
Abstract
Background:
To assess the impact of the lymph node dissection (LND) technique on short- and long-term complications. This retrospective review included patients who underwent hysterectomy, oophorectomy, and pelvic ± para-aortic LND for gynecological malignancies (cervical, endometrial, and ovarian) from 2020 to 2022 in our Gynecological Oncology Surgery clinic.
Methods and Results:
Among 147 patients who underwent pelvic LND for gynecological malignancy, 48 had procedures involving scissors and 99 had procedures involving unipolar cautery. There was no significant difference in the numbers of extracted pelvic and para-aortic lymph nodes between groups. The extents of LND were comparable between the scissors and unipolar cautery groups (p = 0.945). The scissors group exhibited less fluid drainage between days 2 and 5 postoperatively (1300 [600–3100] vs 1800 [600–3400]; p = 0.038). In terms of primary early and late clinical outcomes, there were no significant differences in lymphocele (16.7% vs 15.2%; p = 0.494) and lymphedema (18.8% vs 17.2%; p = 0.491) rates between groups.
Conclusions:
After retroperitoneal LND for gynecological malignancy, early complications such as lymphocele and late complications such as lower extremity lymphedema did not significantly differ between procedures using cold scissors and procedures using unipolar cautery.
Introduction
Retroperitoneal lymph node dissection (LND) has a central role in the surgical treatment of cervical, endometrial, and ovarian cancers, which are among the most common cancers in the genital system. The lymphatic system facilitates the removal of fluid from interstitial compartments into the vasculature. Although LND has considerable diagnostic and therapeutic value, it can lead to short-term complications such as lymphatic leakage and long-term complications such as lymphedema. Some of these complications can be severe, impairing mobility and affecting quality of life. To reduce the risk of these complications, the National Comprehensive Cancer Network guidelines advocate sentinel LND in endometrial cancer as a preferred strategy. 1 However, many surgeons continue to perform systematic pelvic and para-aortic LND for high-risk tumors or because of technical limitations.
A lymphocyst constitutes a large volume of lymphatic fluid in the retroperitoneal space, often caused by surgical dissection and insufficient closure of afferent lymphatic vessels.2,3 Lymphocysts, possible short- and medium-term complications of pelvic LND, are generally asymptomatic. However, in rare instances, they can become infectious or considerably enlarged, leading to pressure on adjacent organs. Lymphedema arises from the accumulation of protein-rich exudate underneath the skin of the extremities when lymphatic return to the venous system is inadequate. The incidence of lymphedema, lower in retrospective studies and higher in prospective studies, varies between 2% and 48%.4–6 No definitive cure for lymphedema exists, underscoring the importance of prevention. Factors such as the number of lymph nodes (LNs) extracted and subsequent use of radiotherapy have been identified as major risk factors for lymphedema.7,8 LND can be executed using thermal devices (e.g., unipolar/bipolar cautery) or Metzenbaum scissors. This study explored the incidence of lymphedema and other complications in patients who underwent LND and the impact of LND technique on short- and long-term complications.
Materials and Methods
This retrospective study included patients who underwent hysterectomy, oophorectomy, and pelvic ± para-aortic LND for gynecological malignancy (cervical, endometrial, and ovarian) between 2020 and 2022 at the Gynecological Oncology Surgery Clinic. Patients were excluded if they had lymphatic system dysfunction, chronic immune disease, bowel resection, a history of interval debulking surgery, or a history of fertility preservation procedures. Additionally, patients were excluded if they had conditions that mimic lymphedema (e.g., chronic venous insufficiency, heart failure, renal failure, or hypoalbuminemia). Finally, patients with partial or total peritonectomy were excluded because the peritoneum contributes to the postoperative absorption of lymphatic and hemorrhagic fluid. The patient inclusion flowchart is depicted in Figure 1. The University Clinical Research Ethics Committee approved this study protocol (Date: 09/03/2022, Number: 2022/199). All procedures adhered to the ethical standards of the institutional and/or national research committee, as well as the Declaration of Helsinki (2013 revision) and its subsequent amendments or comparable ethical standards.
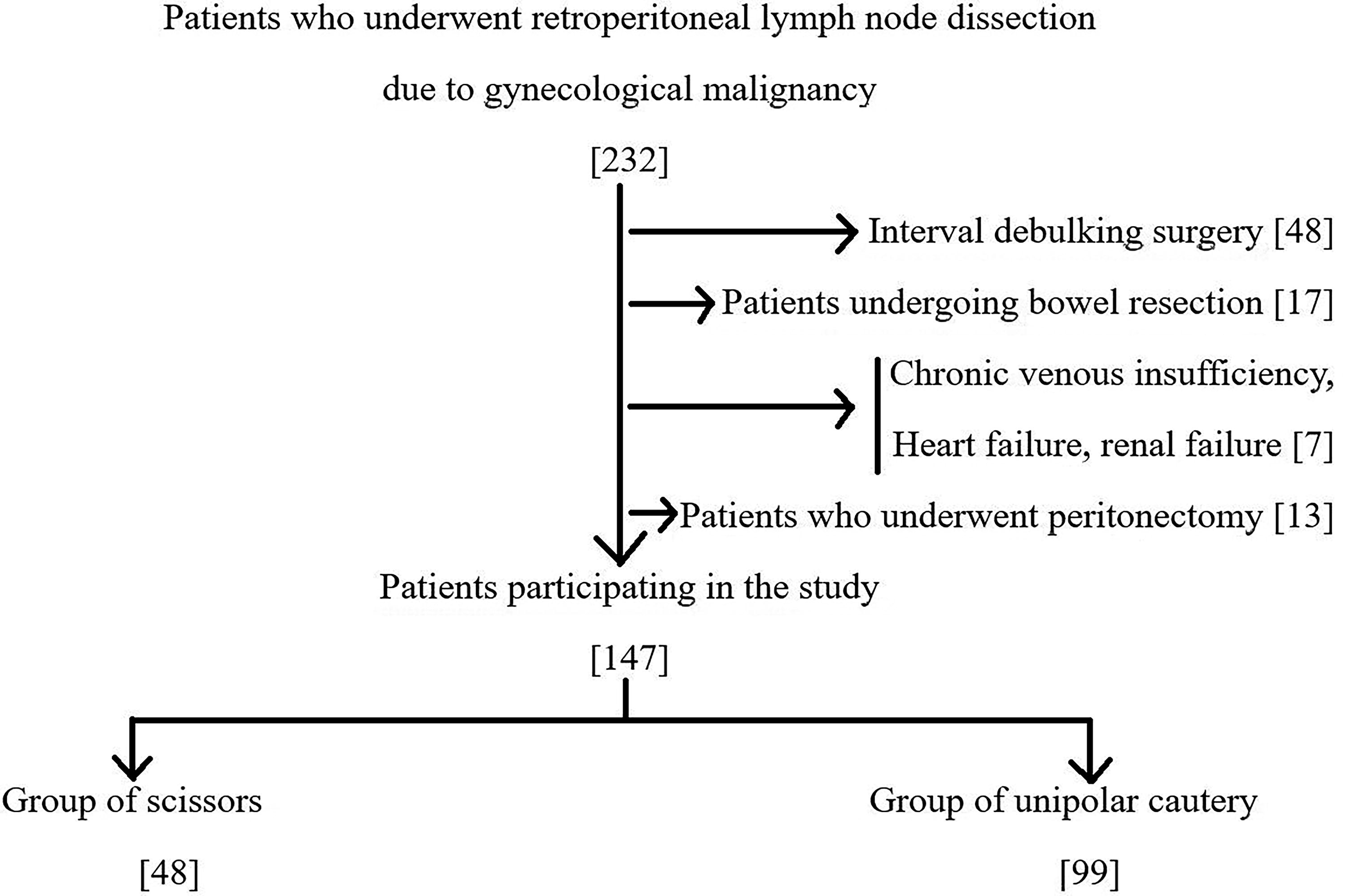
The flowchart of the patients included in the study.
All surgeries were performed by experienced gynecological surgical oncologists. Cervical and endometrial cancer diagnoses were established through preoperative biopsies; ovarian cancer was diagnosed via frozen sections. A vertical midline incision below the navel was the primary surgical approach, with extension above the navel when necessary. The following areas were examined: intestinal mesentery and serosa, liver capsule, stomach, paracolic areas, Douglas peritoneum, omentum, and subdiaphragmatic peritoneum. Patients underwent hysterectomy and bilateral oophorectomy. Extrafacial hysterectomy (type 1) comprised full excision of the uterus and cervix, while the parametrium and paravaginal tissues remained intact. Radical hysterectomy (type 3) encompassed removal of the cervix, proximal vagina, parametrial tissues, and paracervical tissues. Omentectomy was performed when necessary. Endometrial cancer management varied, particularly regarding the role of LND. Although LND was omitted in some patients, others underwent bilateral pelvic LND; a few patients underwent para-aortic LND. Such variations were selected by individual surgeons during the study. Cervical cancer patients underwent pelvic and para-aortic LND up to the inferior mesenteric artery; ovarian cancer patients underwent pelvic and para-aortic bulky LN sampling up to the left renal vein. Gynecological pathologists performed pathological assessments. The numbers of extracted LNs were recorded. Pelvic LND comprised the removal of lymphatic tissue over the external and common iliac vessels, as well as within the obturator fossa. Para-aortic LND was characterized by the extraction of lymphatic tissue beginning at the bifurcation above the inferior vena cava and aorta and then extending below the left renal vein. If bulky LNs were not detected during pelvic LND, LNs distal to the deep circumflex external iliac vein and below the obturator nerve were not removed. Absorbable sutures or hemoclips were utilized as necessary to secure lymphatic vessels. They were also used to connect the distal pelvic LND region in all cases. LND was performed by unipolar cautery or Metzenbaum scissors. The use of unipolar cautery (BÖ) alone or Metzenbaum scissors (İSS) alone for LND was recorded by another observing surgeon (VG). Cases in which unipolar cautery and Metzenbaum scissors were used together for LND were not included in the study. After LND, no hemostatics or adhesives (e.g., fibrin glue) were applied.
A rubber drain (lumen diameter 4 mm, total diameter 6 mm) was placed into the abdomen (Douglas gap) of all patients to monitor for bleeding or leakage in the early postoperative period. Daily drain volumes were measured using a 1000-cc non-negative pressure rubber drain. Comparisons of daily drainage and hospital stays were made between the two groups. The total lymphatic drainage volume comprised the sum of daily drainage from day 2 to day 5 postoperatively. The drain was removed when daily discharge from the abdomen decreased to <200 cc. Chylous ascites was diagnosed according to the presence of uninfected, milky-colored peritoneal fluid with a volume >100 mL/day and a triglyceride concentration >110 mg/dL. A drainage catheter was maintained until the daily output was <200 mL and the fluid appeared clear and pink (serosanguinous). White blood cell counts and body temperature measurements helped to exclude potential infections (e.g., bacterial peritonitis). The secondary outcome of this study was the incidence of lymphocele. Lymphocysts were diagnosed on the basis of ultrasonographic findings comprising fluid-filled cystic structures with various shapes, structures, and echogenicities. Computed tomography or magnetic resonance imaging was utilized for clarity, as necessary. For symptomatic lymphocele, interventions such as percutaneous drainage were performed. The tertiary outcome of this study was the incidence of lymphedema within the first 6 months postoperatively. For the diagnosis of unilateral lymphedema, the unaffected leg was used as a reference. For the diagnosis of bilateral lymphedema, specific skin alterations (e.g., changes in limb volume, edema, peau d'orange, cutaneous fibrosis) were considered indicative of lymphedema because a “normal” limb was unavailable for comparison. 9 Lymphedema grading adhered to the guidelines of the International Society of Lymphology. 10 All detected cases of lymphedema were grade 1.
All participants received intravenous 2 g cefazolin as prophylaxis; extended surgeries (>3 hours) required additional doses. Patients also received thrombosis prophylaxis comprising low-molecular-weight heparin. In our facility, this prophylaxis begins 12 hours before surgery and continues until postoperative day 28. Dose and duration were customized according to the patient’s body mass index and any relevant risk factors, such as a history of embolism, atrial fibrillation, or cardiovascular disease. Observations until 6 months postoperatively were recorded for this study.
Numerical values were compared using one-way analysis of variance; they are presented as means ± standard deviations or as medians. Categorical variables are shown as frequencies and percentages. The chi-squared test was used to analyze categorical data. The Pearson chi-squared test was utilized when <20% of the groups contained fewer than five patients. Fisher’s exact test was used if the proportion of such groups exceeded 20% and the minimum expected count value was <5. Data recording and statistical analyses were performed with SPSS software (ver. 17, SPSS, Inc., Chicago, IL, USA). p-Values <0.05 were considered statistically significant.
Results
This study included 147 patients who underwent pelvic LND for gynecological malignancy; LND was performed with scissors in 48 patients and with unipolar cautery in 99 patients. The numbers of extracted pelvic (22 [range 10–37] vs 24 [range 10–39]; p = 0.259) and para-aortic LNs (8.5 [range 2–19] vs 10 [range 1–24]; p = 0.533) were similar between the two groups. There was no significant difference in extent of LND between the scissors and unipolar cautery groups (p = 0.945). In the scissors group, 13 (27.1%) patients received adjuvant radiotherapy; 9 (18.8%) patients received both adjuvant chemotherapy and radiotherapy. In the unipolar cautery group, 24 (24.2%) patients received adjuvant radiotherapy, whereas 20 (20.2%) patients received both adjuvant chemotherapy and radiotherapy (p = 0.837). Demographic data relevant to this study are presented in Table 1.
Comparison of Demographic Data According to Lymphadenectomy Application Methods
Mean ± standard deviation.
Median (min–max).
BMI, body mass index; CT, chemotherapy; LN, lymph node; RT, radiotherapy.
The primary and secondary outcomes of the study are shown in Table 2. Fluid drainage between days 2 and 5 postoperatively was lower in the scissors group (1300 mL [range 600–3100 mL] vs 1800 mL [range 600–3400 mL]; p = 0.038). The median times until drain removal from the abdomen were 4 (range 3–9) days in the scissors group and 5 (range 3–9) days in the unipolar cautery group (p = 0.011). In terms of the main early and late clinical outcomes (lymphocele [16.7% vs 15.2%; p = 0.494] and lymphedema [18.8% vs 17.2%; p = 0.491]), there were no significant differences between the two groups.
Comparison of Outcomes According to Lymphadenectomy Application Methods
Median (min–max).
Discussion
In the present study, we compared LND techniques with respect to lymphatic complications among patients who underwent hysterectomy, oophorectomy, and pelvic ± para-aortic LND for gynecological malignancy. To our knowledge, no other published study has compared LND techniques in terms of short- and long-term complications. With respect to postoperative follow-up parameters, fluid drainage between days 2 and 5 was lower in the cold scissors group than in the unipolar cautery group. The duration of drain usage was also shorter in the cold scissors group. Nevertheless, short- and long-term outcomes did not significantly differ between the cold scissors and unipolar cautery groups in terms of chylous ascites, lymphocele, and lower extremity lymphedema.
After gynecological oncology surgeries, accumulated fluid in the abdomen predominantly consists of surgical wound exudates and LND-related unclosed lymphatic vessels. In our cohort, both the volume of fluid drained and the duration of drain usage were lower in the scissors group than in the unipolar cautery group. Chylous ascites is characterized by the postoperative leakage of triglyceride- and protein-rich lymphatic fluid into the peritoneal cavity. 11 The incidence of chylous ascites after retroperitoneal LND is between 0.1% and 9.0%.11,12 Consistent with published literature, we found that chylous ascites was rare (2.0%) and did not significantly differ between groups (4.2% for scissors vs 1.0% for unipolar cautery; p = 0.204).
Lymphocele, the most common postoperative complication of LND, has an incidence of 1–40%.3,13 The incidence of lymphocele in our patients (15.2–16.7%) is similar to previous reports. Lymphocele is caused by postoperative leakage from afferent lymphatic vessels. Factors such as the number of LNs excised, LN involvement, anticoagulant use, and supplementary radiotherapy have been identified as risk factors for lymphocyst development.2,3,13 The extent of para-aortic LND is not considered a risk factor for lymphocele formation. 6 Numerous prophylactic strategies have been proposed to prevent lymphocyst development; these include placement of an abdominal drain, maintenance of pelvic peritoneal patency, ligation of primary lymphatic vessels draining lower extremities, use of fibrin glue, and omentoplasty.3,13,14 In our center, pelvic LND is routinely conducted; the deep circumflex iliac lymph vessel (i.e., the most caudal boundary) is sealed with hemoclips or a LigaSure device. In terms of LND technique and lymphocele formation, the main hypothesis of this study, we found no significant differences between groups. Thus, we conclude that scissors and unipolar cautery have similar efficacy in sealing lymphatic vessels.
Lymphedema is the most common long-term complication after retroperitoneal lymphadenectomy.4,15 Major factors contributing to lymphedema onset include the number of LNs dissected and the performance of deep circumflex iliac LND.4,9,16,17 To reduce the risk of lymphedema, prophylactic compression garments are recommended. 5 Considering that the incidence of metastasis to the circumflex iliac LN in gynecological cancers is ∼1%, the dissection of these LNs may be unnecessary. 4 In our institution, non-bulky circumflex iliac LNs typically are not excised, and compression stockings are consistently recommended to all patients. Assessment of the extent of LND and median number of LNs excised in both groups revealed uniformity between groups. Moreover, there was no difference in terms of lymphedema incidence. Based on our analysis of these complication rates, we suspect that the choice of LND technique is unimportant; surgeons should choose the method with which they are most familiar.
This study had some limitations. First, it used a retrospective design. Second, it had a relatively small number of patients, which may limit the generalizability of the findings. Finally, the use of more precise diagnostic tools to identify lymphedema might have been beneficial. Despite these limitations, this study benefitted from our center’s robust follow-up system for patients with malignancies. All relevant patient data are meticulously recorded by specialist physicians and promptly entered into the appropriate database. Thus, the data-driven insights from this study have high clinical value.
Conclusions
In conclusion, we found that the incidences of lymphocele, an early postoperative complication of retroperitoneal LND for gynecological malignancy, and lower extremity lymphedema, a subsequent complication, remained consistent regardless of whether the LND procedure involved cold scissors or unipolar cautery. More extensive, prospective studies with larger patient populations will improve potential insights and offer more definitive conclusions.
Footnotes
Authors’ Contributions
V.G.: Manuscript writing/editing. M.D.: Data collection or management. İ.A.Ö: Editing, Data analysis. F.Ç.: Data analysis and statistics. E.Ş.: Data collection. B.Ö.: Protocol/project development. İ.S.S.: Protocol/project development. K.G.: Editing.
Author Disclosure Statement
All authors declare no competing financial interests exist.
Funding Information
No funding was received for this article.