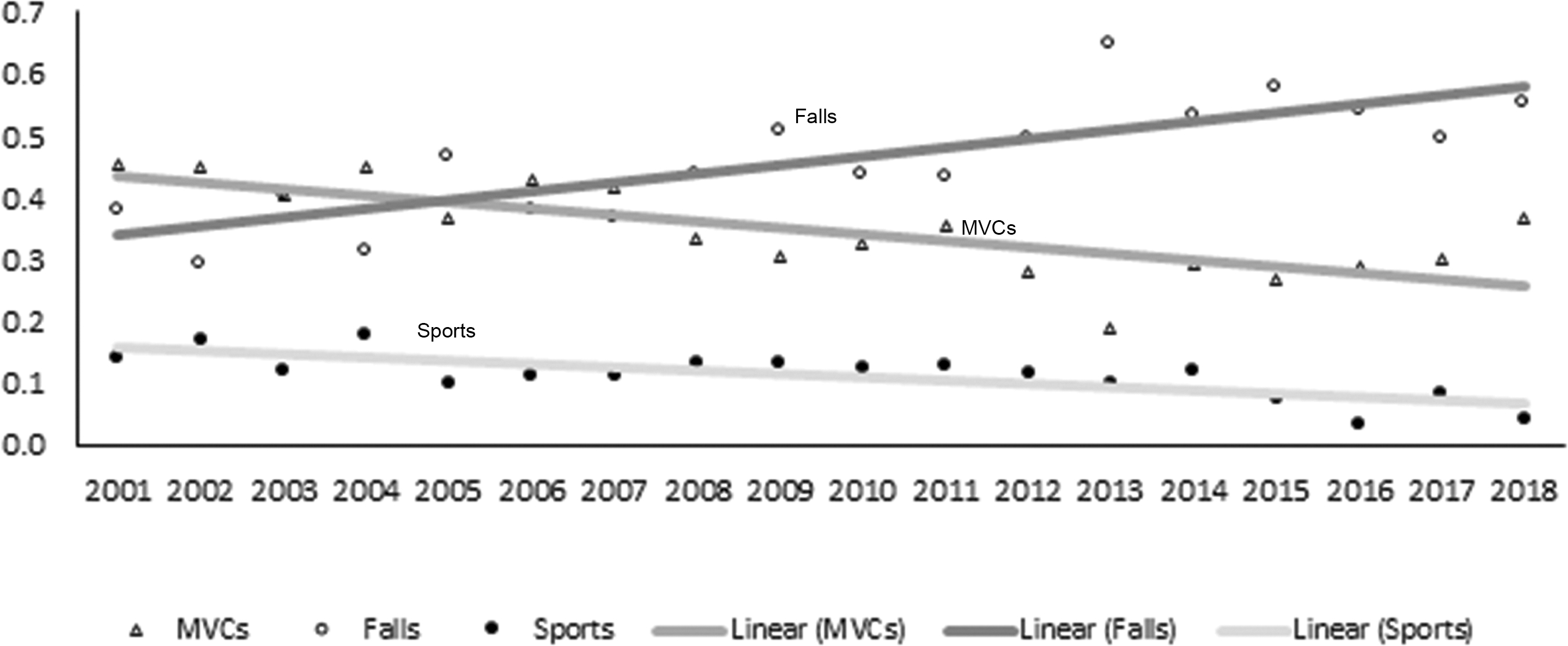
Proportion of traumatic cervical spinal cord injuries (tCSCIs) attributable to different injury mechanisms among adult trauma patients treated at the R Adams Cowley Shock Trauma Center 2001–2018, n = 1420; p < 0.001, increasing trend falls; p < 0.001, decreasing trend MVC; p = 0.001, decreasing trend sports.
American Spinal Injury Association Motor Score and American Spinal Injury Association Impairment Scale grade
An ISNCSCI instrument was used to determine neurological injury severity among patients who were referred to the University of Maryland after tCSCI. 24,25 AMS was not testable in 71 patients. Altered mental state at the time of admission, frequently attributable to associated traumatic brain injury, rendered determination of motor score not testable (NT) in 51 patients. In this group, Glasgow Coma Scale (GCS) score was 4.1 (range, 3–12) in 44 patients, and in 7 patients GCS score was not documented. AMS was not documented in 14 patients, and in 5 patients fractured extremities with or without external fixation precluded the exact determination of AMS. Additionally, 1 patient had Alzheimer's dementia with NT AMS. AIS grade could not be determined in 39 cases. Altered mental state was noted in 39 patients: GCS was 3.5 (range, 3–7) in 36, not documented in 3, and 1 patients suffered from Alzheimer's dementia. As such, median AMS among 1359 patients was 47 (SD, 36.1; range, 0–100). Motor score in 404 complete tCSCI patients was 10.2 (SD, 11.1; range, 0–50; NT in 5) and in 945 incomplete tCSCI patients was 62.8 (SD, 31.4; range, 0–100; NT in 66). There was a significant increase in AMS >18 years (p = 0.008) and a significant (p < 0.001) decline in the proportion of complete tCSCI patients and increase in the proportion of incomplete tCSCI patients, which remained significant with adjustment for other significant variables (Figs. 3 and 4).
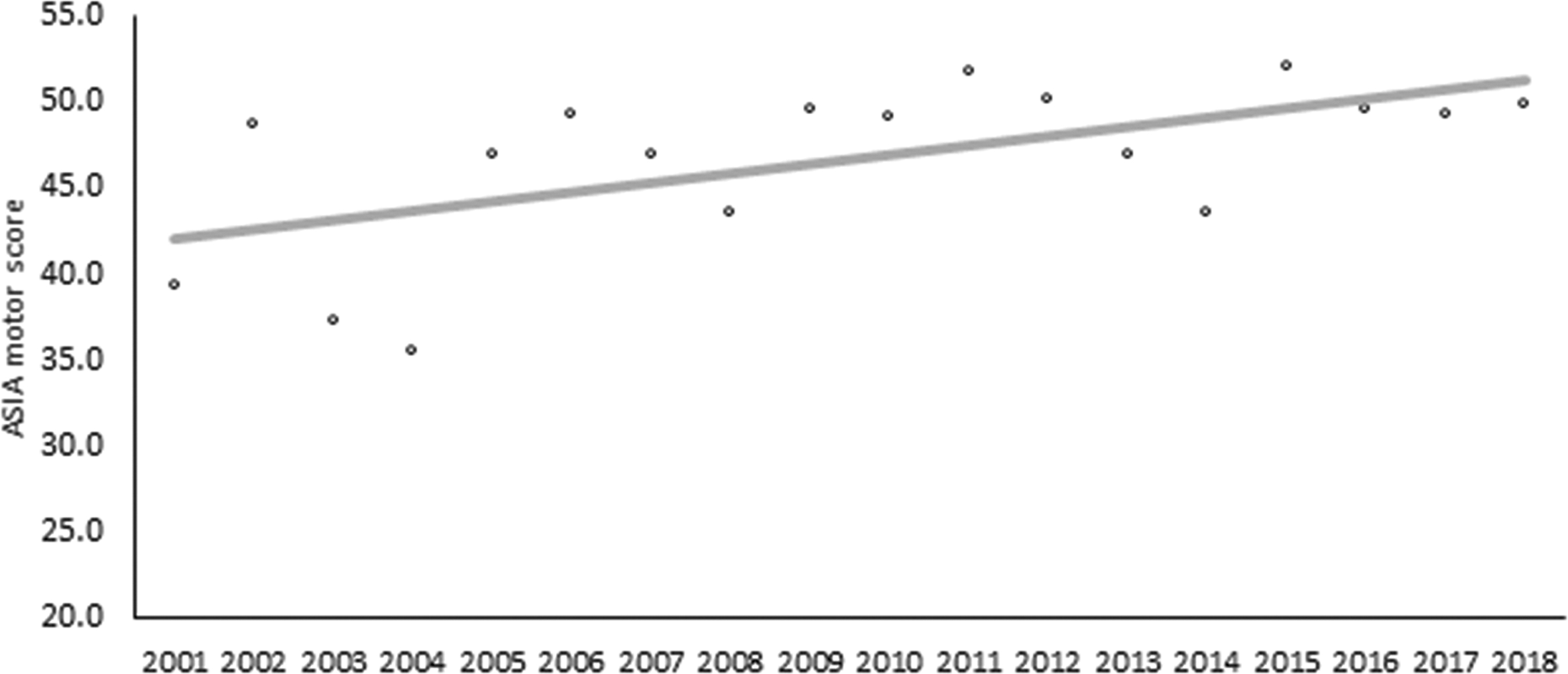
Mean ASIA Motor Score (AMS) among traumatic cervical spinal cord injury (tCSCI) patients referred to the R Adams Cowley Shock Trauma Center 2001–2018, n = 1420. p = 0.008 for increasing trend. ASIA, American Spinal Cord Injury Association.
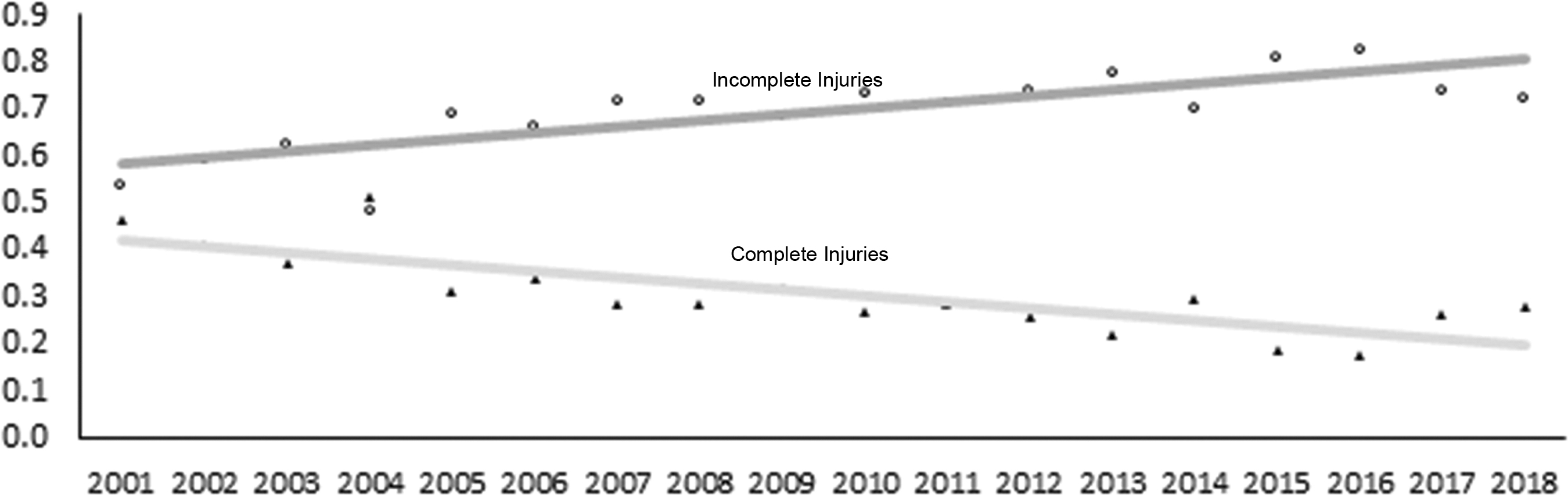
Proportion of traumatic cervical spinal cord Injury (tCSCI) patients referred to the R Adams Cowley Shock Trauma Center with incomplete and complete injury 2001–2018, n = 1420; p < 0.001 for trends.
Anatomical level of injury
tCSCI segments are primarily centered in the middle (C3–C6), followed by lower (C6–T1) and upper (C1-C3) cervical spine. National Spinal Cord Injury Statistical Center studies have indicated that over the past 40 years, there has been a significant increase in the proportion of upper cervical tCSCI patients. 15,26 At our center, injuries were confined to the upper cervical spine in 115 (8.1%), middle in 956 (67.9%), and lower in 291 (24%) patients. Fifty-eight of 1420 patients had injuries at more than one spinal cord injury segment. There was no significant increase in the proportion of upper cervical spine injury patients over an 18-year follow-up.
Injury morphology
Clinical and scientific applicability of injury morphology in tCSCI is to determine the degree of structural instability and the direction of vector force at the time of trauma. These principals have helped investigators to classify injury morphology. 27 –30 Mechanistic classifications of traumatic cervical spine and SCI have considered horizontal and vertical translation as indicators of injury severity. 28,31,32 The latest AOSpine subaxial cervical spine injury classification system has suggested horizontal and/or vertical translation as hallmarks of force and injury severity at the time of trauma, given that such fracture dislocations (Fig. 5) have sustained more devastating injury than injuries not associated with fracture dislocations. 33,34
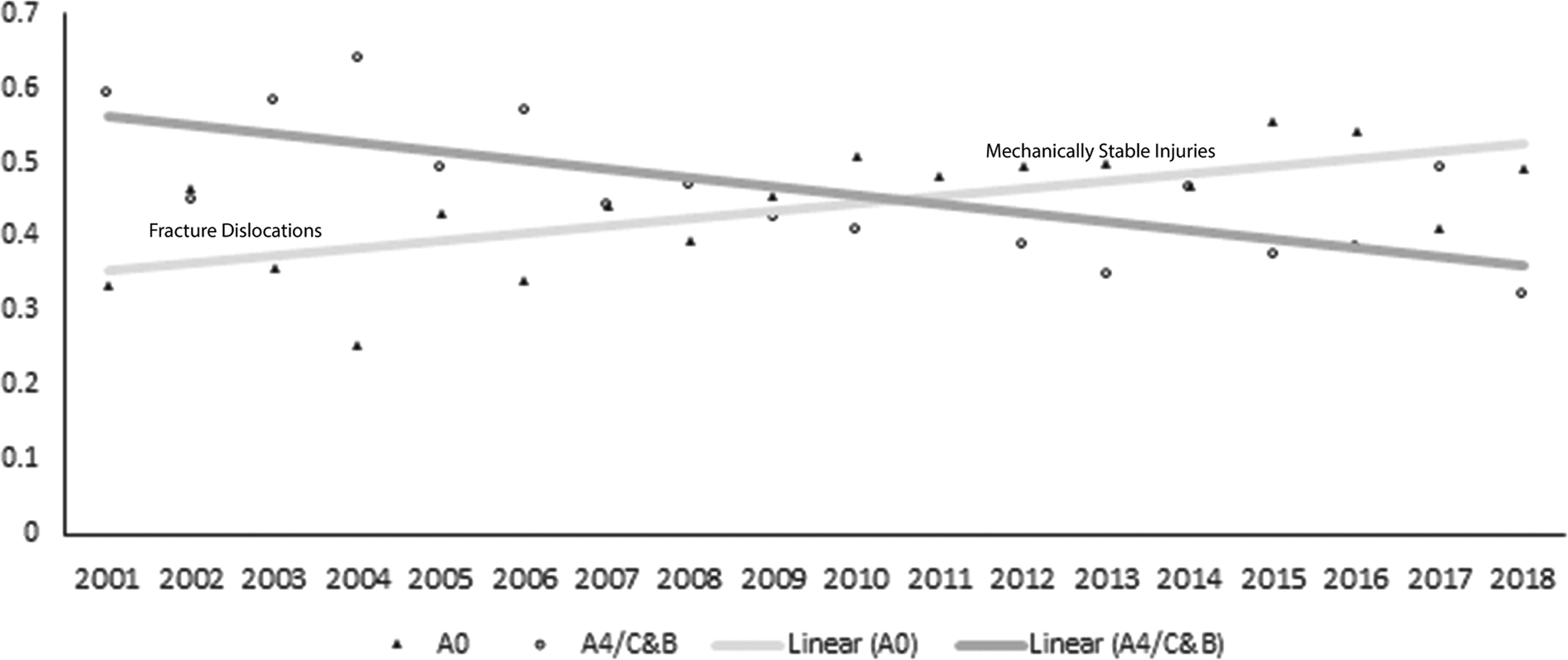
Evidence of fracture dislocation (A4/C and B) among traumatic cervical spinal cord injury (tCSCI) patients referred to the R Adams Cowley Shock Trauma Center 2001–2018, n = 1420; p = 0.007, increasing trend A0; p < 0.001, decreasing trend A4/C and B.
In the present study, 634 of 1420 (44.7%) patients with tCSCI had radiographical evidence of injury to the boney spine and discoligamentous complex and 786 (55.3%) patients presented with CT and MRI indications of fractured spine and disruption of discoligamentous complex (Fig. 6). Time-trend analysis indicated a gradual and significant increase in the proportion of injuries with no fracture dislocation and a decline in injuries with fracture dislocation.
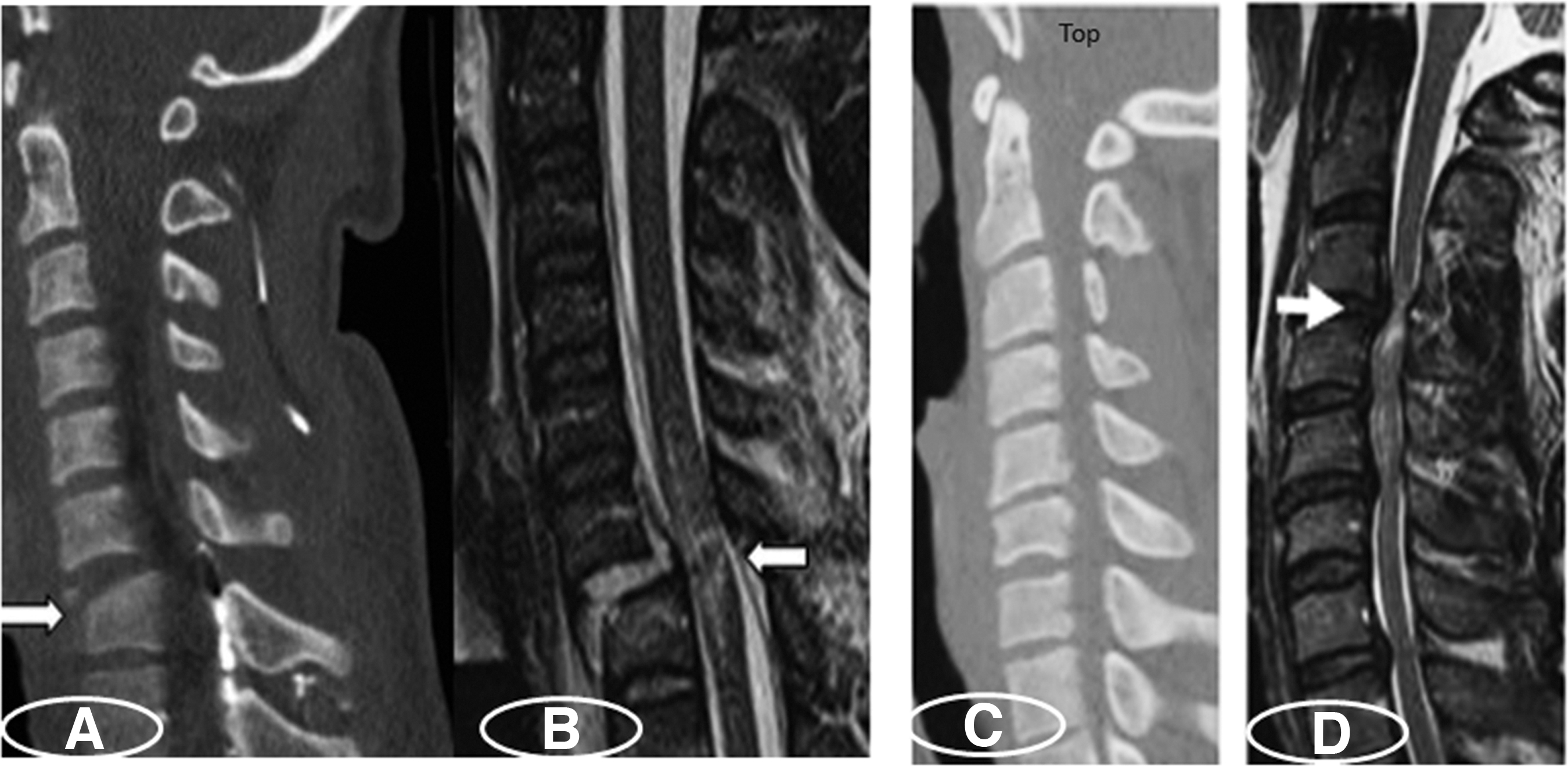
Midsagittal CT and MRI views of a teardrop fracture dislocation (plates
Magnetic resonance imaging markers of injury severity
Evidence supports a relationship between intramedullary lesion length, AMS, and AIS grade. 14,35,36 On T2-weighted (T2W) and short tau inversion recovery (STIR) images, motor-complete tCSCI patients have longer IMLL than motor incomplete subjects. 14 Similarly, as the AMS drops, the IMLL increases and there is increased probability of concomitant hematomyelia. 35,37 Mean IMLL among 1399 verifiable tCSCI patients who were referred to the trauma center was 36.0 mm (SD, 22.9). Among those with complete tCSCI, mean IMLL was 56.3 mm (SD, 25.2) and mean IMLL in incomplete injuries was 27.4 mm (SD, 15.4). A high percentage of complete tCSCI patients had indication of hematomyelia in pre- or post-operative T2W and STIR MRI images. 35,38 In our study, 479 (34.3%) patients with tCSCI indicated evidence of hematomyelia on pre- or post-operative MRI studies. There was an insignificant time-trend decrease in IMLL and incidence of hematomyelia among patients who were admitted to the trauma center with tCSCI (Fig. 7).
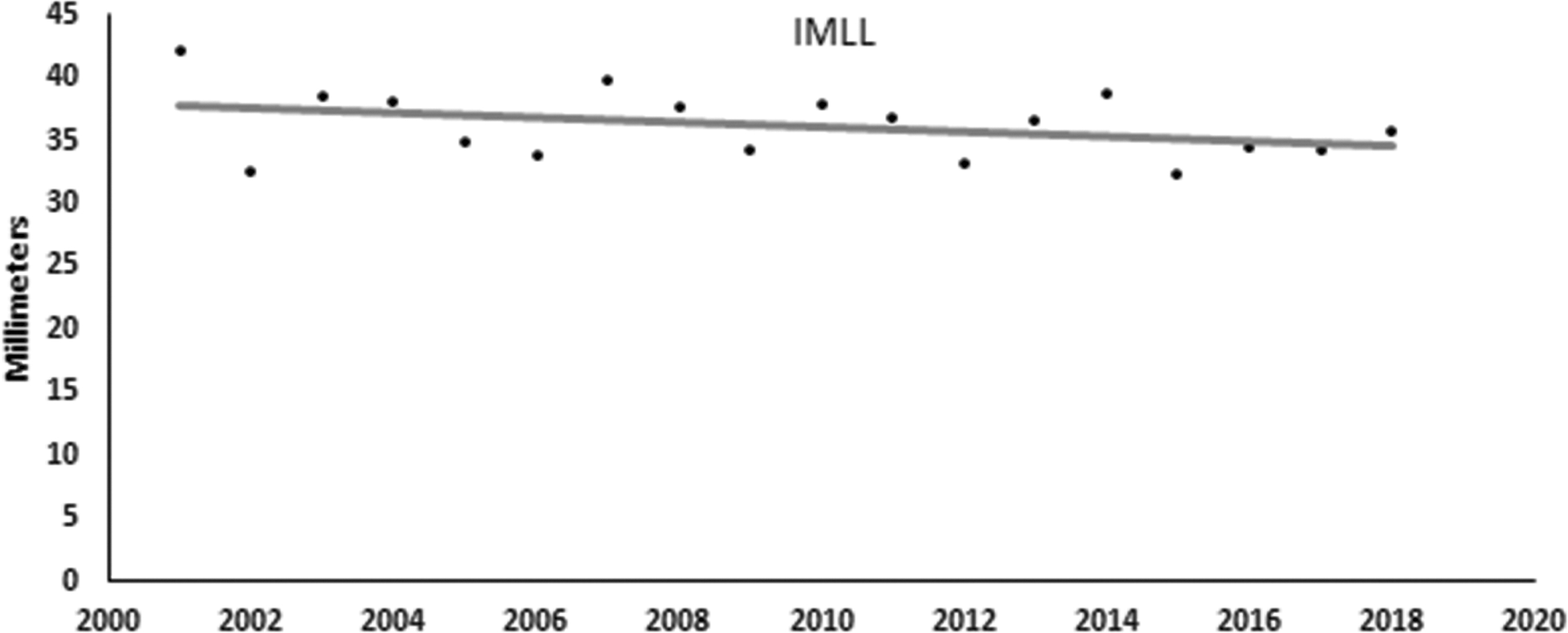
Mean intramedullary lesion length (IMLL) among cervical spinal cord injury patients referred to the R Adams Cowley Shock Trauma Center 2001–2018. n = 1399; p = 0.17.
Hospital length of stay and acute care mortality
Mean hospital length of stay in this study was 16.4 days (SD, 16.7). There was a significant increase in hospital length of stay >18 years (p = 0.03), possibly an indication of increased admission of older patients with higher comorbidities. One hundred twenty-four of 1420 (8.7%) patients died with no significant trend in acute care mortality.
Discussion
Evidence presented here indicates that over the past 18 years, there has been a major shift in the epidemiology of tCSCI. There are now fewer younger patients with catastrophic fracture dislocations and complete injuries and more older victims with incomplete tCSCI. Additionally, we found a decrease in motor vehicle accidents and an increase in ground-level falls involving older persons. The present epidemiological trends have significant implications for management and research in tCSCI. On the one hand, an understanding of recent and ongoing demographic trends in tCSCI can help guide more-effective medical, 39 surgical, 22 and rehabilitative management. 40 On the other hand, knowledge of these trends can help fine-tune preventive measures, including public education, safety standards, and innovations in the transportation industries, and multi-dimensional assessment of the factors precipitating common injury mechanisms (e.g., ground-level falls in the elderly). 41 –48
Over the past three decades, and with the support of several other pre-clinical studies, 49 –55 neurosurgeons and orthopedic surgeons have viewed “decompressive” surgery as a neuroprotective measure, especially in the setting of motor-complete tCSCI. As a consequence, early surgery has been recommended not only to facilitate further patient care and early rehabilitation, but also as a means to promote upward AIS grade conversion. 11,39,56 –61 Besides attention to timing of surgery, more-recent clinical research has recognized the importance of the specific surgical technique utilized. In addition to reduction and internal fixation, several studies have indicated that full (circumferential) decompression of the injured spinal cord, as confirmed by post-operative MRI, may yield enhanced recovery of neurological function. 14,22
In contrast to fracture-dislocation injuries, which are motor complete and for which there has generally been less controversy, tCSCI without fracture dislocation has posed multiple dilemmas for surgeons over the past half century, since Dr. Schneider's original description of the clinical syndrome of acute traumatic central cord syndrome. 17,62 These dilemmas continue to include, but are not limited to, operative versus non-operative management, optimal timing of surgery, operative technique, and extent of spinal cord decompression. 61,63 –69 That these questions remain unsettled at present is attributable largely to the fact that the overwhelming majority of these patients exhibit modest clinical improvement when managed according to several different strategies. 70,71 Against this background, it is noteworthy that nearly 58% of incomplete tCSCI patients in the present study (561 of 972, excluding 39 AIS non-testable) lacked fracture-dislocation morphology, indicating that if the trends of the past two decades continue, surgeons will encounter increasing numbers of patients for whom the standard of care remains a matter of ongoing debate. 69 That surgeons can anticipate older tCSCI patients with more medical comorbidities will, by itself, influence these debates. Older patients may not have the “reserve” of younger patients and are more likely to experience surgical complications.
Decisions regarding surgical technique will also have to consider that an increasing number of these patients will have underlying degenerative spinal stenosis with associated buckling of the ligamentum flavum and/or disc-osteophyte complexes. In these cases, an already-compromised spinal milieu will contribute to patterns of injury presentation and recovery, whereas age-associated changes of the cervical spine can sometimes markedly increase the difficulty and duration of surgery and the risk of perioperative complications. The increasing number of incomplete tCSCI patients who will likely fit this clinical picture makes the resolution of unsettled management questions more pressing. One of the unexpected findings of the present study was the slight decline in IMLL >18 years, which was not statistically significant (p = 0.17; Fig. 7). Several possible explanations present themselves. That improved AMS at time of admission over an 18-year period could be the result of improved pre-hospital resuscitation measures, which are not reflected in the IMLL. The IMLL may be a non-specific imaging marker of injury severity at the time of admission, even though longer admission IMLL values in AIS grades A and B patients are associated with less likelihood of AIS grade conversion at 6 months after trauma. Further research is warranted to clarify this unexpected finding on the IMLL.
Limitations
Because institutional ICD-9 and ICD-10 coding included 656 patients with a questionable diagnosis of tCSCI, a population-level analysis could not be carried out.
Conclusions
From 2001 to 2018, the proportion of cervical spinal cord injuries caused by MVCs and the proportion of complete injuries decreased significantly whereas age, injuries attributable to falls, and proportion of incomplete tCSCI increased. An increasing proportion of our patients did not show evidence of fracture dislocations. These trends highlight the urgent need for research to establish standard of care for incomplete tCSCI patients. Specifically, research is needed on elderly patient populations in regard to multi-dimensional preventive measures and clinical trials to better define indications, extent, and techniques of surgical intervention in order to maximize motor and functional recovery.
Footnotes
Acknowledgments
We thank Dr. Patricia Stephens for her editorial assistance.
Authors' Contributions
B. Aarabi; study concept, writing, overall oversight on data safety. Critical editorial review: Marc Simard, K. Crandall, T. Chryssikos, J. Olexa, J. Oliver, C. Sansur, G. Schwartzbauer, M. Scarboro, C. Diaz Lomangino, B. Howie, N. Caffes, A. Wessell, and G. Cannarsa. MRI IMLL rater: K. Shanmuganathan, B. Aarabi. Statistics: J. Albrecht. Data collection from various resources: M. Gertner, B. Aarabi, C. Diaz Lomangino, M. Scarboro, T. Chryssikos, J. Olexa, J. Oliver, G. Cannarsa, N. Caffes, A. Wessell, and B. Howie.
Funding Information
No funding was appropriated for this study.
Author Disclosure Statement
No competing financial interests exist.