
Abstract
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus attacks multiple organs of coronavirus disease 2019 (COVID-19) patients, including the brain. There are worldwide descriptions of neurological deficits in COVID-19 patients. Central nervous system (CNS) symptoms can be present early in the course of the disease. As many as 55% of hospitalized COVID-19 patients have been reported to have neurological disturbances three months after infection by SARS-CoV-2. The mutability of the SARS-COV-2 virus and its potential to directly affect the CNS highlight the urgency of developing technology to diagnose, manage, and treat brain injury in COVID-19 patients. The pathobiology of CNS infection by SARS-CoV-2 and the associated neurological sequelae of this infection remain poorly understood. In this review, we outline the rationale for the use of blood biomarkers (BBs) for diagnosis of brain injury in COVID-19 patients, the research needed to incorporate their use into clinical practice, and the improvements in patient management and outcomes that can result. BBs of brain injury could potentially provide tools for detection of brain injury in COVID-19 patients. Elevations of BBs have been reported in cerebrospinal fluid (CSF) and blood of COVID-19 patients. BB proteins have been analyzed in CSF to detect CNS involvement in patients with infectious diseases, including human immunodeficiency virus and tuberculous meningitis. BBs are approved by the U.S. Food and Drug Administration for diagnosis of mild versus moderate traumatic brain injury and have identified brain injury after stroke, cardiac arrest, hypoxia, and epilepsy. BBs, integrated with other diagnostic tools, could enhance understanding of viral mechanisms of brain injury, predict severity of neurological deficits, guide triage of patients and assignment to appropriate medical pathways, and assess efficacy of therapeutic interventions in COVID-19 patients.
Introduction
Infection by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) coronavirus results in significant mortality and long-term disability. Global costs of coronavirus disease 2019 (COVID-19) are predicted to reach as much $35.3 trillion through 2025. 1 The full spectrum of disease associated with COVID-19 is not yet fully characterized, yet 35% of adult COVID-19 patients report they have not returned to their usual state of health 2–3 weeks after testing positive for the SARS-CoV-2 virus. 2 Emerging data indicate the presence of brain injury in a subset of COVID-19 patients, consistent with the known ability of coronaviruses to infect the CNS. However, the clinical manifestations, frequency of CNS effects, and associated primary or secondary mechanisms underlying neurological injury produced by SARS-CoV-2 infection are not well understood.
Human coronaviruses have been described as underestimated opportunistic pathogens of the CNS. 3 The SARS-CoV-2 virus, like many viruses including coronaviruses related to SARS-CoV-2, attacks multiple organs of COVID-19 patients, including the brain. There have been worldwide reports of neurological deficits in COVID-19 patients involving both the central and peripheral nervous systems. However, the pathobiology of CNS infection by SARS-CoV-2 and the associated neurological sequelae of this infection remain poorly understood. A central question is whether or not brain damage in individual patients results from a direct primary effect of the virus on the brain or results indirectly from systemic secondary insults, including hypoxemia, thrombosis, or autoimmune responses. In this review, we outline the rationale for the use of BBs for diagnosis of brain injury in COVID-19 patients, the research needed to incorporate their use into clinical practice, and the improvements in patient management and outcome that can result.
BBs have been successfully used in other acute and chronic brain diseases. Timely implementation of BBs in the current SARS-CoV-2 pandemic will also allow this emerging technology to provide critically needed insights into the risk factors associated with SARS-CoV-2 neurological involvement and the potential for increased risks for long-term neurological deficits and neurodegenerative diseases.
Injury to the peripheral nervous system (PNS) has also been reported in COVID-19 patients. 4 –7 However, in contrast to studies of biomarkers of CNS injury, there is currently an absence of reliable biomarkers of PNS injury. 8 Thus, we have focused on the clinical and research advantages of using BBs in conjunction with other diagnostic tools to provide a better understanding of CNS brain injury associated with SARS-CoV-2 and, potentially, with its ongoing mutations.
Viral mutations present an especially worrisome challenge to responses to infection by the SARS-CoV-2 virus. There are 219 viruses currently known to be capable of infecting humans, and microbes continuously mutate to enhance their capabilities for human infection. The mutation spike D614G in SARS-CoV-2 has been described as “of urgent concern” given that it represents the emergence of a dominant and more transmissible form of the virus. Some investigators have reported that the spike protein D614G and RdRp P323L mutations in SARS-CoV-2 are associated with severity of COVID-19. 9 Other data show that, over the course of only a month, the variant carrying the more infectious D614G spike mutation became the globally dominant form of SARS-CoV-2. D614G is associated with potentially higher viral loads in COVID-19 patients, but not injury severity. 9 Similar observations were made in Houston, Texas. Between the first wave of infection in April 2020 and the second wave in June 2020, the more infectious, but not more virulent, D614G mutation increased from 71% to 99.9% of infections, completing its domination of this local outbreak. 10
Secondary infections have been reported internationally. A case report documented reinfection by a variant of the SARS-CoV-2 that had significantly different genomic sequences from the variant causing the first infection.
11,12
Significantly, the SARS-CoV-2 reinfection resulted in a worse disease progression than the first infection. In addition, a prevalent Eurasian avian-like H1N1 swine influenza virus possesses 2009 pandemic genes facilitating human infection.
13
The mutability of SARS-CoV-2 has prompted investigators to speculate that the virus will be a permanent addition to viruses that can infect humans (e.g.,
The mutability of the spike protein and its potential for rapid spread should alert scientists and public health experts to the possible appearance of spike mutations favoring CNS infection given that sequestration in the CNS confers survival advantages by protecting viruses from systemic immune responses. An analysis pipeline has been developed to facilitate real-time mutation tracking in SARS-CoV-2, focusing initially on the spike protein because it mediates infection of human cells and is the target of most vaccine strategies and antibody-based therapeutics. 14 To date, the pipeline has identified 14 mutations in spike that are accumulating. Such mutations, considered in a broader phylogenetic context, provide an early warning system to reveal mutations that may confer selective advantages in transmission or resistance to interventions. Each mutation is evaluated for evidence of positive selection, and the implications of the mutation are explored through structural modeling. We encourage, where possible, the screening and evaluation process to include assessments of the potential of spike protein mutations to favor CNS infection. Fortunately, the technology we propose here has the potential for detecting CNS damage resulting from any viral infection.
Clinical Presentations
Although the novel SARS-CoV-2 virus is primarily associated with respiratory problems, investigators are becoming increasingly aware of extrapulmonary complications of COVID-19, including CNS pathologies 15 (for recent reviews, see previous works 16 –19 ). Table 1A summarizes international reports of neurological symptoms, and Table 1B summarizes pathological observations in COVID-19 patients, as of September 2020.
CNS Injury in COVID-19 Patients A. CNS Injury in COVID-19 Patients: Neurological Manifestations
B. CNS Injury in COVID-19 Patients: Cerebrovascular and Other Neuropathological Observations
Percentage calculated from the total number of patients with a specific disorder, symptom, or neuroimaging finding.
Timing of neurological disorders missing in 7 patients.
ADEM, acute disseminated encephalomyelitis; ARDS, acute respiratory distress syndrome; CAM-ICU, confusion assessment method in the intensive care unit; CNS, central nervous system; COVID-19, coronavirus disease 2019; CSF, cerebrospinal fluid; CT, computed tomography; EEG, electroencephalography; EMG, electromyography; GMV, gray matter volume; ICH, intracerebral hemorrhage; ICU, intensive care unit; IVH, intraventricular hemorrhage; MRI, magnetic resonance imaging; NIHSS, the National Institutes of Health Stroke Scale; PTSD, post-traumatic stress disorder; RT-PCR, reverse-transcription polymerase chain reaction; SAH, subarachnoid hemorrhage; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TIA, transient ischemic attack.
Early communications from China provided data on neurological symptoms suggesting CNS involvement in COVID-19 patients 4 now confirmed in several other studies. 4,23,25,27,29,30,40,72 Disturbances in taste and smell have been prominent neurological sequelae of COVID-19 infection, 56 but neurological symptoms can also include descriptions of impaired consciousness and confusion, altered mental status, confusion, headache, and syncope as well as anxiety, depression, and post-traumatic stress disorder (PTSD). 7,57 Neurological manifestations have been observed in 42% of COVID-19 patients at disease onset, 63% during hospitalization, and 82% at some time during the course of the disease. 24 In contrast, a prospective study of hospitalized COVID-19 patients reported that 13.5% developed new neurological symptoms before or during hospitalization with a median onset of 2 days from COVID-19 symptoms onset. 20 These data signal the importance of standardizing the evaluation of neurological assessments across study sites and, where possible, linking behavioral observations to organically based assessments such as BBs and imaging.
There are also multiple descriptions of CNS pathological observations that include a predominance of reports of cerebrovascular injury, such as diffuse cerebral ischemia, ischemic and hemorrhagic stroke, microhemorrhages, white matter microangiopathy, and arterial thrombosis as well as meningitis, encephalitis, acute transverse myelitis (ATM), and encephalopathy 4,20,23,24,27,29,30,39,40,67,70,72,76,90,100,102,103,109,123 –126 (see also other works 24,69,121,127 –132 ). Investigators have also observed associations between magnetic resonance (MRI) abnormalities and neurological deficits persisting in 55% of hospitalized patients 3 months after disease onset. 28
Hypercoagulopathy resulting from viral effects on systemic and CNS coagulation pathways has been a growing concern, and anticoagulant administration was reported to be associated with decreased mortality in COVID-19 patients. 133 There is also a case report of an ischemic stroke in a COVID-19 patient even though no viral particles were detected in the cerebrospinal fluid (CSF), suggesting the possibility that peripheral hypercoagulopathies could contribute to stroke in these patients. 30
Brain hypoxia may be another prominent contributor to CNS injury, especially in patients presenting with significant pulmonary symptoms and having experienced prolonged periods of ventilator support or even extracorporeal membrane oxygenation (ECMO). “Silent hypoxemia,” oxygen levels incompatible with life without dyspnea in COVIR-19 patients, has been of concern as well, in spite of difficulties in conducting reliable assessments using pulse oximetry. 134 Post-mortem histopathological examination of brain specimens obtained from 18 patients showed only hypoxic changes and did not detect encephalitis or other specific brain changes referable to the virus. 121 There was no cytoplasmic viral staining, but the virus was detected at low levels in six brain sections obtained from 5 patients who were not consistently related to the interval from the onset of symptoms to death. However, the broad diagnostic categories, variability in the times of post-mortem examinations, and limited number of observations limit the generalizability of these data.
Collectively, these cases document that the CNS is among the multiple organs targeted by SARS-CoV-2. Characterization of cerebrovascular pathologies and potentially related systemic hypercoagulopathies that occur in severe COVID-19 cases are especially needed, 64 as is a clearer understanding of the nature of persistent neurological deficits and their relationships to disease severity and epidemiological factors. In addition, longitudinal studies of affected patients should enable detection of later-emerging neurological symptoms.
The Potential for SARS-CoV-2 to Increase Risks for Neurological Deficits and Neurodegenerative Diseases: The Need for Improved Diagnostic Rigor and Outcome Assessments
As reviewed in preceding sections and tables, a number of studies have provided evidence of CNS consequences of infection by SARS-COV-2, either by inferences from changes in neurological status or by more direct neuropathological assessments such as imaging. Studies to date have primarily been observational and used differing criteria for reporting CNS injury. For example, altered mental status is commonly used as a sign of possible CNS injury in COVID-19 patients (e.g., see earlier works 102,103,135,136 ). However, functional neurological assessments can be non-specific, and neurological symptoms attributable to SARS-CoV-2 infection must be distinguished from exacerbation of pre-existing neurological and psychiatric conditions, especially in the elderly. 137,138 Moreover, CNS pathology may not be reliably related to the severity of respiratory symptoms in COVID-19 patients. 67 Methods to enable accurate prognoses of patients' vulnerability to neurological disturbances as well as the extent and durations of cognitive and functional deficits attributable to infection by SARS-CoV-2 are urgently needed.
The most urgent unanswered questions relate to the frequency and severity of brain injury in COVID-19 patients, identification of primary and secondary injury mechanisms contributing to this injury, risk factors for injury, and the nature and duration of neurological deficits in COVID-19 patients diagnosed with brain damage. Investigators have initiated important retrospective studies to begin to address these questions. 139 The researchers felt, based in part on extrapolation from previous data from severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), that neurological complications in COVID-19 patients are infrequent. However, given potential that 50–80% of the world's population might be infected before herd immunity develops, they recognized the significant need for clinical, diagnostic, and epidemiological studies to characterize neurological manifestations in COVID-19 patients and the resulting disease burden.
We argue that conclusions about the frequency and severity of CNS injury and resulting neurological deficits are premature in the absence of established diagnostic and outcome measures. Our goal is to provide a framework in which such studies can be rapidly implemented to provide these much needed data. As we reference in this review, the framework incorporates technologies and clinical approaches previously successfully used in studies of other acute CNS injuries, notably TBI.
Does infection with SARS-CoV-2 increase risk for later emergence of new neurological symptoms or development of neurodegenerative diseases? Cell senescence and a stable state of proliferative arrest is an adaptive response to viral infections, 140 and investigators have posited that SARS-CoV-2 invokes CNS cellular senescence and neurodegenerative processes. 141 Inflammatory and neuroimmune responses to CNS infection are thought to be important mediators of Alzheimer's disease (AD). 142 “Cytokine storms” and immunosuppression have both been reported to occur during the course of COVID-19. 143 However, levels of inflammatory markers in COVID-19 patients may be lower than levels observed in secondary insults such as acute respiratory distress syndrome (ARDS) that could be associated with SARS-CoV-2 infection. 144
The interleukin (IL)-6 inhibitor, tocilizumab, reduces cognitive deficits in a mouse model of AD, 145 and IL-6 inhibitors are being studied in clinical trials for their efficacy in treating severe SARS-CoV-2 disease. 143 Long-term follow-up of these patients will enhance understanding of the role of IL-6 and SARS-CoV-2 in any subsequent neurodegeneration. The hypothesis that initiation of AD could be attributable, in part, to systemic pathogens entering the CNS and initiating aberrant A-beta cascades 146 or stimulating inflammation that facilitates the cascades highlights the need for such studies. There is an interesting reciprocity between COVID-19 and dementia and neurodegenerative diseases. As we document in a later section of this review, AD, Parkinson's disease (PD), and dementias are associated with more complicated clinical courses and poorer outcomes in COVID-19 patients.
Mechanisms of Central Nervous System Injury by Coronaviruses
Viral infection of the CNS enables the pathogen to evade a response from the systemic immune systems of the host. 113 Numerous viruses, including the coronaviruses, are known to have CNS involvement and cause brain injury after infection. 147 –149 For example, human immunodeficiency virus-1, a lentiviris, 150 and herpes simplex virus-1, a simplexvirus, 151 produce CNS pathologies. In fact, five neuroinvasive arboviruses have been identified as emerging potential public health threats in the United States. 152 Zika, a flavivirus, is especially likely to cause Guillain-Barre syndrome. Chikungunya, an alphavirus, is more likely to cause inflammation and swelling in the brain (encephalitis) and spinal cord (myelitis). However, stroke, which could be caused by either virus alone, is more likely to occur in patients infected with the two viruses together. 153
Recent studies suggest a direct CNS mechanism contributing to neurological symptoms produced by the SARS-CoV-2 virus. 154 SARS-CoV-2, but not SARS-CoV, can infect and replicate in induced pluripotent stem cells (iPSCs)-derived human neural progenitor cells (hNPCs) and in neurospheres and brain organoids produced from these cells. Studies with the neurospheres showed that the virus is alive and able to replicate within the brain cells. The brain organoids showed morphology that was similar to developing human cerebral cortex, and this experiment showed the potential of the virus to interfere with neurogenesis. The organoids were positive for neuron-specific class III beta-tubulin (TUJ1), a marker for neuronal cells, paired box 6 (PAX6), a marker for radial glial cells, and nestin (NES), a marker of proliferation for neural progenitor cells. Brain cells have the angiotensin-converting enzyme 2 (ACE2) receptors, transmembrane serine protease 2 (TMPRSS2), cathepsin L, and furin, all of which have been identified as important for the process of infection with SARS-CoV-2 (see Zhang and colleagues 2020, supplemental material). Other investigators have confirmed that SARS-CoV-2 targets neurons of three-dimensional human brain organoids. 155 Finally, it is important to remain vigilant to the potential for endogenous retroviruses to contribute to CNS disease. 156,157
The ACE2 receptor plays a role in cell entry of SARs-CoV-2, similar to the other coronaviruses SARS-CoV and MERS-CoV. 158 ACE2 receptors are present in the CNS on neurons, glia, and the cerebrovascular endothelium, the latter being one possible route of entry into the brain. 159 Regional variability in the distribution of ACE2 receptors in the human brain has been reported. The highest ACE2 expression level was detected in the brainstem containing the medullary respiratory centers, an observation that could be relevant to the respiratory distress experienced by many COVID-19 patients. 160 Upregulation of ACE2 in the brain has been linked to oxidative stress, apoptosis, and neuroinflammation leading to neurodegeneration in several brain disorders. 161 Consistent with this possibility, a post-mortem case report detected SARS-CoV-2 viral particles in endothelial cells of the microvasculature of the frontal lobes. 162
A recent case report of a patient with anosmia and confirmed SARS-CoV-2 infection described a hyperdense MRI signal on fluid-attenuated inversion recovery in the olfactory bulb and posterior gyrus rectus, a cortical region associated with olfaction, supporting the hypothesis of virus brain entry through the olfactory pathway. 163 This potential SARS-CoV-2 entry into the CNS through the olfactory bulb is similar to the way SARS-CoV does in mice, although this remains speculative at the present time. 158,164,165
In addition, ACE2 and TMPRSS2 have been reported to be localized to support cells, stem cells and perivascular cells rather than olfactory neurons in mouse, non-human primate, and human olfactory mucosa. 166 Studies detecting SARS-CoV-2 in clinical specimens 167 have shown that the highest viral copy number is found in nasal swabs (∼200-fold), compared to bronchoalveolar lavage or pharyngeal swabs. These findings, taken together with ACE2 protein cellular localization, suggest that active virus infection and replication occur in the apical layer of nasal and olfactory mucosa. The high similarities between SARS-CoV and SARS-CoV-2 has prompted some investigators to posit that the potential invasion of the CNS by SARS-CoV-2 is partially responsible for the acute respiratory failure noted in COVID-19 patients during ICU management. 168 Others, however, suggest a more limited role of CNS involvement in the respiratory failure associated with COVID-19. 169 Regardless, there is a need for additional studies on SARS-CoV-2 effects on the CNS, especially through the olfactory route. 165
Rationale for Studies of Blood Biomarkers for Diagnosis of Central Nervous System Injury: Integration with Existing Diagnostic Tools
Use of blood biomarkers
Consistent with our understanding of evolutionary biology, proteins and cell-signaling pathways underlying CNS injury and cell death following viral infections can be interrogated by blood-based assays of relevant proteins which have already been validated extensively as biomarkers of cell death, acute brain injury and neurodegeneration. Proteins assayed by blood tests assessing mechanisms of CNS cell injury and death are highly conserved across species, including Caenorhabditis elegans, rodents, and humans. Table 2 summarizes human studies of brain injury BBs after systemic infections, including infections by SARS-CoV-2. A recent observational study and limited case reports detected increased CSF and/or plasma levels of glial fibrillary acidic protein (GFAP), neurofilament light polypeptide (NfL), tau, and several inflammatory markers in COVID-19 patients. 100,106,107,170,171 Increased staining of GFAP was also detected in the post-mortem analysis of the brain of a COVID-19 patient. 118 Studies have also reported elevations of BBs in CSF of tuberculous meningitis patients (GFAP, S100 calcium-binding protein [S100B], and neuron-specific enolase [NSE]), 172 –175 HIV patients (NfL, GFAP, and S100B), 176 –180 and cerebral malaria (S100B, NSE, tau proteins, and inflammatory protein markers). 181 –186
Human Studies of Brain Injury and Inflammatory Biomarkers after COVID-19 and Other Systemic Infections
AIDS, acquired immunodeficiency syndrome; ART, antiretroviral therapy; CD, cluster of differentiation; COVID-19, coronavirus disease 2019; CSF, cerebrospinal fluid; CX3CL1, fractalkine, interferon-inducible T-cell α chemoattractant; EDI, estimated date of infection; Fas-L, Fas-ligand; FGF, fibroblast growth factor; G-CSF, granulocyte colony-stimulating factor; GFAP, glial fibrillary acidic protein; GM-CSF, granulocyte-macrophage colony-stimulating factor; HAD, HIV-associated dementia; IFN-γ, interferon-γ; IL, interleukin; IP-10, interferon-γ-induced protein-10; MCP-1, monocyte chemoattractant protein-1; MDC, macrophage-derived chemokine; MIG/CXCL9, monokine induced by γ-interferon/chemokine (C-X-C motif) ligand 9; MIP, macrophage inflammatory protein; MMP-9, matrix metallopeptidase 9; NfL, neurofilament light; NPY, neuropeptide Y; NSE, neuron-specific enolase; PDGF-BB, platelet-derived growth factor; pNfH, phosphorylated neurofilament heavy chain protein; RANTES, regulated on activation, normal T cell expressed and secreted chemokine; S100B, S100 calcium-binding protein B; sCD, soluble cluster of differentiation; SDF-1α, stromal cell-derived factor 1α; sFas, soluble Fas; sTNF-R, soluble TNF receptors; sTREM-1, soluble triggering receptor expressed by myeloid cells 1; suPAR, soluble urokinase-type plasminogen activator receptor; TNF-α, tumor necrosis factor α; VEGF, vascular endothelial growth factor.
Protein biomarkers of CNS damage have also been detected after a variety of acute injury modalities. 193 –201 Elevations of brain injury biomarkers, including GFAP and ubiquitin C-terminal hydrolase L1 (UCH-L1), have been detected in humans and animals acutely after diverse brain injuries, including TBI, 202,203 ischemic/hemorrhagic stroke, 198 cardiac arrest, 204 hypoxia, 196 seizures, 194 and even drug toxicity. 193 Consistent with these observations, high levels of NSE, S100B, GFAP, and other biomarkers (e.g., neurofilament proteins) can be used to support the prognosis of poor neurological outcome after cardiac arrest, as recommended by the American Heart Association (AHA) Guidelines, and in the recent AHA report on standards for prognostication; serial testing is recommended. 197,201 A recent study of 717 patients reported that UCH-L1 and GFAP were optimal BB predictors of outcome as early as 24 h after cardiac arrest. 205 Use of BBs as an adjunct to other diagnostic modalities was recommended. Monitoring of plasma concentrations of GFAP and other brain injury biomarkers, including S100B and NSE, has also been shown to detect brain injury in children on extracorporeal membrane oxygenation (ECMO). 206, 207
Interestingly, serial serum S100B sample analyses demonstrated significant increases in biomarker levels and increasing trajectory in adult ECMO patients developing intracranial lesions. 208 Serial NSE levels were associated with neurological outcomes after cardiopulmonary resuscitation in patients on ECMO. 209 Increased blood levels of NSE and S100B were associated with mortality and poor neurological outcomes in adult patients with accidental hypothermia treated with rewarming and/or extracorporeal life support, including ECMO. 210
BBs are also altered in AD patients. GFAP measured in serum is increased in AD and correlates with cognitive decline. 211 Temporal profiles of serum NfL levels are associated with cognitive decline 212 and can predict clinical progression even in pre-symptomatic AD. 213 At present, levels of BBs of brain injury in COVID-19 patents are unknown. However, recent studies have shown that protein biomarker assays can detect even low levels of UCH-L1, S100B, and GFAP elevated after sport concussion not associated with CNS pathology detectable by computed tomography (CT) scans. 214,215
BBs have yet to be fully exploited for medical management of brain injury. However, as documented in Table 3, research laid the foundation for U.S. Food and Drug Administration (FDA) accelerated approval of measures of UCH-L1 and GFAP for acute diagnosis of TBI not associated with CT abnormalities versus moderate TBI associated with CT abnormalities. This clearance was provided under the FDA's Break-through Devices Program. 216 –218 Studies of BBs potentially assessing brain injury in COVID-19 patients could explore the BBs' previously reported properties, including: quantifying injury magnitude; aiding in outcome prediction; defining the presence of diffuse injury versus mass lesions; assessing injury to different cell types (e.g., neurons vs. glia); assessing subcellular loci of injury (e.g., cell body, axons, myelin sheath, and pre- and post-synaptic structures); tracking contributions from different injury mechanisms and their time courses (e.g., necrosis vs. apoptosis); and detecting secondary insults during patient care. 198,202,203,219 –221
Human Studies of Brain Injury BBs in CNS Disorders and Disorders Associated with Neurological Complications
BDNF, brain-derived neurotrophic factor; CA, cardiac arrest; CCL2, monocyte chemoattractant protein 1/chemokine (C-C motif) ligand 2; CPP, cerebral perfusion pressure; DAI, diffuse axonal injury; ECMO, extracorporeal membrane oxygenation; EPO, erythropoietin; GCS, Glasgow Coma Scale/Score; GFAP, glial fibrillary acidic protein; GFAP-BDP, GFAP breakdown products; HIE, hypoxic-ischemic encephalopathy; ICAM, intercellular adhesion molecule; ICH, intracerebral hemorrhage; ICP, intracranial pressure; IL, interleukin; MDA, malondialdehyde; NIHSS, National Institutes of Health Stroke Scale/Score; NR2, N-methyl-d-aspartate receptor subunit 2; PICU, pediatric intensive care unit; RPB4, DNA-directed RNA polymerase II subunit B4; S100B, S100 calcium-binding protein B; SBDP150, αII-spectrin breakdown product 150 KDa; TGF-1β, transforming growth factor 1β; TH, therapeutic hypothermia; TIA, transient ischemic attack; TNF-α, tumor necrosis factor α; tPA, tissue plasminogen activator; VCAM-1, vascular cell adhesion molecule 1.
Although the clinical utility of BBs for detection of CNS injury is widely recognized, the influence of mechanisms regulating transport of molecules into and out of the brain is poorly understood. Moreover, the literature is often compromised by the assumption that the same processes underlying movement of molecules from the blood to the brain, commonly referred to the blood–brain barrier (BBB), also underlie movement of molecules from the brain to the blood, that is, the BBB, as would be the case for BBs originating in the brain and detected in blood. Some studies further assume that S100B can be a marker of BBB opening even though S100B is also found in peripheral tissue (e.g., a previous work 222 ). More generally, investigations have failed to appreciate the complexity and dynamic qualities of movement of substances between CNS and extra CNS compartments, as highlighted by descriptions of the glymphatic system involved in the removal of molecules from interstitial spaces of the brain. 223 –225 BBB opening after acute injuries such as TBI are biphasic and exhibit acute and chronic phases with different characteristics and mechanisms. 226
A dual role for astrocytes at the BBB has been documented in studies of CNS injury. Astrocytes can mediate either increases or decreases in BBB permeability depending upon the type of injury (for a review, see a previous work 227 ). Even exercise and stress have been reported to open the BBB. 228 –230 A comparison of levels of GFAP and UCH-L1 in rats after experimental TBI found differing levels of the two BBs in CSF versus blood. 231 These data suggest that levels of BBs may result from different transport and/or clearance processes that need to be examined individually for each marker. Similar conclusions were drawn for NSE and S100B in studies conducted in severe TBI patients. 232 The prominent pathology observed in the cerebrovasculature of COVID-19 patients supports the possibility of disruptions of the normal processes regulating exit and entry of molecules into and out of the brain, and studies of these disturbances present promising areas of investigation. As has been done successfully in the past, this research can occur in parallel with studies examining the clinical utility of BBs in COVID-19 patients.
Although not widely appreciated, TBI, stroke and other “acute” brain injuries initiate progressive and evolving pathological events. Similarly, infection by the SARS-CoV-2 virus can initiate pathologies attributable to both the initial insult and secondary injures that can continue for as yet undetermined durations. This progressive pathology is confounded by sustained infection in COVID-19 patients. Thus, we have pointed out the need for serial measurements of BBs in clinical studies given that differing biokinetics of individual markers will produce useful data relevant to understanding the durations of different pathological responses to SARS-CoV-2 and disturbances in processes regulating compartmentalization of molecules originating in the brain.
Integration of Central Nervous System Injury Diagnostic Tools
As in every area of medicine, BBs of brain injury are optimally used in conjunction with other diagnostic tools and can synergistically improve the accuracy and utility of other diagnostic modalities.
Brain imaging
Significant CNS neuroimaging findings have been reported after SARS-CoV-2 infection, including cerebrovascular-related injury, meningitis, and encephalitis (see Table 1). Some CNS abnormalities detected by imaging may be related to intracranial cytokine storms, which may result in BBB breakdown without direct viral invasion or parainfectious demyelination. 143 It will be important to characterize the optimal MRI and CT imaging protocols to detect CNS damage in neurologically symptomatic patients, including emphasis on protocols best suited to detect even subtle microvascular damage. These findings and any changes in them over time will be useful in determining the validity of the BB results.
Neurological assessments
Common Data Elements (CDEs) have been created for a number of neurological disorders, including TBI, stroke, and neuromuscular diseases (
Genotyping
As has been the case for TBI and stroke, knowledge of individual genotypes may improve the prediction of differing clinical outcomes of COVID-19 patients. 283 –286 Although individual, non-genetic susceptibility may influence the occurrence or severity of brain injury caused by SARS-Cov-2, variation in susceptibility to SARS-Cov-2 may also be attributable to individual differences in genetic susceptibility factors in infected individuals. Susceptible persons may have impaired innate abilities to fight viruses attributable to suboptimal interferon responses 287 or inability to mount adequate cell-mediated immune responses. 288 Mutations in Toll-like receptor 3 (TLR3) have been tied to increased herpes simplex encephalitis in patients, 289 suggesting that immune system impairment can increase viruses' abilities to invade the brain and cause injury. Polymorphisms of the sulfonylurea receptor 1-transient receptor potential melastatin 4 (Sur1-Trpm4) cation channel are also associated with the development of malignant cerebral edema after acute brain injury. 290,291 Importantly, investigators have recently identified a 3p21.31 gene cluster as a genetic susceptibility locus in patients with COVID-19 with respiratory failure and confirmed a potential involvement of the ABO blood-group system. 292,293
Other studies have reported associations between blood-group types and disease severity and multi-organ dysfunction in COVID-19. 294,295 In the first publications of the COVID Human Genetic Effort, researchers found that 101 of 987 patients with life-threatening COVID-19 pneumonia had neutralizing immunoglobulin G auto antibodies against the interferons (IFNs), including IFN-ω and 13 types of IFN-α or both, at the onset of critical disease. Some patients also had autoantibodies against the other three type I IFNs. Ninety-five percent of these patients were male. These autoantibodies also neutralized corresponding type I IFNs to block SARS-CoV-2 infection in vitro. 296
Other investigators discovered that among nearly 660 persons with severe COVID-19, >3.5% were completely missing a functioning gene. Further experiments showed that immune cells from those 3.5% did not produce any detectable type I IFNs in response to SARS-CoV-2. 297 Consequently, both groups lack effective immune responses that depend on type I IFNs. Whether IFNs were neutralized by autoantibodies, produced in insufficient amounts because of genetic influence, or because IFNs induced an inadequate antiviral response, their IFN deficits seem to be a commonality among a subgroup of people who suffer from severe COVID-19 pneumonia. It will be important to determine whether the same IFN deficits contribute to enhanced CNS injury in COVID-19 patients.
Among the known genetic risk factors for CNS injury, the potential contribution of the apolipoprotein E (ApoE4) genotype should be determined, especially given that cerebrovascular damage may be a prominent characteristic of brain injury in COVID-19 patients. ApoE4 is associated with increased risk of intracerebral hemorrhage (ICH) 298 and predicts unfavorable neurological outcome after TBI and stroke. 283,299 ApoE4 also appears to have direct effects on the cerebrovascular system and may affect neurovascular functions independently of its known influence on amyloid beta (Aβ) pathology in AD. 300,301
Use of health information technology to support integration
Unlike past pandemics, the fight against COVID-19 can utilize recent advancements in health information technology (HIT). Barriers to research during pandemics, such as those requiring in-person contact (e.g., obtaining informed consent and acquiring CDEs), can be more readily obtained by utilizing HIT. Electronic health record (EHR)-embedded strategies for CDE collection and customized computable composite outcomes can be gathered and deidentified while patients are contagious, in support of, although not replacing, traditional approaches. EHR-embedded strategies can be linked to clinical laboratories for remnant serum/plasma sample collection and storage, reducing the need for dedicated blood draws and further minimizing exposure of nurses and/or healthcare personnel to potential infection. EHR-embedded data also lends itself to machine learning or artificial intelligence approaches.
Multi-center databases of patients with COVID-19 built with CDEs mapped to interoperable data standards, such as the Observational Medical Outcomes Partnership (OMOP) Common Data Model, 302,303 could be used to develop predictive models for biodigital identification of patients at risk. More important, these approaches may also identify modifiable risk factors, susceptibility risk factors in patients, and aid in validation of best practices to inform patient care and future clinical trials.
Clinical Applications of Blood Biomarkers to Improve Medical Management of COVID-19 Patients
The identification of applications of BBs that could improve medical practice for management of CNS injuries in COVID-19 patients is a prerequisite for design of research studies assessing their clinical utility. Unlike single brain injuries such as stroke or TBI, COVID-19 is an evolving disease process that will require serial BB assessments to provide optimal data. In addition, BBs for different brain injury processes may have different expression profiles, 304 –307 an observation that may provide additional diagnostic information.
We have reviewed evidence for the neuroinvasive capacity of SARS-CoV2 and potential consequence of direct neuronal cell by SARS-CoV-2. In light of increasing evidence for CNS infection as well as for ischemic damage, microinfarcts, and vascular pathology, there is a clear medical need for diagnostic tests that potentially aid with screening and identification patients, improve patient management of those with CNS involvement, and prediction of short- and long-term neurological consequences. The potential for a blood-based test for neurological injury may help clinicians identify patients early in the disease process and assist in determining the need for advanced imaging and initiation of current or potential new therapies.
An accurate diagnostic test that could reflect the degree of ongoing, worsening, or improving neurological involvement would aid clinicians in following patients' response to therapy and their overall clinical course. These tests may be particularly useful when patients are in critical condition, on ventilators, sedated, and possibly with chemical paralysis for which movement to imaging suites and clinical evaluation of neurological functions are difficult. These patients are especially vulnerable to secondary CNS injuries, such as hypoxia, frequently observed during the clinical course of the disease. Finally, evidence of CNS involvement may portend long-term neurological consequences. Thus, BBs could help clinicians determine the potential for longer-term or delayed neurological deficits and disease and direct patients to appropriate rehabilitation regimens.
As pointed out in the following section, clinical applications of BB diagnostics would primarily affect medical practice in acute and critical care environments. Important related research applications include assessments of risks for neurodegenerative diseases and design of clinical trials to treat COVID-19.
Screening
Most screening will occur in emergency rooms and acute care facilities. Prolonged, potentially chronic systemic pathologies resulting from SARS-CoV-2 infection are of increasing concern, including recent reports of acutely undetected cardiovascular pathologies such as myocarditis. 295 Given the distribution of ACE2 receptors in the brain as well as systemic organs, it may be prudent to screen all COVID-19 patients for occult brain injuries that might, as in myocarditis for cardiac disease, later become clinically expressed as persistent neurological deficits and/or increased risk for neurodegenerative diseases (see sections above). In addition, elevations of brain injury biomarkers may be sensitive indicators to alert clinicians to accompanying injuries to systemic organs and the need to screen accordingly (e.g., a troponin test for cardiovascular damage). Conversely, lower levels of BBs may predict a more favorable neurological clinical course.
Non-restrictive screening studies can be used to identify variables that could influence BB levels in individual patients. Unless incorporated into predictive models, these variables could compromise the predictive value of BBs. A more restricted screening strategy should be based on the most current literature and minimally select patients on the basis of risk criteria, including disease severity, the presence of altered mental status and other acute neurological symptoms, previous histories of CNS injuries, including stroke and TBI, evidence of hypoxia, smoking, 308 dementia, 16, 309 –311 and the presence of any other pre-existing medical conditions that may render them more vulnerable to disease progression. Age is a major factor affecting disease severity and outcome of COVID-19 patients 31,310,312 (also see a previous work, 313 an observation which may require the development of age-adjusted norms for biomarkers such as GFAP and UCH-L1 314 ). Finally, in light of recent data on genetic influences on COVID-19 disease progression (see above section), genetic screening is advisable.
Acute diagnosis and triage
As reviewed in an earlier section, the potential utility of the BBs, GFAP and UCH-L1, to acutely diagnose even low levels of CNS injury, such as sport concussion, 214,215 and to triage moderate and severe TBI patients for imaging has been demonstrated. 217,271,315,316 In addition, BBs in combination with refined imaging classification systems can also assist in assessments of acute patient care needs (e.g., discharge vs. hospitalization), thereby assisting in maintaining a clinical care pathway that optimizes management of potentially scarce medical resources. 313,317
Prognosis
As pointed out above for screening tests,
The duration of confusion was longer in more severe clusters whereas loss of smell or taste was reported over a longer duration in milder clusters, suggesting that CNS injury increased in more severely affected COVID-19 patients. 324 It will also be important to identify potential confounders of accurate prognosis, and data provided by screening studies can provide assist in characterizing variables influencing disease severity and outcome. A useful model may be the International Mission for Prognosis and Analysis of Clinical Trials project, a study of outcome predictors in severe TBI patients. 325 –327
Management of therapeutic interventions in hospitalized patients
There is growing recognition by critical care specialists that all critically ill patients must be concurrently managed for risks both to systemic organs and to the brain. 328 COVID-19, as a systemic disease with potentially severe CNS consequences, confirms the merits of this approach. In addition to risks for CNS injury resulting directly from the virus, patients can suffer brain injuries as a result of secondary insults, such as hypoxia or hypotension, experienced during their hospital stays. A brain infected by the SARS-CoV-2 virus may be more vulnerable to secondary insults than an uninfected brain, given that the CNS has a low tolerance for repeated injuries. 329 –331 As emphasized in the section below, aside from limited information provided by imaging and surface electroencephalography measurements, there are no available tools to assess directly the evolution of brain injury in hospitalized patients or in ICUs.
Such information is essential in order to provide timely guidance in management strategies seeking to attenuate brain injury such as improved CNS oxygenation and perfusion as well as reductions in intracranial pressure. For example, BBs of brain injury and inflammation could be used to detect acute brain injury in a patient with COVID-19 with an accompanying “cytokine storm” who develops severe acute lung injury (ALI). Severe ALI mandates use of a protective lung strategy with tolerance of marginal oxygen saturation. Elevations of levels of brain injury biomarkers would also raise concerns over hypoxic brain injury from systemic hypoxemia or stroke, or possibly from direct CNS involvement of COVID-19, prompting an increase in FiO2 and an emergency diagnostic workup for stroke. Thus, early identification of acute brain injury complicating COVID-19 using serum biomarkers could prompt early interventions and improve outcomes.
Clinical applications in acute care facilities and emergency rooms
Existing FDA approval of use of BBs for acute diagnosis of mild versus moderate TBI 217 and numerous publications on the use of BBs for acute diagnosis of brain injury 220,221 strongly support the feasibility of studies of BBs for acute detection of CNS involvement. Diagnostic tools that can assist in rapid diagnosis of potential CNS injury from SARS-CoV-2 infection are badly needed in order to inform appropriate medical care and establish evidence-based clinical pathways. Although altered mental status is a significant sign of CNS injury in COVID-19 patients (e.g., see previous works 102,103,135,136 ), media reports of asymptomatic hypoxia suggest the need for early assessment of CNS involvement even in patients showing no neurological symptoms.
As has been the case for FDA-approved BBs of TBI, 217 circulating biomarkers may prove useful to determine the need for emergency CTs, thereby assisting in allocation of limited medical resources during pandemics and mitigating the need to transport highly infectious patients to these imaging facilities. Both military and civilian healthcare emphasize the need for information on patients' abilities to return to normal daily routines. Thus, providing accurate prognoses of the extent and duration of neurological deficits in COVID-19 patients is important. As with TBI, sufficient clinical validation of BBs in CNS injury could contribute to aiding the clinical course of patients as well as their neurological outcomes. 220,221
Clinical applications for hospitalized patients and in intensive care units
A substantial percentage of COVID-19 patients are admitted for hospitalization or ICU care. Monitoring the status of possible CNS injury in these patients is vital given that cognitive deficits are observed even in ICU patients receiving care for other medical complications not associated with a primary brain injury. 199,205,241,332 –334 Even a year after leaving the ICU, many people experience PTSD, cognitive deficits, and depression. 335 Thus, the presence or absence of CNS injury in the ICU will be important in determining subsequent neurological deficits and neuropsychiatric problems. ARDS in COVID-19 patients 336 leads to ICU admission and is itself associated with long-term cognitive impairment. 337
BBs also have clinical utility as diagnostics for detection of neurologic morbidity in ICU patients admitted for ARDS and multiple organ dysfunction syndrome, 338 both typical manifestations of severe COVID-19. BBs could reduce need for neuroimaging as screening tests for potential CNS damage. In addition, sensitive and specific BBs could replace the option for diagnostic lumbar punctures to collect samples for assessments of possible CNS involvement. Appropriate use of clinically validated brain injury biomarkers could more safely, rapidly, and inexpensively inform clinicians on any ongoing, potentially evolving brain pathology, thereby guiding management and intervention strategies.
Research Applications of Blood Biomarkers to Enhance Potential Utility of Blood Biomarkers for Risk Analyses and Clinical Trial Designs
Assessments of risks for neurodegenerative diseases
The assessment of possible risk factors for AD or other neurodegenerative diseases conferred by SARS-CoV-2 will require a long-term longitudinal study. Given the magnitude of the pandemic, an approach similar to the Framingham Heart Study could be warranted. Such a study should minimally include assessments of biomarkers already implicated in the early of stages of AD such as tau, beta amyloid, NfL, and GFAP 339,340 (Fig. 1).
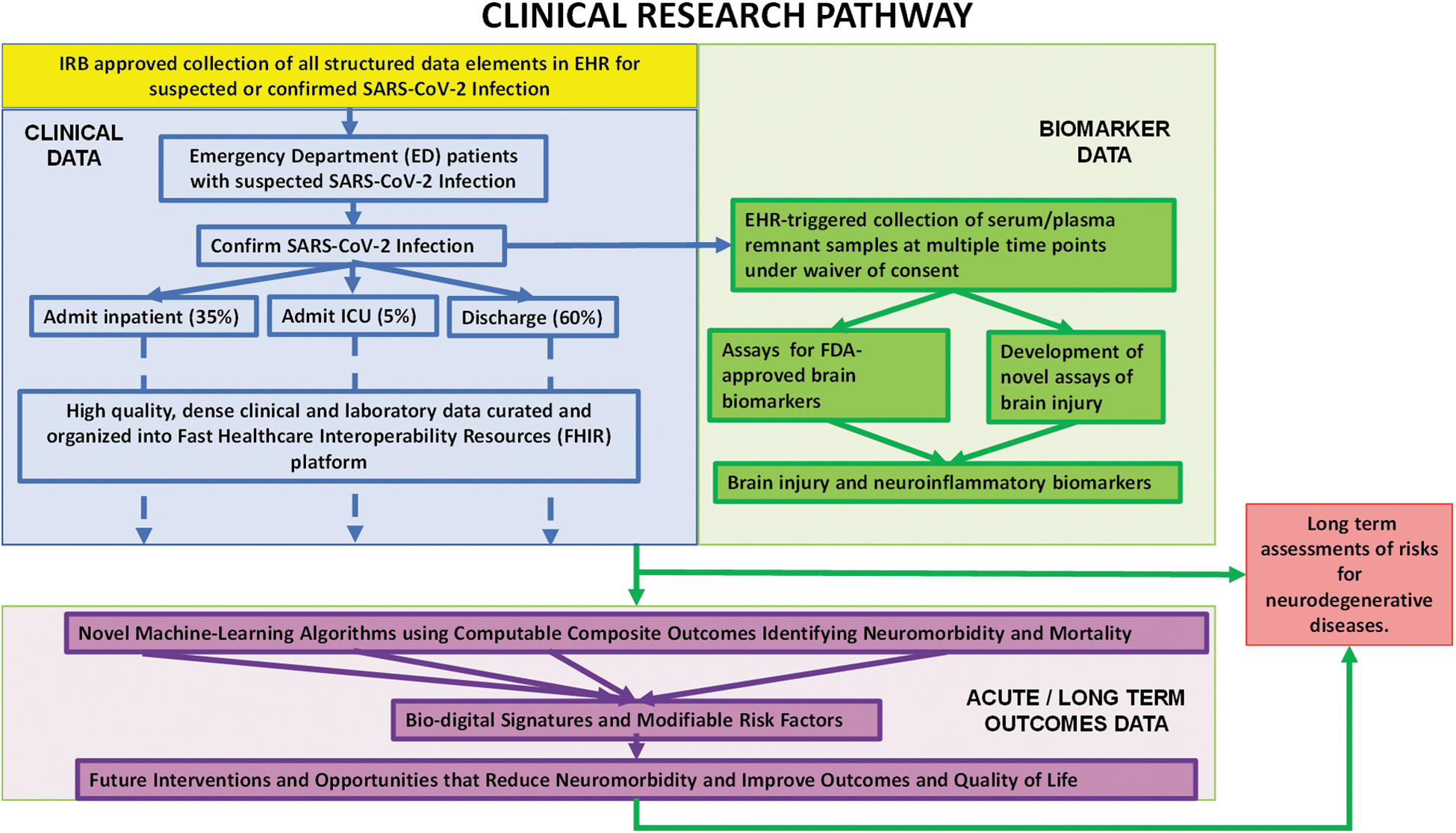
Generalized schematic of a clinical research study of BBs of CNS Injury in COVID-19 patients. BBs, blood biomarkers; CNS, central nervous system; COVID-19, coronavirus disease 2019; EHR, electronic health record; FDA, U.S. Food and Drug Administration; ICU, intensive care unit; IRB, institutional review board.
Design of clinical trials of therapies to treat central nervous system injury
There is widespread recognition that the use of BBs, alone and in combination with other diagnostic tools, can improve design of therapeutic trials for acute CNS injuries and neurodegenerative diseases. 341,342 BBs could also enhance the design of treatment trials designed to assess effectiveness of therapies for CNS injury in COVID-19 patients. A secondary analysis of BBs collected from moderate and severe TBI patients showed that BBs, especially GFAP, could reliably predict intracranial hemorrhages and outcomes. 342 In addition to approving UCH-L1 and GFAP for acute diagnosis of mild versus moderate TBI, the FDA has issued a Letter of Support for the incorporation of these two BBs into clinical trials studying potential therapies for mild TBI. 218 Operation Brain Trauma Therapy (OBTT) provided strong support for the use of BBs for pre-clinical drug development studies for TBI (e.g., see an earlier work 343 ) and reflects increasing confidence in the use of BBs to detect and monitor CNS injury.
Designing Clinical Studies to Examine the Utility of Blood Biomarkers for Diagnosis of Central Nervous System Injury: An Overview of a Clinical Research Strategy
Figure 1 presents a general outline of studies of BBs to diagnose CNS injury in COVID-19 patients. BBs data can be integrated with patient data and existing diagnostic technologies (brain imaging, neurological assessments, and genotyping) and readily incorporated into current standard-of-care practices. The pathway proposes serial collection of remnant blood samples acutely (admission to 72 h) under resource-limited pandemic conditions, daily (or more frequent) interrogation of BBs in hospitalized patients, and integration of BBs data with EHR-embedded records of neuromorbidity 344 and other structured CDEs. In addition, neurological condition at discharge and long-term follow-up of patients (e.g., 6–12 months) should be integrated with the EHR data. Selection and frequency of sampling of BBs can be modified to meet the needs of individual clinical study designs. Selection of BBs should be carefully designed and specifically selected on the basis of the goals of the study. For example, living systematic reviews of BBs of TBI can provide updated resources (e.g., see a previous work 345 ), and recent reviews of stroke 198 can provide updated resources for BB review and selection.
There are a number of currently well-characterized BBs of brain injury that can be incorporated in studies of COVID-19. 198,203 BBs should include GFAP, UCH-L1, S100B, and NfL, proteins extensively described in studies of acute brain injury. 198,202,203 Sensitive and FDA-approved assays are available. 217 In light of the potential importance of immunosuppression, inflammation, and “cytokine storms,” 143,144 a systematic assessment of markers of inflammation should also be included into BBs selected for further study. 346 It will be important to appropriately adjust sampling time points to identify potentially differing temporal profiles of individual biomarkers, a property which could assist in characterizing acute versus chronic pathological processes. Serial neurological assessments can be similarly adjusted. The pathway also provides for use of HIT to support integration of BBs data with other clinical and diagnostic information.
It is important that the designs of clinical research studies of BBs of CNS injury in COVID-19 patients generate data to assess the potential clinical utility of the BBs as outlined in the preceding section. Research approaches must also consider general clinical and pathobiological phenotypes resulting from SARS-CoV-2 CNS infection. These include: 1) the potential for SARS-CoV-2 to directly infect the brain producing acute CNS injury and subsequent persistent neurological deficits versus brain injury resulting from secondary systemic injuries; 2) the potential for previous brain injuries or existing neurodegenerative diseases to be associated with increased risks for and/or increased magnitudes of CNS injury; 3) the potential for hospitalized COVID-19 patients to have increased pathological responses to secondary systemic insults as a resulting of CNS infection by SARS-CoV-2; and 4) the potential for increased risk of subsequent neurodegenerative diseases such as AD or PD. It is unlikely that a single BB of brain injury will optimally differentiate the potential subsequent evolution into these phenotypes.
It is also essential that any study evaluating the utility of BBs review and report the analytical properties of the assay platform employed in the research (e.g., limits of quantification, lower limits of detection). Technological improvements have led to increased accuracy of the assays. Failure to provide the methodology and performance characteristics of BB assays makes it impossible to compare data from different studies and can lead to erroneous interpretations. 346
Conclusions
We are at the beginning of our understanding of the pathobiology of CNS infection by the SARS-CoV-2 virus and of the neurological consequences of this infection. The COVID-19 pandemic poses significant risks for acute and persistent neurological deficits, as well as possible increased risk for neurodegenerative diseases. The use of BBs of brain injury integrated with additional existing diagnostic tools with big dataset analytics could provide timely, cost-effective approaches to address this increasingly urgent unmet medical need.
Footnotes
Acknowledgments
The views expressed in this article do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. government.
Darci R. Smith is a military service member and federal employee of the U.S. government. This work was prepared as part of her official duties. Title 17 U.S.C. 105 provides that “copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a U.S. government work as work prepared by a military service member or employee of the U.S. government as part of that person's official duties.
Funding Information
This work received no external funding.
Michael D. Davis is funded by the National Institutes of Health (NIH)/National Heart, Lung, and Blood Institute (NHLBI; P01 HL128192), the Indiana Clinical and Translational Sciences Institute, the Lilly Endowment, and the Riley Children's Foundation. Christopher M. Horvat is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD; 1K23HD099331-01A1). Ruchira M. Jha receives grant funding from the NIH/National Institute of Neurological Disorders and Stroke (NINDS; K23101036), Chuck Noll Foundation, and Dean's Faculty Award.
Author Disclosure Statement
Ronald L. Hayes owns stock in, receives compensation from, and is an executive officer of Banyan Biomarkers, Inc. and as such may benefit financially as a result of the outcomes of this research or work reported in this publication. Nancy D. Denslow was a founder of the company and currently serves on the Board of Directors of Banyan Biomarkers, Inc. that has developed assays for biomarkers for traumatic brain injury. These biomarkers may be of interest to identify brain damage from COVID-19. Steven DeKosky chairs medical advisory boards for Acumen Pharmaceuticals and Cognition Therapeutics and chairs the Drug Safety Monitoring Boards for Biogen, Prevail Pharmaceuticals, and Vaccinex, Inc. He is editor of the Section on Dementia for Up-To-Date, a point of care electronic textbook, and Associate Editor of Neurotherapeutics, the journal of the American Society for Experimental Neurotherapeutics. None of them have any conflicts with the manuscript or its contents. Michael D. Davis is a Co-Founder of Airbase Breathing Company. Ruchira M. Jha is a paid consultant/on the Advisory Board for Biogen. Robert D. Welch will be doing a seminar for Abbott Labs, Inc. regarding a point-of-care test for GFAP and UCH-L1 and he previously (not since 2017) received contract research funding from Banyan Biomarkers, Inc.