
Abstract
Background:
Previous evidence has demonstrated that elevated low-density lipoprotein cholesterol (LDL-C) was associated with atherosclerosis. However, there is scarce population-based evidence for the role of remnant cholesterol (remnant-C) in arterial stiffness, an imaging marker for subclinical atherosclerosis. Herein, we aimed to evaluate the correlation of remnant-C with arterial stiffness beyond LDL-C in a check-up population.
Methods:
The study included consecutive subjects who visited the Murakami Memorial Hospital for health check-ups between 2004 and 2012. The calculation of remnant-C occurred as total cholesterol minus high-density lipoprotein cholesterol (HDL-C) minus LDL-C. The brachial-ankle pulse wave velocity (baPWV) >1400 cm/sec was defined as arterial stiffness or baPWV abnormality. The independent correlation of remnant-C level to arterial stiffness was evaluated using adjusted regression models.
Results:
A total of 909 participants were included (mean age 51.1 ± 9.6 years, male sex 64.9%). In multivariate linear regression analyses, remnant-C remained an independent predictor of the baPWV predictor [β: 94.76, 95% confidence interval (CI) 42.19–147.33, P < 0.001] after adjusting for confounders. After multivariable adjustment, including LDL-C, the highest remnant-C quartile odd ratio (OR) (95% CI) was 2.79 (1.27–6.09) for baPWV abnormality compared to the lowest quartile. Furthermore, each 10-mg/dL increase in remnant-C correlated with a 28% increased risk for baPWV abnormality (OR: 1.28, 95% CI: 1.04–1.57). Moreover, the correlation between remnant-C and baPWV abnormality was still significant in the participant subgroup with optimal levels of LDL-C.
Conclusions:
Our findings demonstrated that remnant-C levels correlated to arterial stiffness with the dependence of LDL-C and other cardiovascular risk factors in a check-up population.
Introduction
Reducing low-density lipoprotein cholesterol (LDL-C), mainly through standard or intensive statin therapy, reduces atherosclerotic cardiovascular disease (ASCVD). 1 Nevertheless, there remains a significant cardiovascular event residual risk in individuals who had the statin treatment, despite the optimal LDL-C levels. 2,3 Recently, ongoing attempts are still finding approaches to address these residual risks. 4 In light of the high-density lipoprotein cholesterol (HDL-C) elevating treatment failure to reduce cardiovascular events, 5 this research focus has shifted to remnant cholesterol (remnant-C), also named triglyceride-rich-lipoprotein (TRL) cholesterol, which is associated with the development of ASCVD.
Remnant-C includes the cholesterol content of chylomicron remnants and intermediate- and very-low-density lipoproteins during fasting or nonfasting. 6 Remnant-C particles in circulation can enter the arterial wall and consequently be taken up by macrophages in the subendothelial space, contributing to the production of foam cells, endothelial dysfunction, and in consequence, atherogenesis. 7,8 Observational and genetic population-based studies have indicated a significant correlation between increased remnant-C and high ASCVD risk. 9 –12 In addition, observational studies have demonstrated that elevated remnant-C correlated to high ischemic stroke risk in the general population. 13 Despite that, there was scarce proof from epidemiological studies based on population for the remnant-C role in arterial stiffness risk.
Measurement of arterial stiffness as brachial-ankle pulse wave velocity (baPWV) is an early detectable measure of vascular damage, firmly anticipating cardiovascular-related events in the general population or multiple pathophysiologic circumstances. 14 –16 In addition, arterial stiffness is commonly used as a noninvasive indicator of subclinical atherosclerosis in clinical practice. 14 The recognized predisposing factors for arterial stiffness include aging, hypertension, diabetes, obesity, and metabolic syndrome. 17 –19 Higher remnant-C levels are present more frequently in populations with obesity, diabetes, and atherogenic dyslipidemia, 20 so it is essential to identify the relationship between remnant-C and arterial stiffness. We aim to investigate the correlation of remnant-C with arterial stiffness in a check-up population.
Materials and Methods
Study design and population
A consecutive health check-up program was used at the Murakami Memorial Hospital Medical Health Check-up Center between March 2004 and December 2012 to select individuals whose baPWV was recorded (n = 1445). This medical study purpose, also called a human dock, explores chronic disorders and their risk factors. The details of the medical health check-up program were reported formerly. 21 The findings on the main outcome have already been published. 22 Currently, by sharing the available data in the document with the DRYAD database by Takuya et al., the data ownership has been transferred to the DRYAD database. 23 According to the terms of the DRYAD data service, the dataset can be used for secondary analysis in light of the new research hypothesis, and that is what we performed in our present study, in addition to the extraction of the cohort dataset, which was considered an observational cross-sectional study.
The study excluded subjects who met the following criteria from the study: receiving any medication (n = 433), receiving hormone replacement therapy (n = 66) or oral contraceptives (n = 1), known liver disease (n = 26), pregnant women (n = 1), and missing covariate data (n = 3). Furthermore, to ensure the accuracy of the baPWV measurement, subjects whose ankle-brachial index (ABI) <0.95 were excluded; therefore, 909 volunteers were finally included (Fig. 1).
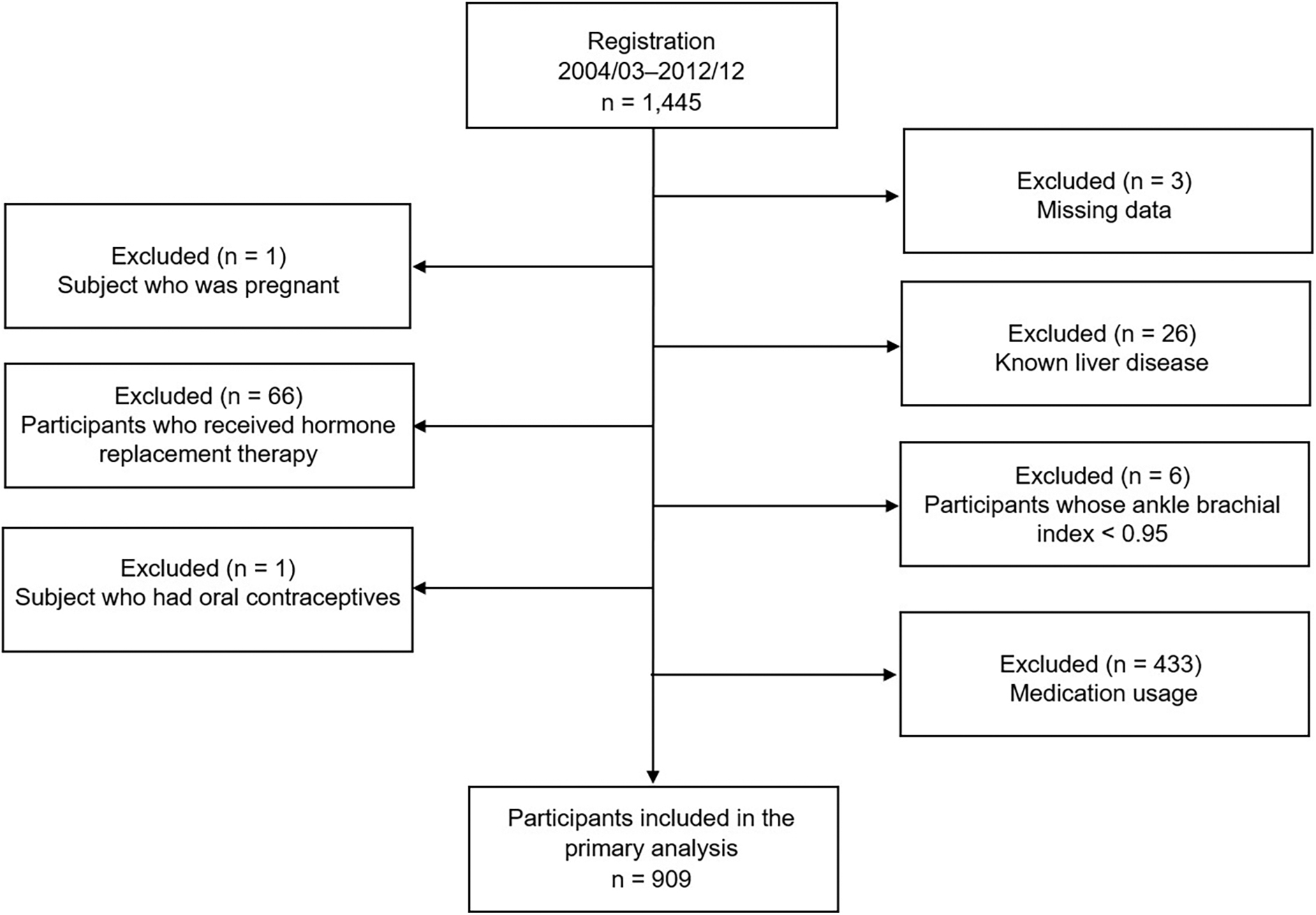
Study flowchart.
Definition of remnant-C
By utilizing MODULAR ANALYTICS (Hitachi High-Technologies Corp. Ltd., Japan), total cholesterol (TC), triglycerides (TG), HDL-C, and LDL-C were assessed at baseline, calculating remnant-C as TC minus LDL-C minus HDL-C. 24,25 Non-HDL-C was calculated as TC minus HDL-C. 24 No standard method is present for the remnant-C estimation. This equation was previously routinely used as it can be obtained from the standard lipid profile. 10,12,13,24,25 For this study, baseline remnant-C data were available for 909 individuals.
Measurement of baPWV and definition of arterial stiffness
An automatic waveform analyzer (Colin Medical Technology, Komaki, Japan) was used to measure baPWV and ABI. 26 A previous study has published detailed parameters and protocols for measuring baPWV. 22 Clinical data and other indicators are kept confidential by the analyst, reporting that the coefficients of variation between interobserver and intraobserver are 8.4% (r = 0.98, P < 0.01) and 10% (r = 0.87, P < 0.01), respectively. baPWV >1400 cm/sec was defined as arterial stiffness or baPWV abnormality. 27
Ethics approval and consent to participate
This study followed the Declaration of Helsinki 1964 and its later amendments and had the approval of the Murakami Memorial Hospital Ethics Committee. All participants gave Informed consent. Meanwhile, the Medical Research Ethics Committee of the Affiliated Hospital of Jining Medical University (2022-11-1001C) authorized the investigation.
Availability of data and materials
The datasets for this study are accessible from the corresponding author (A.Z.) upon reasonable request.
Statistical analysis
Baseline features of the study subjects were represented across baPWV, ABI, and plasma remnant-C levels. The reporting of continuous variables as mean ± SD or median (interquartile range) was based on the distribution of the variables and categorical variables as count (proportion). Continuous variables with skewed data were transformed into a log scale. The cohort was classified into four groups based on remnant-C-level quartiles to compare group characteristics with higher and lower remnant-C levels. Using the chi-square test, categorical variables were compared; and using the unpaired Student's t-test or the Mann-Whitney U-test, continuous variables were compared depending on the distribution of the variable in addition to the Kruskal-Wallis test on the remnant-C level.
In univariable analyses, simple linear regression analyses were constructed for baPWV (as a continuous variable) to determine whether remnant-C levels are potential predictors of arterial stiffness. Moreover, we performed multivariable logistic regression models to assess the independent correlation between remnant-C levels and the baPWV abnormality risk. Adjusting these models for age, sex, body mass index (BMI), current smoking, moderate to heavy alcohol consumption, hypertension, diabetes mellitus, TC, HDL-C, LDL-C, and uric acid was based on their correlation with interest outcomes or a change in effect estimate of more than 10%. 28 In addition, variables such as TG and non-HDL-C that were potentially confounders according to prior literature or knowledge of pathophysiology were also included in adjusted models in a stepwise manner. 29,30
Furthermore, for the dose dependence evaluation of the relationships between remnant-C and the risk of baPWV abnormality, we performed linear trend tests by entering the median value of each quartile group of remnant-C concentrations as a continuous variable in the adjustment models.
The study also used clinical cutpoint in assessing our finding robustness. Despite using medians as cutpoints, we focused on clinically relevant LDL-C cutpoints (130 mg/dL) derived from the worldwide guideline recommendation. 31 Determining the remnant-C cutpoint was based on an equivalent population percentile of the cohort corresponding to the LDL-C value.
Therefore, we divided the cohort into four mutually exclusive groups: group 1, with both elevated remnant cholesterol (RC) and LDL-C levels (RC ≥ 27.4 mg/dL and LDL-C ≥ 130 mg/dL); group 2, with nonelevated RC and elevated LDL-C (RC < 27.4 mg/dL and LDL-C ≥ 130 mg/dL); group 3, with elevated RC and nonelevated LDL-C level (RC ≥ 27.4 mg/dL and LDL-C < 130 mg/dL); and group 4, with nonelevated RC and nonelevated LDL-C level (RC < 27.4 mg/dL and LDL-C < 130 mg/dL, referent group). The independent and joint association of elevated remnant-C and elevated LDL-C levels with the risk of baPWV abnormality was evaluated using the same models adjusted for the previously mentioned covariates.
The study performed three sensitivity analyses to further evaluate the relationship between remnant-C and LDL-C levels and the risk of baPWV abnormality. First, we performed sensitivity analyses excluding participants with diabetes mellitus at baseline, considering that diabetes mellitus may increase remnant-C levels. 12 Second, we similarly excluded individuals whose BMI ≥24 kg/m2 in the sensitivity analyses because elevated remnant-C levels are likely to be affected by overweight or obesity. 12 Finally, we designate remnant-C level ≥24 mg/dL as the “elevated” level regarding previously published literature. 12
All statistical analyses were done using EmpowerStats version 4.0 (X&Y Solutions, Inc., Boston, MA) and R software. P < 0.05 in two-sided indicated statistically significant.
Results
The study included 909 participants (mean age 51.1 ± 9.6 years, male sex 64.9%). The median value of baPWV was 1370 (1264–1516) cm/sec. The frequency of baPWV abnormality, also defined as arterial stiffness, was 403 (44.3%). The median level of remnant-C was 25.8 (19.1–34.4) mg/dL. Table 1 illustrates the cohort baseline features. Participants with higher remnant-C levels were older and male; had higher levels of BMI, systolic and diastolic blood pressure, TG, TC, LDL-C, non-HDL-C, fasting plasma glucose, uric acid, and baPWV; high prevalence of known diabetes; and a higher proportion of baPWV abnormality, while had lower levels of HDL-C and estimated glomerular filtration rate than the lowest remnant-C quartile (Table 2).
Baseline Characteristics of the Cohort (n = 909)
Data represent median (IQR) or n (%).
baPWV, brachial-ankle pulse wave velocity; BMI, body mass index; GFR, glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol.
Baseline Characteristics of Cohort Study Participants Stratified by Remnant Cholesterol
Data represent median (IQR) or n (%).
Q, quartile.
In multivariable linear regression analyses, remnant-C remained an independent baPWV predictor [β: 94.76, 95% confidence interval (CI): 42.19–147.33, P < 0.001] after adjusting for confounders (Table 3). The baPWV abnormality rates increased in the remnant-C quartiles (Table 2). From the lowest to the highest quartile, the rates increased from 32.1% to 58.7% for baPWV abnormality (Table 2). In an age, sex, BMI, current smoking, moderate to severe alcohol consumption, hypertension, diabetes mellitus, TC, TG, HDL-C, LDL-C, non-HDL-C, and uric acid-adjusted model, odds ratio (OR) (95% CI) for the highest remnant-C quartile was 2.79 (1.27–6.09) for baPWV abnormality than for the lowest quartile (Fig. 2) (Table 4). Furthermore, each 10-mg/dL increase in remnant-C correlated with a 28% increased risk for baPWV abnormality (OR: 1.28, 95% CI: 1.04–1.57).
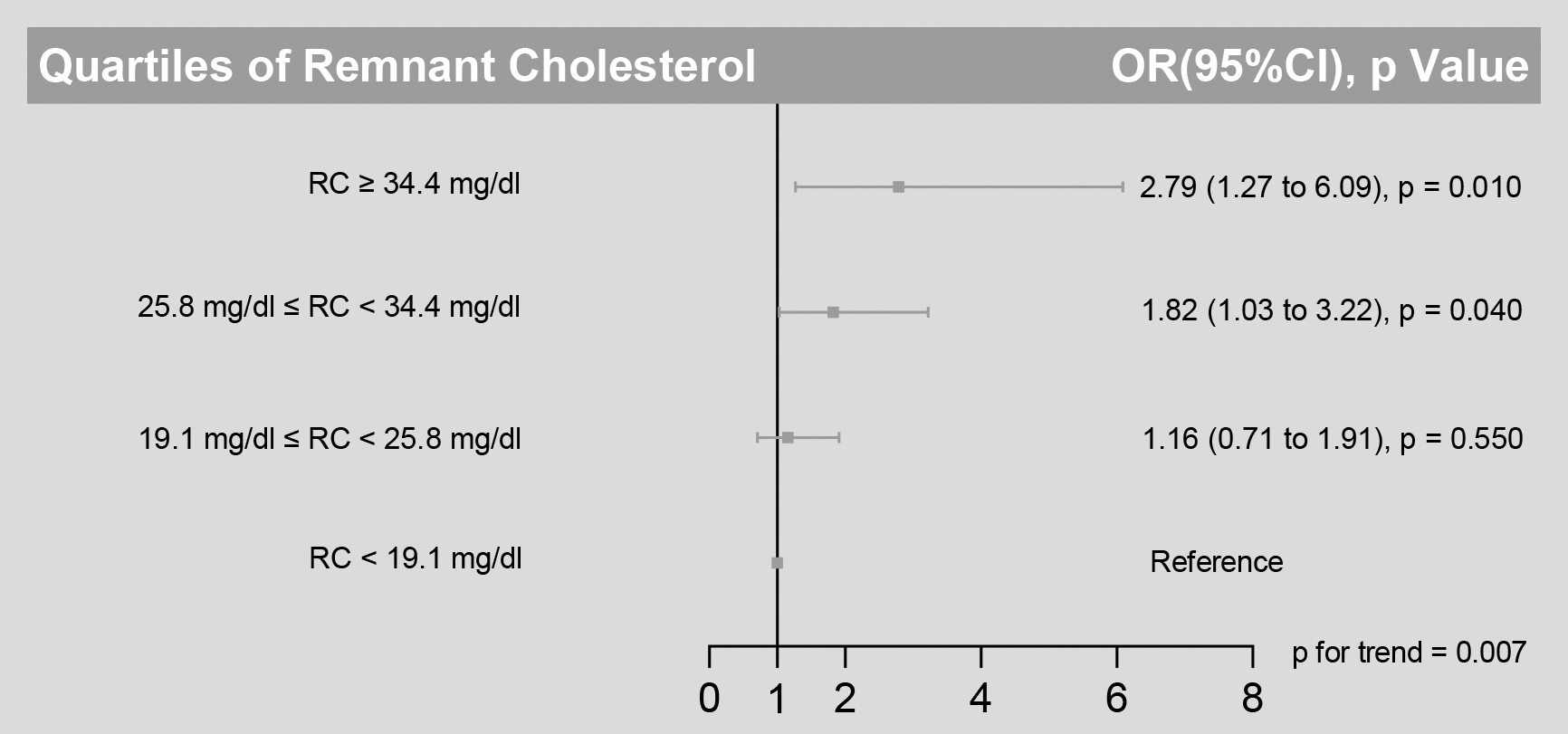
Risk of baPWV abnormality across quartiles of remnant cholesterol levels. To assess the risk of baPWV abnormality associated with remnant cholesterol levels, we calculated odd ratios for the second, third, and fourth quartiles (compared with the first quartile) of levels of remnant cholesterol. Analyses were adjusted for age, sex, body mass index, current smoking, moderate to heavy alcohol consumption, hypertension, diabetes mellitus, TC, TG, HDL-C, LDL-C, non-high-density lipoprotein cholesterol, and uric acid. baPWV, brachial-ankle pulse wave velocity; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; RC, remnant cholesterol; TC, total cholesterol; TG, triglycerides.
Univariable and Multivariable Logistic Regression Analyses Between Log Remnant Cholesterol and Brachial-Ankle Pulse Wave Velocity
Model I: no adjusted; Model II: adjusted for age+sex; Model III: Model II+body mass index, current smoking, moderate to heavy alcohol consumption, hypertension, diabetes mellitus, TC, TG, HDL-C, LDL-C, non-HDL-C, and uric acid.
CI, confidence interval; TC, total cholesterol; TG, triglycerides.
Odds Ratio (95% Confidence Interval) for Brachial-Ankle Pulse Wave Velocity Abnormality Stratified by Quartiles of Remnant Cholesterol
Model I: no adjusted; Model II: adjusted for age+sex; Model III: Model II+body mass index, current smoking, moderate to heavy alcohol consumption, hypertension, diabetes mellitus, TC, TG, HDL-C, LDL-C, non-HDL-C, and uric acid; RM, remnant cholesterol.
The evaluated residual lipid risk by a remnant-C ≥ 34.4 mg/dL identified participants at higher baPWV abnormality risk without regard to LDL-C concentrations (Fig. 2). Within the LDL-C subgroup (< 130 mg/dL), a high baseline remnant-C identified participants at a higher risk of baPWV abnormality risk than those at lower concentrations (Fig. 3). However, there was no similar finding in another LDL-C subgroup (LDL-C ≥ 130 mg/dL).
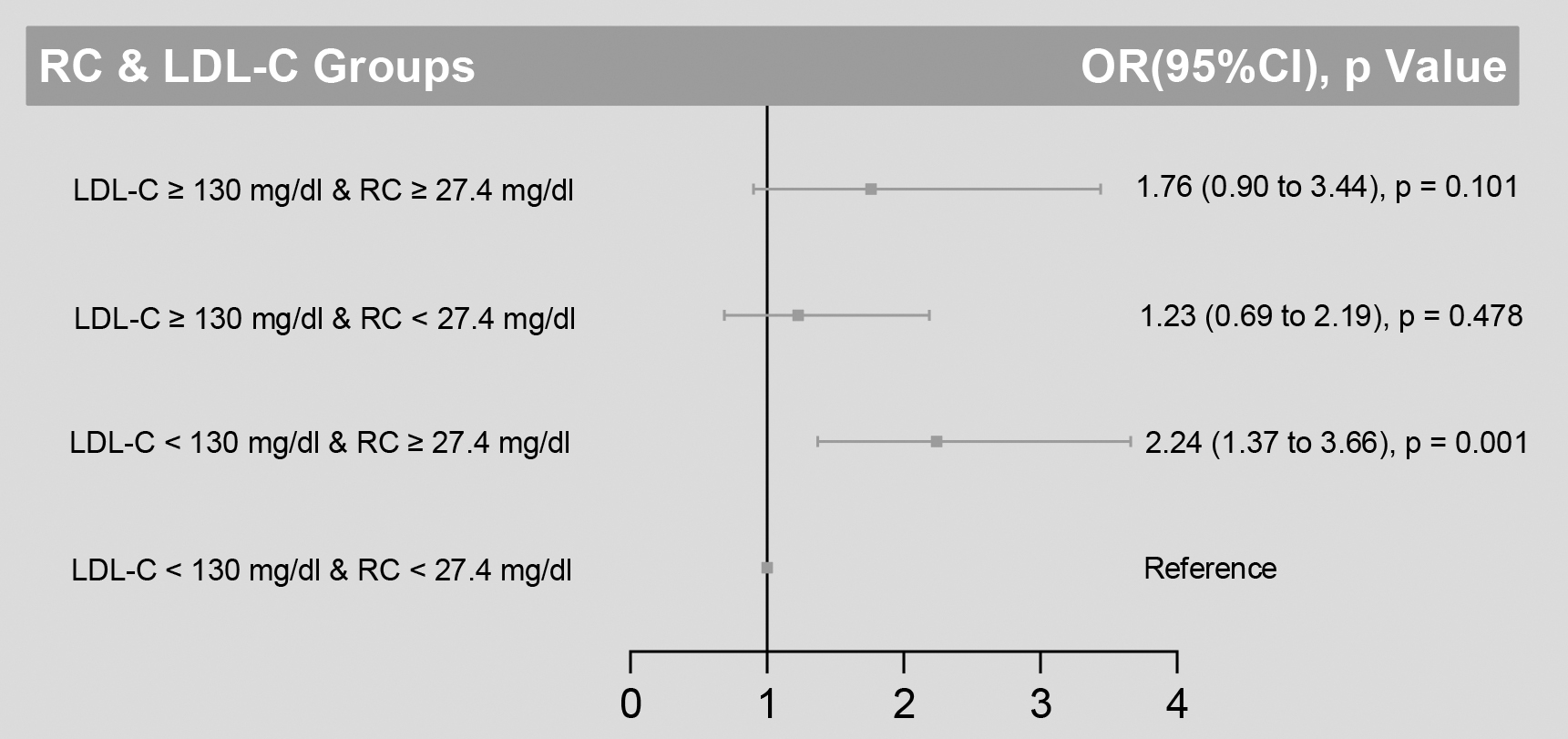
Risk of baPWV abnormality based on categories of LDL-C and remnant cholesterol levels. To assess the risk of baPWV abnormality by categories of low and high LDL-C and remnant cholesterol, odd ratios were plotted relative to the lowest risk category (LDL-C < 130 mg/dL and RC <27.4 mg/dL). Data were adjusted for age, sex, body mass index, current smoking, moderate to heavy alcohol consumption, hypertension, diabetes mellitus, TC, TG, HDL-C, LDL-C, non-HDL-C, and uric acid.
For sensitivity analyses, using the same model, we assessed the relationship between the remnant-C and LDL-C groups and the risk of baPWV abnormality. First, after we excluded participants with diabetes mellitus at baseline, the presence of higher remnant-C in subjects was correlated to a more than twofold risk for baPWV abnormality (Supplementary Table S1). Second, the higher remnant-C levels were still correlated to baPWV abnormality in individuals whose BMI <24 kg/m2 (Supplementary Table S2). Finally, when we selected the remnant-C cutpoint (24 mg/dL) that was obtained from previously published literature, 12 participants in group 2 (LDL-C < 130 mg/dL and RC ≥24 mg/dL) continued to have the highest risk of baPWV abnormality (Supplementary Table S3).
Discussion
In a population-based cohort of 909 individuals, high remnant-C levels were found to correlate with the risk of baPWV abnormality with the independence of traditional cardiovascular risk factors and LDL-C, revealing that identifying residual risk related to remnant-C, in addition to risk related to LDL-C, is clinically significant as we enter an innovative era of treatments aimed at lower lipids. Further studies are required to ascertain potential mechanisms to account for the correlation of remnant-C with baPWV abnormality and whether reducing its levels would improve clinical outcomes.
Our results are parallel to earlier studies, in which remnant-C was correlated to arterial stiffness and other subclinical markers of atherosclerosis. For instance, Qian et al. showed a positive correlation between high fasting remnant-C levels and carotid artery intima-media thickness in patients with ischemic stroke. This association is still even in participants with optimal LDL-C levels. 32 In addition, a cross-sectional analysis of 13,237 participants indicated that subjects with higher levels of remnant-C were associated with endothelial function and atherosclerosis. 33 Moreover, a recent analysis of 8028 subjects of a community-based atherosclerosis cohort from China suggested that remnant-C and TG levels were associated with arterial stiffness, revealing the remnant-C ability as a preferential therapeutic target. 34
This study extended the current literature by suggesting a stronger correlation between remnant-C levels and arterial stiffness independent of traditional cardiovascular risk factors and LDL-C. More importantly, the current study identified that a specific population with elevated remnant-C levels and optimal LDL-C levels have a higher risk of arterial stiffness, indicating that much attention should be paid to these individuals in clinical practice.
Mechanistically, the correlation between an increase in remnant-C and a high risk of baPWV abnormality is most likely interpreted by remnant-C per se causing atherosclerosis. 9 The mechanisms behind remnant-C facilitating and participating in forming atherosclerotic are unclear. However, several theories have been proposed for this association. First, similar to LDL-C, remnant-C in the circulation can enter the arterial intima where it is preferentially trapped due to its relatively large size, 35 then contributing to the development of atherosclerosis due to its cholesterol content. 36 Second, remnant-C may facilitate the development of atherosclerosis through endothelial dysfunction. Two population-based studies suggested that remnant-C levels have been associated with reduced brachial artery flow-mediated dilatation and impaired coronary vasomotor function. 37,38
The specific molecular mechanisms are that remnant-C could increase the reactive oxygen species production and induce endothelial cell apoptosis by increasing tumor necrosis factor-α (TNF-α) and interleukin (IL)-1β secretion. 39,40 Third, a Mendelian randomization study indicated that elevated remnant-C is linked causally to low-grade inflammation and ischemic heart disease; 41 nevertheless, no causal association between elevated LDL-C and low-grade inflammation was found. 39 TRLs were hydrolyzed by lipoprotein lipase to produce lipolytic products, including oxidized free fatty acids (FFAs). 39 Subsequently, oxidized FFAs and TRLs induce endothelial expression of ILs (i.e., IL-1, IL-6), cytokines (i.e., TNF-α), and proatherogenic adhesion molecules (i.e., intracellular adhesion molecule-1, vascular cell adhesion molecule-1), all of these play a significant role in atherosclerosis. 42
Our present sample differs in at least three aspects from those evaluated in earlier studies that associated remnant-C with the risk of baPWV abnormalities. First, the present cohort excluded subjects with ongoing lipid-lowering treatment. Thus, this cohort of participants without statins treated was well suited for investigating the correlation of remnant-C to arterial stiffness. Second, the causal correlation between remnant-C and ASCVD events was only demonstrated. 9 –13 However, the pathophysiological mechanisms behind remnant-C in the risk of arterial stiffness have scarce evidence. Thus, our study gave population-based evidence of remnant-C and arterial stiffness. Third, we used different clinical cutpoints to define elevated LDL-C levels, which showed the robustness of our findings.
Although our study includes several novel findings, it has some drawbacks. First, owing to the observational study's limitations, we could not study causality. Therefore, future prospective studies must validate the causal remnant-C function on atherosclerosis risk. Second, our study was conducted in a single ethnic population; therefore, these findings may not be generalized to other populations outside Japan. However, as far as we know, no available studies show ethnic differences in remnant-C ability that leads to atherosclerosis. Third, some covariates used in multivariate adjustments, such as those concerning alcohol consumption, are based on self-reporting and may be biased.
Finally, we used calculated remnant-C instead of direct measurement of remnant-C. However, indirectly calculated and directly measured remnant-C has a close correlation 11 ; calculated remnant-C may underestimate its value regarding direct measurement, 43 suggesting that our results are probably biased toward lower risk estimates. However, indirect remnant-C calculation can be easily performed from available lipid measurements, providing valuable data for clinical management.
Conclusions
Our findings indicated that estimated residual-C levels were correlated with arterial stiffness with the independence of LDL-C and other cardiovascular risk factors in a check-up population. Therefore, the current study provides clues for future studies of the pathophysiology of arterial stiffness. However, our findings should be confirmed in larger prospective studies.
Footnotes
Acknowledgments
We gratefully thank all the workers of the human dock study and editorial team of Home for Researchers (
Authors' Contributions
A.Z. and H.L.: Conceptualization and writing-review. P.Z.: methodology, data curation, formal analysis, and writing-original draft. J.M., D.L., and Q.L.: methodology, data curation, and formal analysis. P.X., L.L., and Z.Q.: methodology, visualization, and data curation. All authors reviewed and approved this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Jining Key Research and Development Program (grant no.: 2022YXNS051); the National Nature Science Foundation of China (grant no.: 81901228) and the Jining Key Research and Development Program (grant no.: 2022YXNS082).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.