
Abstract
Background:
Obstructive sleep apnea (OSA) is a serious threat to individual health. Diagnosis of OSA is mainly polysomnography (PSG). However, PSG monitoring is costly and time-consuming. At present, increasing studies are exploring new diagnostic methods for OSA. This study aimed to explore the diagnostic role of Sestrin2 in OSA.
Materials and Methods:
Sixty-four subjects were recruited in this study. The concentration of plasma Sestrin2 of all subjects were measured and compared. Spearman's correlation analysis was used to investigate the correlation between plasma Sestrin2 concentration and other factors. Receiver-operating characteristic (ROC) curve was used to investigate the role of Sestrin2 in the diagnosis of OSA, moderate-severe and severe OSA.
Results:
Subjects were divided into OSA group (n = 38) and control (n = 26). Levels of Plasma Sestrin2 were significantly higher in OSA patients than in controls. Sestrin2 was positively correlated with oxygen reduction index and negatively correlated with mean oxygen saturation and lowest oxygen saturation. The area under ROC curve (AUC) of Sestrin2 for OSA diagnosis was 0.740 [95% confidence interval (CI), 0.615–0.842], the cutoff value was 1.86 ng/mL, and the sensitivity and specificity were 81.58% and 61.54%, respectively. The AUC of Sestrin2 for the diagnosis of severe OSA was 0.801 (95% CI, 0.682–0.890), and the cutoff value was 5.21 ng/mL exhibiting the sensitivity and specificity of 61.90% and 90.70%, respectively.
Conclusion:
Setrin2 is a marker for OSA and may be helpful in the diagnosis of OSA.
Introduction
Obstructive sleep apnea (OSA) is a serious threat to individual health. 1 The method for diagnosing OSA is mainly polysomnography (PSG) monitoring. However, PSG monitoring is costly and time-consuming, and it requires patients to have good compliance and professional technicians to analyze the results. 2 –4 At present, the questionnaire plays a role in screening OSA. However, the accuracy of questionnaire in screening OSA is highly controversial. 5 Accordingly, some inflammation-related factors are used to diagnose OSA, such as interleukin 6 (IL-6), tumor necrosis factor-α (TNF-α), and C-reactive protein (CRP). 6,7 Moreover, oxidative stress is closely related to the pathogenesis of OSA. 8 Oxidative stress factors, such as 8-isoprostaglandin and thioredoxin (TRX), are helpful in the diagnosis of OSA. 9,10
Sestrin2 is an important oxidative stress factor. 11 Our previous study found that Sestrin2 was involved in the pathogenesis of OSA and was related to the severity of OSA. 12 Therefore, we speculated that Sestrin2 might be helpful for diagnosis of OSA. The purpose of this study was to explore the role of Sestrin2 in diagnosis of OSA.
Materials and Methods
Research population
During the period from June 2016 to January 2019, we recruited 64 subjects who had undergone PSG due to snoring at the First Affiliated Hospital of Kunming Medical University. Some of the subjects came from Jiang et al., 13 which was a partly secondary analysis of the subjects from Jiang et al. Before PSG monitoring, all patients underwent systematic physical examination and consultation to obtain their previous health conditions.
The inclusion criteria were subjects aged 18–65 years. The exclusion criteria were patients with lung diseases, such as pneumonia, lung abscess, and so on, heart failure, kidney diseases, cerebrovascular diseases, metabolic diseases such as diabetes, patients with mental disorders, patients with other sleep disorder-related diseases other than OSA according to history of past illness, pregnancy, and patients with OSA who had received treatment for OSA before this study.
Demographic characteristics, height, body mass index, and waist-hip ratio were measured before PSG. This study was approved by the Ethics Committee of the First Affiliated Hospital, Kunming Medical University.
PSG monitoring
All subjects were monitored with overnight PSG (Alice 5, America). Apnea was defined as a drop in amplitude of more than 90% of nasal airflow for at least 10 sec. Hypopnea was defined as a drop in airflow amplitude of more than 30% associated with oxyhemoglobin desaturation of 3% or more or associated with arousal. 14 Apnea/hypopnea index (AHI) was obtained after analysis of all PSG records and OSA was stratified according to the American Academy of Sleep Medicine Clinical Practice Guideline. 15 In addition, central respiratory events were excluded from this study. Normal subjects were defined as AHI <5 events/hr, and OSA patients were defined as AHI ≥5 events/hr.
Plasma test
On the morning of the day when the PSG monitoring had been completed, the venous blood was taken from all subjects after fasting for more than 8 hrs and centrifuged at 4°C for 20 min (speed 3000 rpm), and the supernatant was stored in a refrigerator (SANYO, Japan) at −80°C for testing. Sestrin2 was detected with ELISA kit (YAD, China). Other tests, including fasting glucose, triglycerides, total cholesterol, low-density lipoprotein (LDL), and high-density lipoprotein (HDL) were performed by the First Affiliated Hospital, Kunming Medical University.
Statistical analysis
Data are presented as mean ± standard deviation. In addition, the single sample Kolmogorov–Smirnov method was used to detect the distribution of data. The data of normal distribution were compared by unpaired t-test and that of non-normal distribution by rank sum test. Spearman's correlation analysis was used to analyze the correlation between Sestrin2 and other parameters. The area under receiver-operating characteristic (ROC) curve (AUC) was used to investigate the diagnostic efficiency of Sestrin2 concentration for OSA, moderate-severe OSA, and severe OSA, respectively. ROC curve drawing and AUC calculation used MedCalc 18.11 (Ostend, Belgium), and other statistical analysis was performed using SPSS 17.0 (Chicago, Illinois).
Results
Sixty-four subjects were enrolled in this study and were divided into two groups: OSA group (n = 38) and control group (n = 26). OSA group was divided into three subgroups according to AHI: mild group (15 > AHI ≥5), moderate group (30 > AHI ≥15), and severe group (AHI ≥30). The results of plasma Sestrin2 and characteristics of all subjects are listed in Table 1.
Demographic Characteristics, Sleep Monitoring Parameters, and Blood Measurements of OSA and Control Groups
Values are indicated as the mean ± standard deviation.
Values are indicated as percentage.
P < 0.05, the results are statistically significant.
AHI, apnea/hypopnea index; BMI, body mass index; ESS, Epworth Sleepiness Score; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NREM, nonrapid eye movement; ODI, oxygen desaturation index; OSA, obstructive sleep apnea; PRTS, percentage of recording time spent; REM, rapid eye movement; TC, total cholesterol.
The concentration of Sestrin2 in OSA was significantly higher than that in control group (Fig. 1).
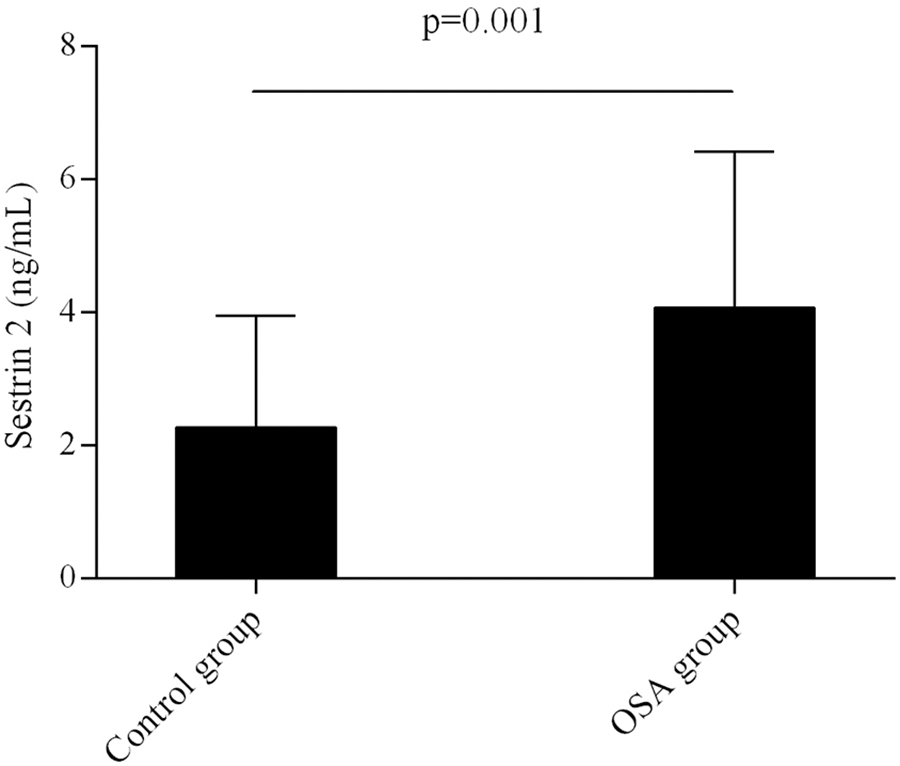
Comparison in plasma Sestrin2 level between OSA and control groups. OSA, obstructive sleep apnea.
Table 2 shows that Sestrin2 was positively correlated with the severity of OSA, HDL and oxygen reduction index, and negatively correlated with mean oxygen saturation and lowest oxygen saturation.
Spearman's Correlation Analysis Between Sestrin2 and Other Factors
P < 0.05, the results are statistically significant.
Figure 2 shows the ROC curve of Sestrin2 for OSA diagnosis. The AUC was 0.740 [95% confidence interval (CI), 0.615–0.842] and the optimal cutoff value was 1.86 ng/mL, exhibiting the sensitivity and specificity of 81.58% and 61.54%, respectively (Table 3). Figure 3 shows the ROC curve of Sestrin2 for the diagnosis of moderate-severe OSA, the AUC was 0.766 (95% CI, 0.644–0.863), and the optimal cutoff value was 1.66 ng/mL, exhibiting the sensitivity and specificity of 93.55% and 51.52%, respectively (Table 4). Figure 4 shows the ROC curve of Sestrin2 for the diagnosis of severe OSA, the AUC was 0.801 (95% CI, 0.682–0.890), and the optimal cutoff value was 5.21 ng/mL, exhibiting the sensitivity and specificity of 61.90% and 90.70%, respectively (Table 5).
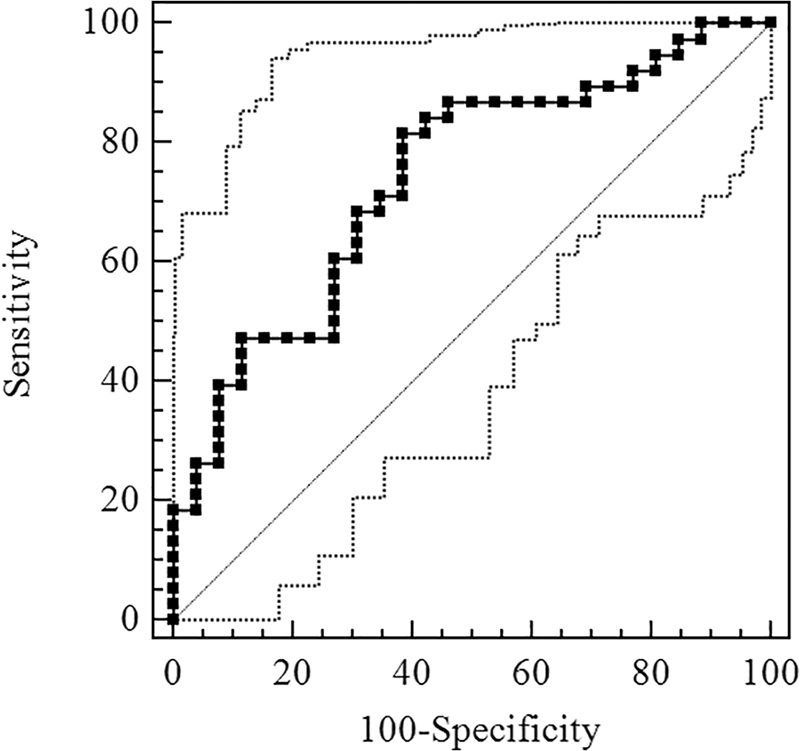
ROC curve for evaluation of Sestrin2 level of diagnostic effect for OSA. ROC, receiver-operating characteristic.
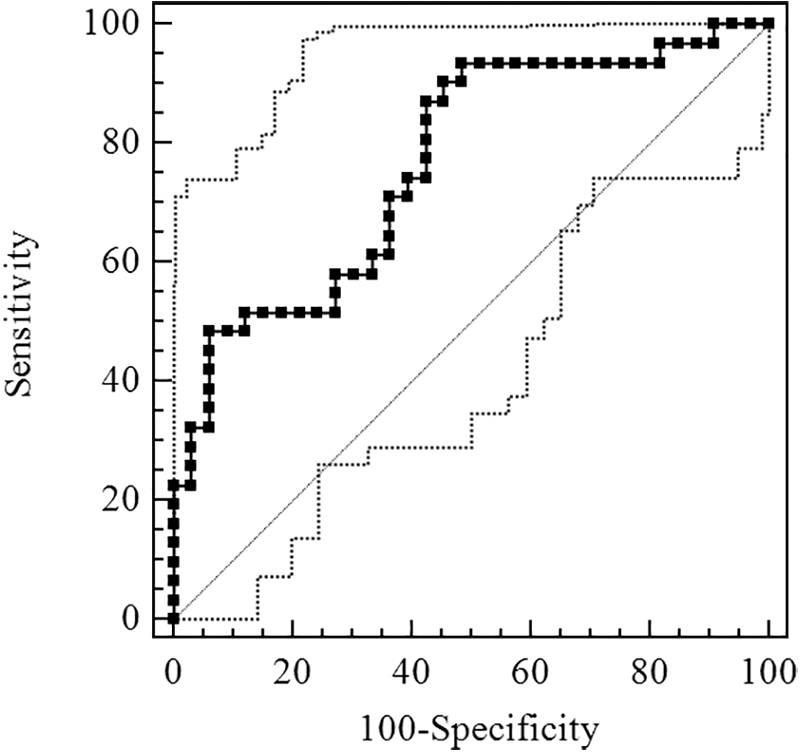
ROC curve for evaluation of Sestrin2 level of diagnostic effect for moderate-severe OSA.
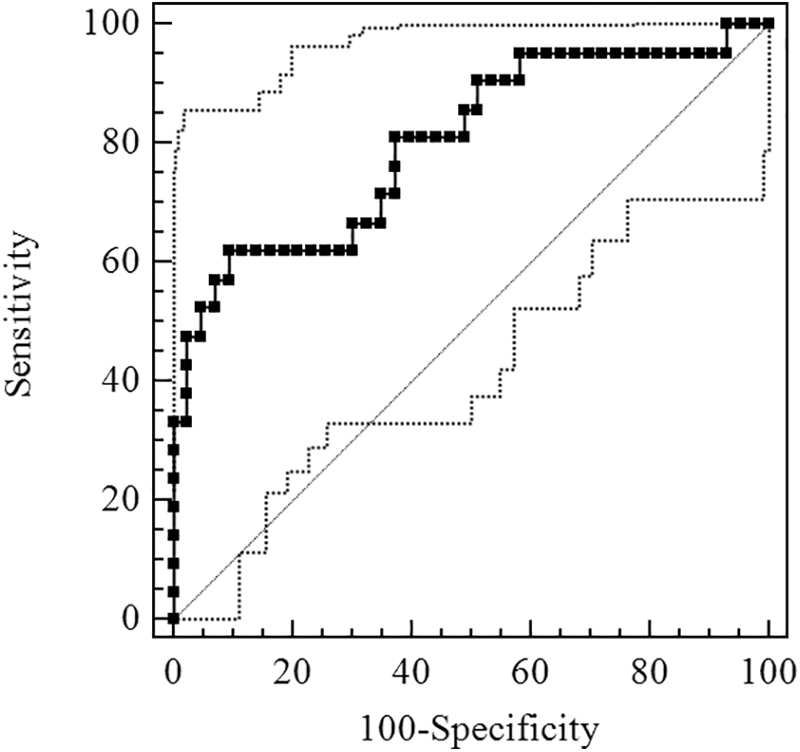
ROC curve for evaluation of Sestrin2 level of diagnostic effect for severe OSA.
Characteristic of Cutoff Value Concentration for Sestrin2 in Diagnosis of OSA
AUC = 0.740 (95% CI, 0.615–0.842).
AUC, area under receiver-operating characteristic curve; CI, confidence interval; LR, likelihood ratio.
Characteristic of Cutoff Value Concentration for Sestrin2 in Diagnosis of Moderate-Severe OSA
AUC = 0.766 (95% CI, 0.644–0.863).
Characteristic of Cutoff Value Concentration for Sestrin2 in Diagnosis of Severe OSA
AUC = 0.801 (95% CI, 0.682–0.890).
Discussion
In this study, the concentration of Sestrin2 in plasma was significantly higher in OSA group than that in control group, suggested that Sestrin2 might differentiate OSA from non-OSA. Moreover, the concentration of Sestrin2 in plasma was positively correlated with the severity of OSA, suggested that OSA severity would be judged by Sestirn2 elevation, which met with the requirements for ideal biomarker. 16 Further analysis showed that Sestrin2 diagnosed OSA and severe OSA with AUC of 0.740 and 0.801, respectively, suggested that Sestrin2 was helpful for diagnosis of OSA, especially for severe OSA.
Sestrin2, a member of the Sestrin family, consists of two globular subdomains with similar structure, and is a stress-induced metabolism regulator. 11,17 The expression of Sestrin2 is mediated by hypoxia or a series of reactions induced by hypoxia. Intermittent hypoxia (IH) is ubiquitous in OSA, 18 which induces the production of hypoxia-inducible factors 119 and results the elevating expression of Sestrin2. 20 Meanwhile, IH induces strong oxidative stress, 21 leading to excessive accumulation of ROS, which in turn activates antioxidant response elements (AREs). Consequently, AREs induce nuclear erythroid-related factor 2 (Nrf2)-mediated expression of Sestrin2. 22
Moreover, endoplasmic reticulum (ER) stress and oxidative stress can induce each other. 23 It may also be the cause of Sestrin2 expression. On the one hand, ER stress induces the production of Sestrin2 through a variety of complex pathways, 24 and on the other hand, oxidative stress may cause elevating expression of Sestrin2 by the pathway as described in previous study. 22 Therefore, hypoxia or/and oxidative stress is an important cause of Sestrin2 increasing in OSA. 12 In addition, activated Sestrin2 indirectly regenerates peroxidase (Prx) by promoting the expression of TRX, or removes the Nrf2 inhibitor Kelch-like epichlorohydrin-associated protein 1 (keap1) to activate the antioxidant transcription process, 24,25 to exert antioxidant effects.
Some explored new ways to diagnose OSA, such as portable monitoring (PM). 26,27 To some extent, it can make up for the defects of PSG. 28 However, some suggested that the diversity of PM devices and multiscoring schemes had a significant negative impact on the diagnostic effectiveness of OSA. 29,30 Moreover, questionnaires are often used to screen OSA. 5 However, OSA is often accompanied by cognitive deficits, 31 so that its accuracy is not enough to rely on. Accordingly, some biomarkers with diagnostic accuracy and simple operation were used to diagnose OSA.
Currently, inflammation-related factors, such as IL-6, TNF-α, and CRP, are considered as potential biomarkers for the diagnosis of OSA. 6,7 Fleming et al. 32 obtained the AUC of diagnosing OSA (moderate-severe) by CRP was 0.73, and Li et al. 10 even obtained the AUC of diagnosing OSA by IL-6 was 1.00, which suggested that inflammation-related factors as biomarkers might be helpful in diagnosing OSA. Oxidative stress is an important pathological feature of OSA. 33 Guo et al. 9 found that the TRX, as an oxidative stress factor, was a biomarker of OSA exhibiting the sensitivity and specificity of 91% and 78%, respectively. In addition, 8-isoprostaglandin, another oxidative stress factor, could also be used as a biomarker to identify OSA. 10
Our previous study found that Sestrin2 was involved in OSA, and it was positively related to the severity of OSA. 13 Unfortunately, we did not discuss whether Sestrin2 was helpful for the diagnosis of OSA, which limited its clinical usefulness. On the basis of previous study, we included more subjects and reanalyzed the results, and results showed AUC of Sestrin2 for the diagnosis of moderate-severe OSA and severe OSA was 0.766 and 0.801, respectively. In view of the above findings, Sestrin2 may be recommended as a valuable marker for diagnosing OSA, especially for diagnosing severe OSA. Our findings provide a theoretical basis for the clinical application of Sestrin2.
There were some limitations in this study. The sample size of this study was small and it was not conducted randomly. So randomized, multicenter, large-sample studies are needed to confirm the accuracy of Sestrin2 in diagnosing OSA in future.
Conclusions
Sestrin2 is a marker for OSA diagnosis and may be helpful in the diagnosis of OSA.
Data Availability
The data used to support the conclusions of the study are included within this article.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (nos. 81560589, 30960450, 81173110, 81402991), the Yunnan Provincial Science and Technology Department [nos. 2019FE001 (-058)], Yunnan Provincial Department of Education (nos. 2017zzx201, 2018JS161) and Teaching and Reform Program of Kunming Medical University (no. 2017-JY-Y040).