
Abstract
The Editor-in-Chief of Metabolic Syndrome and Related Disorders officially retracts the article entitled, “Prediction of Proliferative Diabetic Retinopathy to Asymptomatic Obstructive Coronary Artery Disease in Chinese Type 2 Diabetes Individuals: An Exploratory Study: by Jian-Bo Zhou, Xiao-Rong Zhu, Wei Zhao, Lu Yin, Hong-Bing Li, Lu Qi, and Jin-Kui Yang (Metab Syndr Relat Disord, 17(7):2019;367–373; doi: 10.1089/met.2018.0140).
The Publisher and Editor of the journal received an email from Professor Jin-Kui Yang, MD, PhD, from the Beijing Diabetes Institute, Department of Endocrinology, Beijing Tongren Hospital / Capital Medical University in Beijing, China, indicating that he had been falsely and unknowingly added as a coauthor of the published article by the lead author, Dr. Jian-Bo Zhou. Dr. Yang also stated that fabricated data exists in the article.
Upon receipt of the complaint, the journal asked Dr. Zhou to submit the original data from which the article was derived so that it could be independently evaluated, as well as detailed documentation on the specific contributions of all named authors. Dr. Zhao responded with the following message (in full):
“Could you retract this article entitled “Prediction of Proliferative Diabetic Retinopathy to Asymptomatic Obstructive Coronary Artery Disease in Chinese Type 2 Diabetes Individuals: An Exploratory Study,” (2019:17(7):367–373; DOI: 10.1089/met.2018.0140).
I apologized for this process.”
[sic]
No other responses or details were provided in Dr. Zhou's message.
Since the original data was not supplied as requested, and in view of Dr. Zhou's response, all coauthors listed on the paper were notified via email of the decision to retract the paper, utilizing the email addresses provided to the journal at the time of original submission. No responses were received.
Metabolic Syndrome and Related Disorders
is committed to preserving the veracity of scientific literature and the community it serves.
Introduction
Coronary artery disease (CAD) is a leading cause of mortality among patients with type 2 diabetes (T2D). 1 The phenomenon that CAD is often asymptomatic in patients with diabetes makes early identification of CAD a challenge, including obstructive CAD and ischemic nonobstructive microvascular dysfunction CAD. 2 Traditional coronary risk factors such as dyslipidemia and hypertension are not associated with asymptomatic CAD. 3,4 Intensified routine screening for asymptomatic CAD among patients with T2D is not recommended at present.
In a recent study, diabetic retinopathy (DR) was found to confer a risk equivalent to conventional factors, including smoking, hypertension, and dyslipidemia in European descents. 5 DR, as a common chronic microvascular complication, is perceived as contributing to cardiovascular (CV) events and all-cause mortality in T2D. 6,7 Our former results indicated that patients with proliferative diabetic retinopathy (PDR), as advanced stage of DR, had additional contribution for predicting CV death. 8 Therefore, these findings might demonstrate that DR and CV events may have shared certain pathophysiological disease processes. 9
Recent research showed that there may be common risk factors for PDR and CAD at the presence of chronic kidney disease. 10 However, it remains less understood whether PDR is associated with increased risk of asymptomatic CAD, including asymptomatic obstructive coronary artery disease (AO-CAD), at the absence of chronic kidney disease. Furthermore, because of the wide utilization of antivascular endothelial growth factor (anti-VEGF) agents for PDR, studies found that anti-VEGF agents could increase the risk of CAD. 11 So, understanding the specific relationship of PDR with AO-CAD at the absence of chronic kidney disease is clinically relevant.
To address this gap, the aim of this study was to explore the identification of PDR to AO-CAD defined by coronary angiography in a retrospective discovery set. Subsequently, the prediction of PDR to AO-CAD was investigated in a prospective validation cohort.
Subjects and Methods
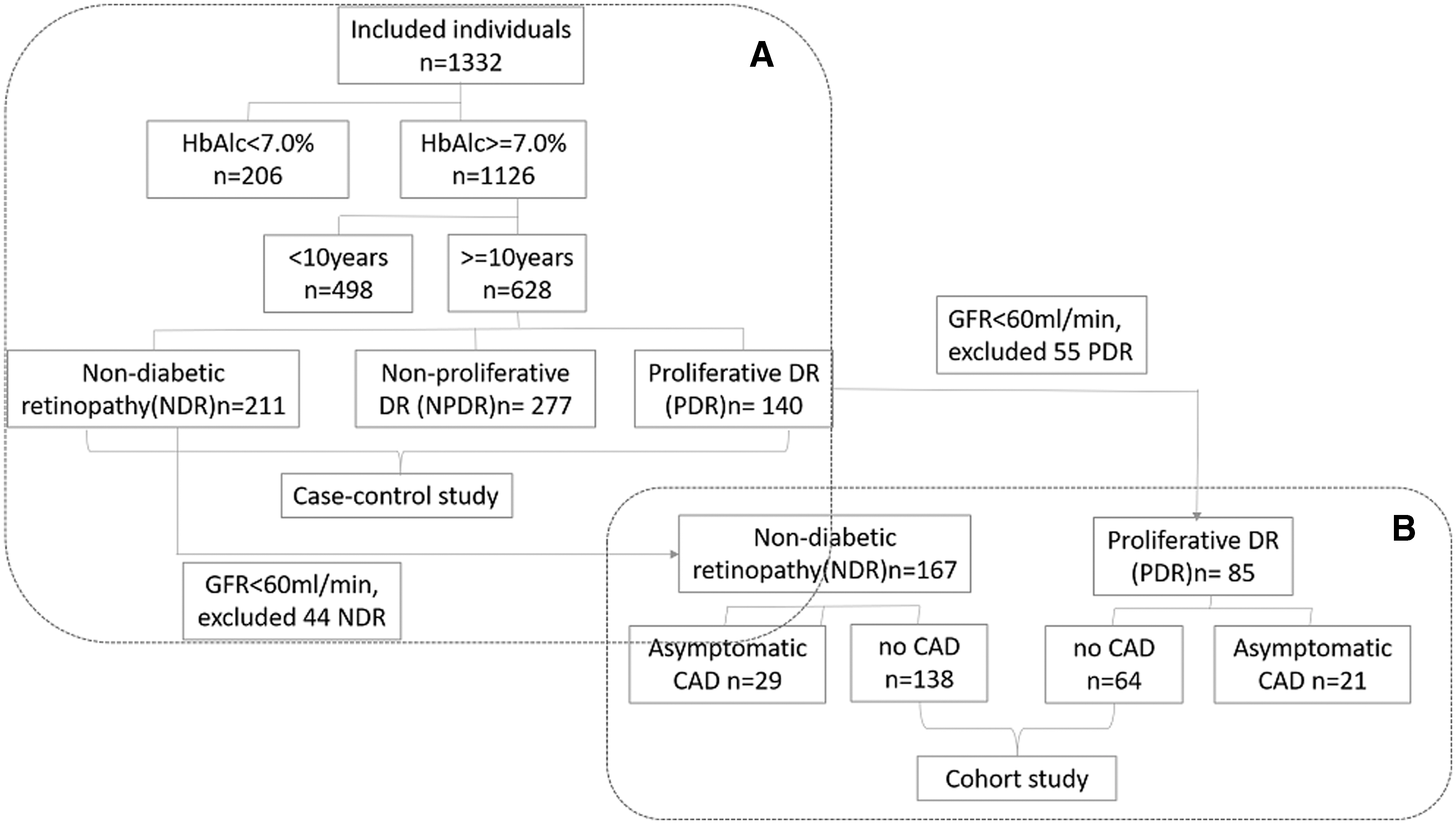
The flowchart of this study is shown in Fig. 1. The data that support the results of this study are available from the corresponding author upon reasonable request. This study consisted of a retrospective discovery set and a prospective validation cohort. Details of the discovery and validation set are in Fig. 1. In short, the retrospective discovery set was to search the additional identification value of PDR to AO-CAD on the base of conventional risk factors. Then in those individuals with no CAD from the earlier case–control set, the predictive values of PDR to CAD were validated in this prospective cohort by follow-up.
This retrospective discovery set was performed. Participants (n = 1332) with comprehensive data on diabetic retinopathy and coronary artery disease were chosen during January 2011 and December 2012 in Beijing, China. From the total 1332 inpatients presenting in the Beijing Tongren Hospital, we excluded patients in whom there was lower A1c (<7%; 206 patients), patients with diabetic duration <10 years (498 patients)
Retrospective discovery set
This retrospective hospital-based case–control study was performed. Inpatients (n = 1332) with comprehensive data on DR and coronary angiography were screened during January 2011 and December 2012 in Beijing, China. Given to the effect of glucose and diabetic duration on the risk of CAD in individuals with diabetes, inpatients with glycated hemoglobin A1c (HbA1c) ≥7.0% (53 mmol/mol) and diabetic duration ≥10 years were included to balance the cofounders between case and control subjects. From the total 1332 inpatients presenting in the Beijing Tongren Hospital, we excluded patients in whom there was lower A1c (<7%; 206 patients) and patients with diabetic duration <10 years (498 patients) (Fig. 1A). Patients with PDR or without any degree of retinopathy [nondiabetic retinopathy (NDR)] were selected in the retrospective discovery set (Fig. 1A) (n = 351, NDR = 211, PDR = 140). Exclusion criteria were as follows: history of known CAD, congestive heart failure, stroke, or any clinical indication for CAD.
AO-CAD and PDR screening
Those with coronary angiography and with eligible eye phenotypes (NDR or PDR) were assigned for this study (Fig. 1). AO-CAD was defined as detection of ≥75% diameter stenosis on coronary angiography, at the same time of no known CAD. Non-CKD was defined as glomerular filtration rate (GFR) >60 mL/(min·1.73 m2) (non-CKD) from 99Tcm-DTPA dynamic renal imaging. 12
The presence of DR was diagnosed using digital retinal photographs (two eyes × seven fields), taken by using a TRC-NW7SF (Topcon Co., Tokyo, Japan) nonmydriatic camera at 45°. These photographs were subsequently examined independently by two qualified retinal photography graders following quality assurance protocols. The definition of graded DR is on the basis of fundus photography findings using the Early Treatment Diabetic Retinopathy Scale (ETDRS). 1
Prospective validation cohort
To further evaluate the prediction of PDR to AO-CAD, a cohort study is followed up from individuals with non-CAD detected in first stage retrospective set in Tongren Hospital (Beijing, China). To minimize the renal effect on the relationship of PDR with CAD, individuals with GFR <60 mL/min were excluded (NDR: n = 44, PDR: n = 55). Subsequently PDR participants with CAD (n = 21) and NDR with CAD (n = 29) were excluded. All remaining 202 patients were finally eligible and included for the prospective validation cohort (no-CAD in NDR: n = 138, no-CAD in PDR: n = 64) (Fig. 1B). Exclusion criteria were as follows: (1) history of known CAD, congestive heart failure, stroke, or any clinical indication for CAD; (2) limit life expectancy or liver disease; and (3) GFR <60ml/min·1.73m2. Patients with T2D who had finished clinical monitoring annually during the follow-up period were eligible. The primary end point was the detection of AO-CAD, or followed to the date of study closure on the 30th of August 2018. The mean duration of follow-up is 4.3 years.
Ethics statement
The study was conducted with the approval from the Ethics Committee of Beijing Tongren Hospital, Capital Medical University, and adhered to the tenets of the Declaration of Helsinki. In addition, the written informed consent was obtained from each participant.
Statistics
Data from continuous and categorical covariates were analyzed with t-tests, analysis of variance, χ2 tests, and multiple logistic regressions, respectively. Age, gender, smoking, HbAlc, and diabetic duration although not significantly associated with AO-CAD, together with significant variants, were included as covariates to enter regression model. Changes in the area under the receiver operating characteristic curve (AUC) were examined by integrating the presence or absence of PDR based on the traditional CV risk factors in the United Kingdom Prospective Diabetes Study (UKPDS) risk engine. 13,14 To determine the prediction of PDR to AO-CAD, a Cox proportional hazards model was used. Statistical significance was determined as a corrected value of P < 0.05. The 95% confidence intervals (CIs) for each parameter were calculated. The analyses were performed in STATA version 11.0 (StataCorp LP, Inc., College Station, TX). 15,16
Results
Characteristics of the retrospective case–control discovery set
Of the 1332 consecutive patients with T2D who were screened, 1126 had a HbA1c ≥7.0%. According to the screening criteria of the cross-sectional study, 211 NDR and 140 PDR were selected for investigation. The number of AO-CAD events in persons with NDR and PDR were 39 (18.5%) and 44 (31.5%), respectively. No significant differences were found in age, duration of known diabetes, body mass index (BMI), low-density lipoprotein cholesterol (LDL-C), except for blood pressure, fasting c-peptide, HbAlc, triglyceride (TG), and total cholesterol (TC) between PDR and NDR groups (Table 1).
Characteristics of the Individuals from the Retrospective Discovery Set
Statistical analyses were performed using Student's t-tests, ANOVA, and χ2 tests.
PDR, proliferative diabetic retinopathy; NDR, nondiabetic retinopathy; NS, not significant; DM, diabetes mellitus; BMI, body mass index; WHR, waist hip ratio; UA, uric acid; FBG, fasting blood glucose; TG, triglyceride; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic blood pressure; GFR, glomerular filtration rate; AO-CAD, asymptomatic obstructive coronary artery disease; ANOVA, analysis of variance; UAER, urinary albumin excretion rate (normal, <30mg/24h; micro, 30–300mg/24h; macro, > = 300mg/24h).
Identification of PDR to the risk of AO-CAD
Odds ratios between individuals with PDR and the risk of AO-CAD varied by different adjusted covariates, 2.53 (1.48–4.32) after only adjusting for age, gender; 2.36 (1.31–4.24) by additionally HbA1c level, duration of diabetes, TC, systolic blood pressure (SBP); 2.16 (1.10–4.31) by additionally urinary albumin excretion rate, and fasting C-peptide (Table 2). With the model estimating risk of AO-CAD based on traditional CV risks factors proposed by the UKPDS, the AUC analysis was improved from 0.583 in the model without PDR (95% CI, 0.51–0.66) to 0.697 in the model with PDR (95% CI, 0.641–0.752; P < 0.05, Fig. 2). Incremental association value for AO-CAD showed that the addition of PDR to base model that contained the covariate risk factors in this sample improved the C-statistic from 0.746 (95% CI, 0.681–0.811) to 0.762 (95% CI, 0.699–0.825; P = 0.73, Fig. 3).
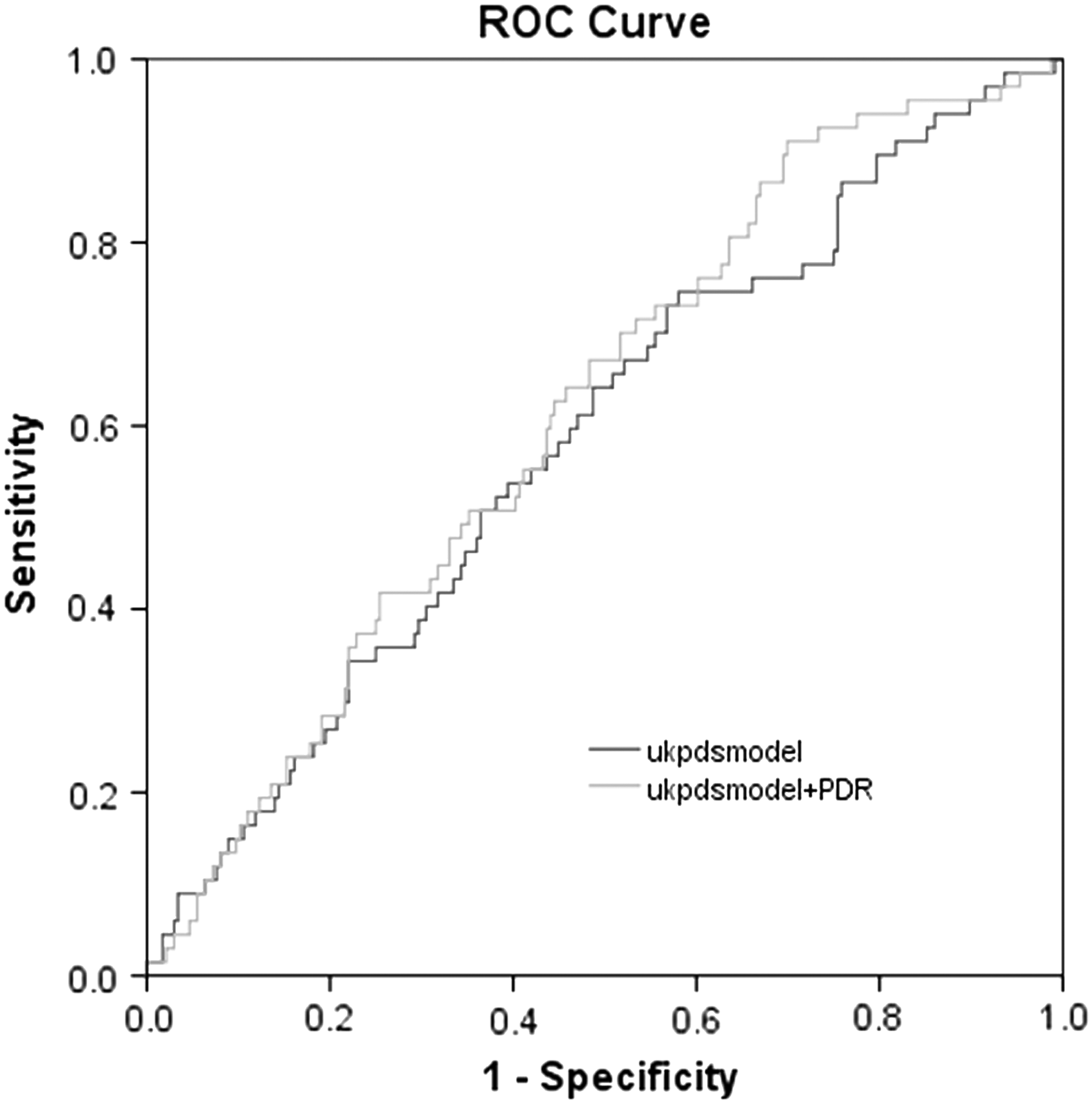
With the model estimating risk of AO-CAD based on traditional cardiovascular risks factors proposed by the UKPDS, the AUC was improved from 0.583 in the model without PDR (95% CI, 0.51–0.66; shown with dark line) to 0.697 in the model with PDR (95% CI, 0.641–0.752; shown with light line). 95% CI, 95% confidence interval; AUC, area under the receiver operating characteristic curve; UKPDS, United Kingdom Prospective Diabetes Study. AO-CAD, asymptomatic obstructive coronary artery disease.
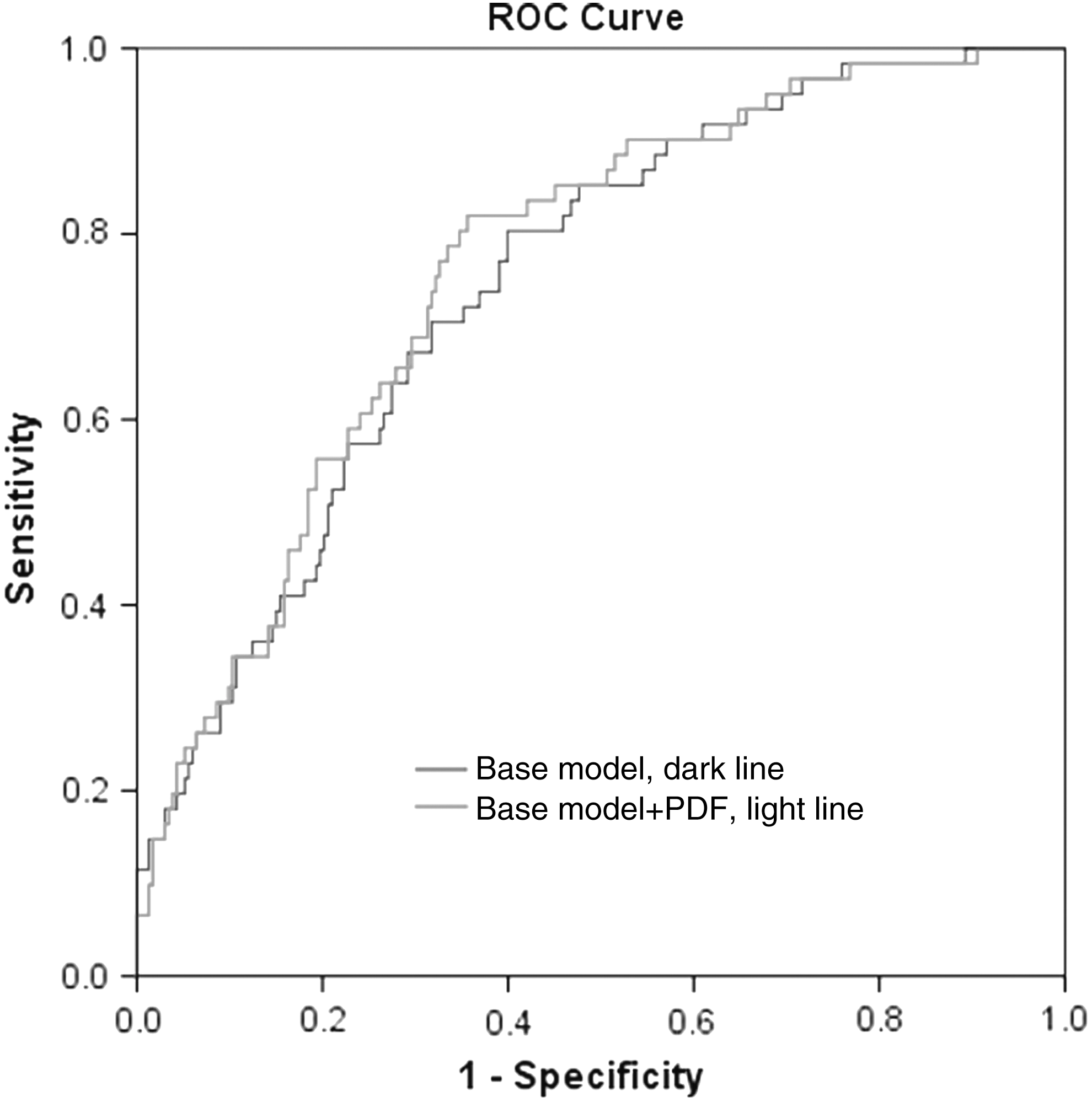
Incremental association value for AO-CAD showed that the addition of PDR to base model that contained the covariate risk factors in this sample improved the C-statistic from 0.746 (95% CI, 0.681–0.811) to 0.762 (95% CI, 0.699–0.825; P = 0.73).
Association Between Proliferative Diabetic Retinopathy and Asymptomatic Obstructive Coronary Artery Disease
Includes age and gender.
Additionally includes diabetic duration, HbA1c level, duration of diabetes, TC, and SBP.
Additionally includes UAER and fasting C-peptide.
95% CI, 95% confidence interval; HbA1c, glycated hemoglobin A1c.
Characteristics of patients grouped by PDR and AO-CAD
To minimize the interference of CKD to the development of CAD, only those with GFR >60 mL/min were included. As a result, individuals with complete data on PDR and CAD were eligible according to the inclusion and exclusion criteria (n = 252). (Fig. 1B). Individuals were divided into the following four categories (Table 3): NDR and CAD− (n = 138), NDR and CAD+ (n = 29), PDR and CAD− (n = 64), and PDR and CAD+ (n = 21).
Clinical Characteristics in This Research Individuals Stratified by Proliferative Diabetic Retinopathy and Asymptomatic Obstructive Coronary Artery Disease
Data are mean ± SD or median (25th and 75th intervals) unless otherwise indicated. Statistical analyses were by Student's t-test or Mann–Whitney U test.
Star key P < 0.05, NDR/AO-CAD− versus other three groups. Statistical analyses were performed using Student's t-tests, ANOVA, and χ2 tests.
DBP, diastolic blood pressure; Cr, creatinine; LDL-C, LDL cholesterol; HDL-C, HDL cholesterol; ATA, antithyroid peroxidase antibody; ATG, anti-thyroglobulin antibody; SD, standard deviation.
No significant differences were found in gender, waist hip ratio, BMI, urine acid, serum creatinine, LDL-C, and high-density lipoprotein cholesterol among groups (seen in Table 3). SBP and DBP were lower in NDR/CAD− group compared with other three groups. In addition, HbAlc, TG, and antithyroid peroxidase antibody (ATA) were higher (P < 0.01) in those with PDR compared with those with NDR. Interestingly, the lowest C-peptide and smoking was observed in those with PDR (mean: 0.82 ± 0.50; 29%) compared with those with NDR (mean: 1.03 ± 0.64; 41%; P = 0.012, P = 0.04).
Cumulative incidence of AO-CAD in a prospective validation cohort
In this study, 202 individuals were followed up for 4.3 years, including 138 patients in NDR group and 64 patients in PDR group. No difference of conventional CV risk factors was observed among non-CAD individuals between included and excluded (Fig. 1B). All patients finished the follow-up study. Total of 45 AO-CAD events occurred in this study, including 23 AO-CAD events in NDR group and 22 AO-CAD events in PDR group. A multivariable Cox proportional hazard regression analysis was performed to determine the factors that affected the progression to AO-CAD. After adjustment for age, gender, C-peptide, smoking, HbAlc, TG, ATA, and SBP, the cumulative risk of AO-CAD was significantly higher in the PDR group compared with risk in NDR group (hazard ratio = 3.07, 95% CI 1.81–5.21, P < 0.001) (Fig. 4).
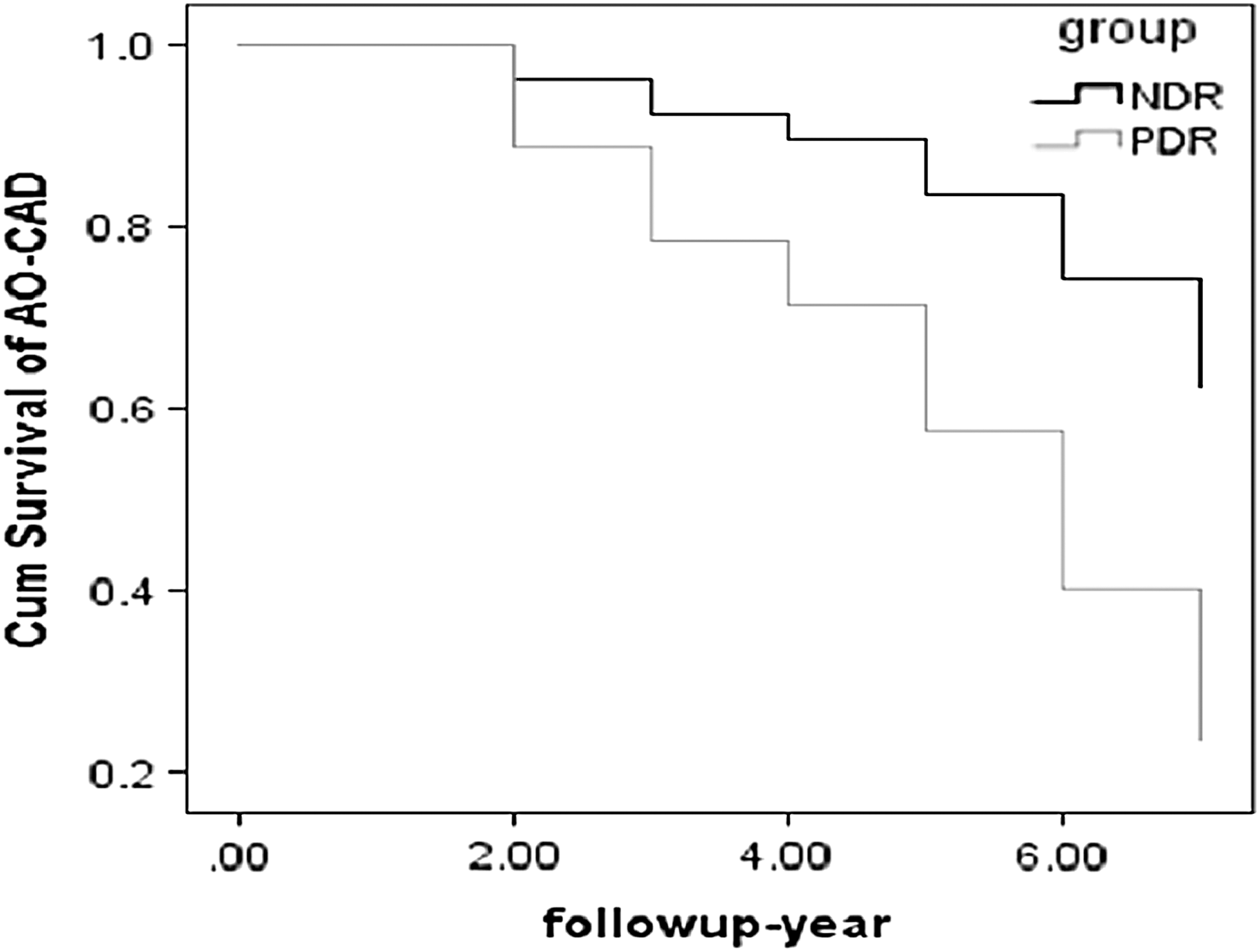
In this prospective validation cohort, 202 individuals were followed up for 4.3 years, including 138 patients in NDR group and 64 patients in PDR group. Total of 45 AO-CAD events occurred in this study, including 23 AO-CAD events in NDR group and 22 AO-CAD events in PDR group. Adjusted by covariants, the cumulative risk of AO-CAD was significantly higher in the PDR group compared with risk in NDR group (HR = 3.07, 95% CI, 1.81–5.21, P < 0.001). HR, hazard ratio.
Discussions
This study analyzed data from individuals with unknown CAD, the retrospective discovery set, and patients with non-CAD in the prospective validation cohort. Findings from this study indicated that PDR strongly predicted AO-CAD in patients with T2D, even after adjustment for multiple covariates, which might contribute to the early diagnosis of CAD. To our knowledge, this is the first research to explore the prediction of PDR to AO-CAD in individuals with T2D.
Latest article showed that patients with T2D and PDR had an increased risk of incident CAD. 17 Once diabetic complications progressed, patients might have suffered from severe autonomic denervation of the heart, accounting for their asymptomatic presentation. 18 While the relationship of PDR to asymptomatic CAD remains unclear, especially to asymptomatic obstructive CAD. 19 It has been suggested that microvascular pathology plays an important role in macrovascular disease. 20,21 Our findings suggest that the presence of PDR may predict the AO-CAD in patients with T2D. Given that these associations remained even after adjusting conventional CV risk factors, some mechanisms underlying atherosclerosis, notably endothelial dysfunction, low-grade inflammation, and rheological abnormalities, are also relevant to diabetic microvascular disease. 22 Furthermore, in support of this hypothesis, histopathological findings have shown that small-vessel disease present in the retina was also evident in the heart of individuals with diabetes. 23,24 Our further analysis of identification of PDR to ischemic nonobstructive microvascular dysfunctional CAD are ongoing.
Another advantage of this research is the diagnosis of the AO-CAD by coronary angiography, not evaluation of ECG or CAD history, which minimized the error of misclassification of AO-CAD and further improved the reliability of this research. Clinical profile stratified by PDR and CAD showed that TG was higher in the PDR group, compared with NDR group, and higher in PDR/CAD+ group than PDR/CAD−. These results were in accordance with the evidence that the addition of fenofibrate to best treatment not only decreased the risk of progression of retinopathy by 40%, 25 but also provided additional reduction in CV risk in patients with dyslipidemia at baseline. 26 Lowest fasting C peptide in PDR group appeared, compared with the NDR group, which was observed in former research. 27
CV risk scores developed for the general population have been shown to underestimate the risk of incidence of CAD in the T2D population, 28 which was in accordance to our findings (UKPDS: AUC 0.583, 95% CI 0.51–0.66; UKPDS+PDR: AUC 0.697, 95% CI 0.641–0.752). The addition of PDR to the traditional risk factors improved the identification of PDR to AO-CAD in T2D group, which highlights the potential of individual PDR to improve CAD risk stratification. Recent study reported that PDR has no additional effect to classical CAD risk factors to identify CAD in T2D patients. 29 Although there is still noise on effect of PDR over traditional CV risk factors, possibly because of differences in the exposures compared (e.g., nonproliferative DR vs. PDR), and diagnosis of CAD (e.g., computed tomography angiography vs. coronary angiography).
This study has several limitations. First, genetic variants potentially associated with PDR and CAD were not specifically assessed in this analysis. Second, because of the limited sample size in this study, present sample size led to wider CIs and loss of statistical significance. However, the point estimates remained stable. Third, the lack of assessment of cardiac autonomic neuropathy (CAN) should be acknowledged in our study. Asymptomatic CAD may be related to CAN, which is strongly related to glucose control and diabetic duration, commonly recognized as risk factors for microvascular disease. 30 Despite no description of CAN, no difference was shown in glucose control and diabetic duration in this study. Fourth, the nonobstructive microcirculation dysfunction CAD could not be detected by coronary angiography, which might be misclassified into the non-CAD group to follow-up. In this circumstance, our results of prediction of PDR to the AO-CAD remain still significant.
Conclusion
This exploratory study suggests the predictive value of PDR to AO-CAD. Understanding whether PDR has a higher risk of AO-CAD will allow diabetologist to more effectively counsel patients.
Footnotes
Acknowledgments
This study was supported by the National Science Foundation Council of China (nos. 81870556, 81670738, and 81561128015), Beijing Municipal Administration of Hospital's Youth Programme (QML20170204), Beijing Tongren Hospital Fund (no. TRYY-KYJJ-2017-003), and Excellent Talents in Dongcheng District of Beijing. The authors thank all the participants and staff in this study.
Authors' Contributions
J.-B.Z., L.Q., and J.-K.Y. have contributed to the design of the study, analysis and interpretation of data, and prepared all figures and tables. J.-B.Z. and X.-R.Z. drafted a part of the article. X.-R.Z., W.Z., L.Y., H.-B.L., and L.Q. took part in analyzing data and drafting a part of the article. All authors reviewed the article.
Author Disclosure Statement
The authors declare that they have no competing interests.