
Abstract
Background:
The purpose of this study was to measure the effects of lymphoscintigraphically guided manual lymphatic drainage (LG-MLD) and to compare it with standardized manual lymphatic drainage (St-MLD).
Materials and Methods:
Fifty-two patients with lymphedema of the upper limb who underwent lymphoscintigraphy were randomly allocated into two groups. Following the phase of physical activity, the control group underwent two phases of St-MLD as the experimental group underwent a first phase of St-MLD followed by a second phase of LG-MLD. Areas of interest were then selected [in particular, dermal backflow (DBF) and axillary lymph nodes (LN)], radioactive activities were quantified for each of these areas.
Results:
If a first phase of St-MLD increased the LN activity by 28% on average, the findings indicated that for the second phase of DLM, LG-MLD was 19% more efficient than St-MLD in increasing LN activity. If a period of rest does not influence the lymph charge of DBF areas, physical activity leads to an average activity increase of 17%, whereas LG-MLD and St-MLD lead to an activity decrease of 11%.
Conclusions:
For patients with lymphedema, the findings indicate that MLD can increase the lymphatic flow toward the lymphatic nodes by 28% on average and can decrease the charge in the areas of DBF by 11% on average. Moreover, lymphoscintigraphy can be an important therapeutic tool because LG-MLD significantly increases lymphatic flow by 19% more than St-MLD. Concerning the areas of DBF, the LG-MLD and St-MLD decrease the charge in these areas with the same intensity.
Introduction
Lymphedema is a chronic evolving disease that can have many detrimental impacts on the physical and psychosocial aspects of the patient's life if not treated. Although this disease is a common condition affecting millions of people worldwide, its true rate remains unknown. 1 According to the 2020 consensus of the International Society of Lymphology (ISL), lymphedema is an external (and/or internal) manifestation of lymphatic system insufficiency and deranged lymph transport. 2 Extracellular protein-rich fluid stasis owing to lymphatic insufficiency leads to swelling of the affected body part and later to chronic inflammation 3 ). Lymphedemas are classified into two types: primary lymphedemas (congenital, praecox, or tarda), which follow a dysplasia of the lymphatic system (lymphatic vessels or nodes), and secondary lymphedemas, which follow damage to the lymphatic system.
Traumatism, infection, neoplastic invasion, and parasitic infection (filariasis) are numerous causes of secondary lymphedema, but in developed countries, the major causes are lymphadenectomy, radiotherapy, and chemotherapy for oncological treatment.4,5 With the highest incidence for European women in 2020, with a frequency of 200 new cases diagnosed per year for 100,000 women according to the Global Cancer Observatory, oncological treatment for breast cancer remains the most common cause of lymphedema in Europe. Depending on the invasiveness of the surgery, the addition of chemotherapy and/or radiotherapy, the extent of lymph node dissection and the tumor burden, the average Breast Cancer Related Lymphedema (BCRL) incidence ranges from 7% to 45%. 6
Indeed, 50% of breast cancers are diagnosed with lymphatic node metastatic invasion. 7 In those cases, it is essential to prevent mortality over morbidity by applying complete axillary lymph node dissection, thereby increasing the risk of developing lymphedema. Usually, the clinical examination and clinical history are sufficient to diagnose lymphedema, but in some more complex cases where the clinical history remains unclear, proper imaging is necessary to objectify lymphatic insufficiency.8,9 Even if there are many types of imaging for the lymphatic system, such as MRI 10 and lymphofluoroscopy, 11 lymphoscintigraphy remains the gold standard for lymphedema diagnosis and the only imaging modality that can quantify physiological lymphatic flow. With that examination, the nuclearist can obtain valuable information concerning the patient's physiological drainage and guide him toward proper treatment.
Following the 2020 consensus of the ISL on lymphedema,
2
the major treatment modality is physical treatment with complex decongestive therapy. It consists of a two-phased physical treatment with skin care, manual lymphatic drainage (MLD), multilayered bandages, physical exercises, and compressive garments.
12
MLD is a very specific massage technique for which the purpose is to improve lymphatic drainage
13
by increasing lymph vessel contractility and by facilitating edema resorption.14–16
Although MLD remains an important part of the physical treatment for lymphedema, there is still a lack of evidence regarding its efficiency.17,18 Moreover, in general physical therapy, the practitioner has to adapt the treatment to the patient and not to the pathology to reach the best efficiency, which is very difficult in cases of lymphedema for two reasons:
Every lymphedema is different, and the only part of the pathology that can be assessed by the physical therapist is the swelling, which is not always representative of the lymphatic drainage. The only way to assess the lymphatic drainage of the patient is through an imaging system for which lymphoscintigraphy is the gold standard. Although lymphoscintigraphy can provide valuable information, the physical therapist rarely has access to the patient's imaging.
Lymphoscintigraphy could be the way to assess the true efficiency of the MLD technique as well as the way to improve the physical treatment and to adapt it to the patient's physiology by becoming a therapeutic tool. In 2004, Jung et al. showed that complex decongestive therapy was improving the lymphatic drainage on patients undergoing lymphoscintigraphy. 19 For that purpose, we used lymphoscintigraphy for lymphatic insufficiency imaging to quantify the effect of a 15-minute MLD period on the lymphedematous upper limb of a population of patients with BCRL. We also aimed to determine whether lymphoscintigraphy can provide information to the physical therapist to treatment by comparing the efficiency of a standardized MLD (St-MLD) with a lymphoscintigraphically guided MLD (LG-MLD).
Materials and Methods
For this research, 52 lymphoscintigraphical clinical imaging examination of patients presenting with secondary upper limb lymphedema were analyzed at the Jules Bordet Institute, Brussels, Belgium. All medical data and medical information regarding the patients included in this study were used in agreement with the rules of conduct dictated by the institution and in accordance with the ethics committee of the Jules Bordet Institute (ethics committee No. 2048). Therefore, no informed consent was needed. As given in Table 1, every lymphoscintigraphy was performed by the same investigator following the classical upper limb lymphoscintigraphical protocol 20 approved by the Belgian Society of Nuclear Medicine and recognized by the Belgian national health insurance system (Table 1). Patients with a painful shoulder owing to inflammation, an osteoarticular disorder, or pain following trauma to the upper limb have not benefited from MLD to avoid painful manipulation during imaging. Before every lymphoscintigraphy, patients need to be aware of the protocol and the clinical importance of following it. Patients are advised to go to the bathroom before the examination, and elastic stockings are removed before the injection and during the examination. Patients are then positioned in dorsal decubitus on the examination bed, and the injections are realized at least 5 minutes after the positioning of the patient. The lymphoscintigraphy apparatus used in this study is an SMV ST-XLi from GE Healthcare (Little Chalfont, United Kingdom). The injected solution was made by adding 1110 MBq of 99mTcO4− to one vial of nanosized human serum albumin colloids Nanocoll® (GE Healthcare, Little Chalfont, United Kingdom) and 0.9% saline up to a final volume of 2.0 mL. A volume of 0.2 cc (3 mCIs per syringe) was injected subcutaneously into both first interdigital spaces of the hands.
Classical Upper Limb Superficial Lymphatic System 3 Phased Lymphoscintigraphical Investigation Protocol
Following the third phase of the lymphoscintigraphical assessment, patients were randomized into two groups: a control group and a test group. The control group underwent two consecutive phases of 15-minute standardized manual lymphatic drainage (St-MLD) and the test group underwent an enhanced protocol with a first phase of 15-minute standardized MLD followed by a second phase of 15-minute LG-MLD. During the MLD phase and imaging, the patient was asked to stay still. The St-MLD was standardized following the Leduc method principles and by considering the injection site as an experimental edema. St-MLD began with resorption maneuvers on the injection site followed by distoproximal inciting maneuvers toward the root of the upper limb and then inciting maneuvers on the axilla and Mascagni lymphatic pathways. The purpose of this phase was to fill the lymphatic collectors with the tracer and to globally stimulate the upper limb lymphatic system to increase the lymphatic flow. LG-MLD corresponds to a St-MLD with 3 adaptations of the MLD to the patient imaging by lymphoscintigraphy:
Application of resorption maneuvers when passing over an area of dermal backflow (DBF).
Pressure of the maneuvers increased and muscle mobilization occurred when passing over an area with deep lymphatic vessels or deep lymphatic node visualization.
Insistence on the lymphatic outlet path at the root of the limb. Radioactivity quantification was performed on every region of interest (injection site at the level of the hands, lymphatic nodes, and areas of DBF) of both upper limbs on the lymphoscintigraphical imaging (Fig. 1).
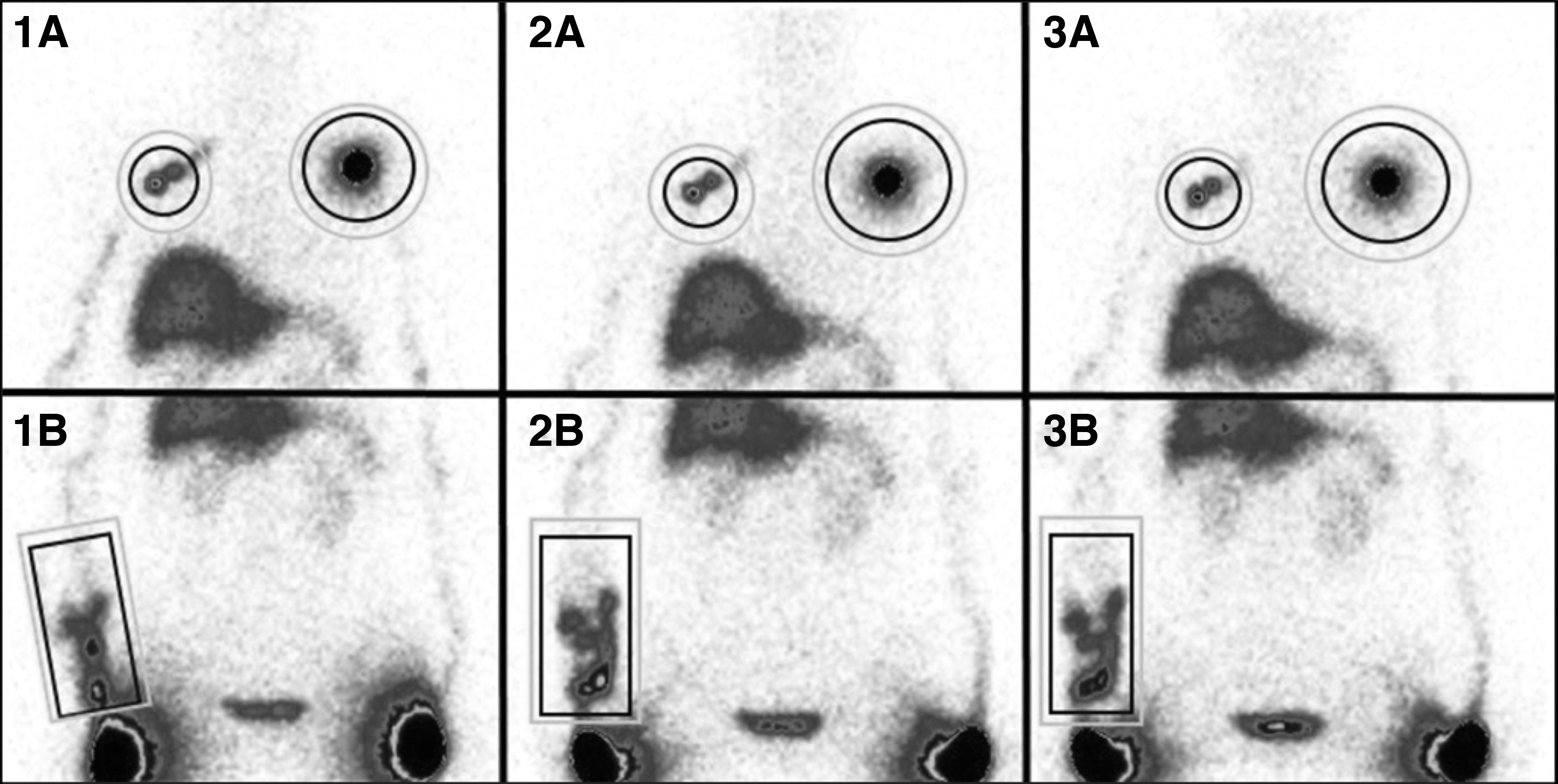
Example of radioactivity quantification made on lymphatic nodes and areas of dermal backflow on axillary centered imaging
Data were then:
Corrected to remove the nonspecific background noise (ambient radioactivity and diffusion of the tracer radioactivity).
Corrected to consider the disintegration of the tracer.
Normalized to a percentage of the injection site.
Transformed into a ratio of increased activity with the following formula:
where RIA is the ratio of increased activity for the phase of MLD investigated; A3, activity count at the end of the third phase of lymphoscintigraphy; AMLD, activity count for the phase of MLD investigated.
First, statistical analysis was performed by comparing the effects of a period of rest, a period of physical activity, and a period of MLD on the areas of DBF using a Kruskal–Wallis test with Dunn's multiple comparison test. Then, we compared a 15-minute period of rest for the lymphatic nodes of the healthy upper limb and a 15-minute period of rest for the lymphatic nodes of the edematous upper limb. Finally, we compared the effects of the St-MLD and the LG-MLD.
Statistical significance was determined as follows.
A value of p ≥ 0.05 indicated that no significance was reached, and the null hypothesis was not rejected. A p-value between 0.05 and 0.01 or equal to 0.01 indicated that significance was reached (*), and the null hypothesis was rejected. A p-value between 0.01 and 0.001 or equal to 0.001 indicated that high significance was reached (**), and the null hypothesis was rejected. A value of p < 0.001 indicated that very high significance was reached (***), and the null hypothesis was rejected. A value of p < 0.0001 indicated that the highest significance was reached (****), and the null hypothesis was rejected.
Results
Concerning the areas of DBF, the results regarding the ratio of increased activity of the two consecutive phases of MLD show two facts:
First, when comparing a 15-minute period of resting, a 15-minute period of physical activity, and a 15-minute period of MLD, we can see that their effects are significantly different (Kruskal–Wallis test, p < 0.0001). If a 15-minute period of rest tends to slightly increase the charge in the areas of DBF activity on average by ∼4%, physical activity seems to clearly increase the charge in the areas of DBF on average by ∼17%. In contrast, it seems that a 15-minute period of MLD generates a different response by decreasing the charge in the areas of DBF on average by ∼11% (Fig. 2).
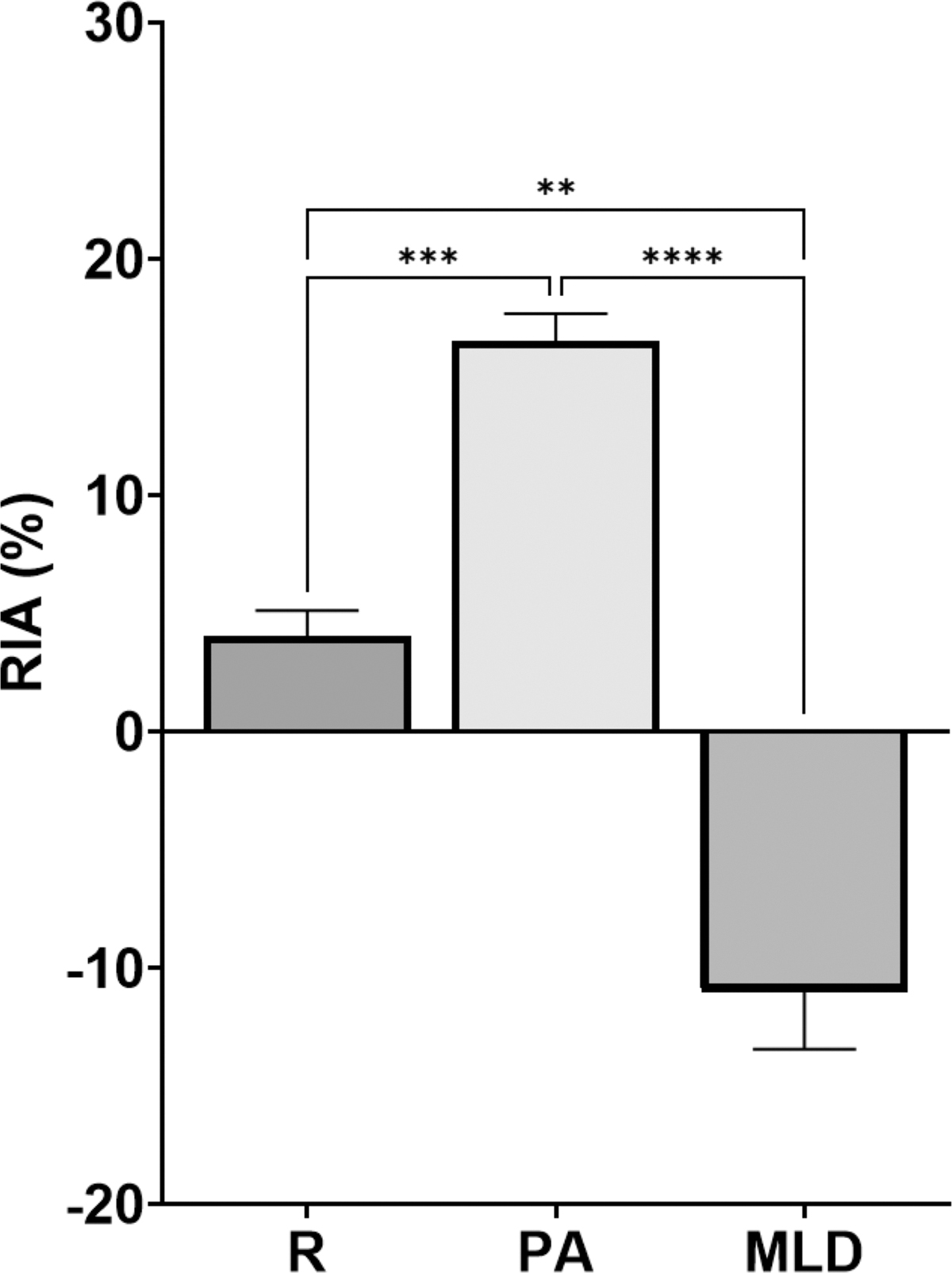
Average quantification in RIA in the areas of dermal backflow during a period of rest (R), a period of PA and a session of MLD. RIA, ratio of increased activity; PA, physical activity. **High statistical significance reached; ***Very high statistical significance reached; ****Highest statistical significance reached.
Second, we can see in Table 2 that there is no significant difference between the two groups during the first phase of MLD or the second phase of MLD. This means that concerning the areas of DBF, the two groups can be compared but also that the LG-MLD and the St-MLD have the same effect with the same intensity.
Average Quantification in the Areas of Dermal Backflow During the First Session of MLD and the Second Session of MLD for the St-MLD Group and LG-MLD Group with Statistical Results Using the Mann–Whitney Test (Between Groups) and Wilcoxon Test (Within Groups)
MLD, manual lymphatic drainage; St-MLD, standardized MLD; LG-MLD, lymphoscintigraphically MLD.
Concerning the filling of the lymphatic nodes, when comparing a 15-minute period of rest for the lymphatic nodes of the healthy upper limb with a 15-minute period of rest for the lymphatic nodes of the edematous upper limb, we can see that their respective effects are significantly different (Mann–Whitney test, p < 0.0001) (Table 3). If a 15-minute period of rest tends to decrease lymphatic node activity on average by ∼10%, it seems that a 15-minute period of MLD increases lymphatic node activity on average by ∼28% (Fig. 3).
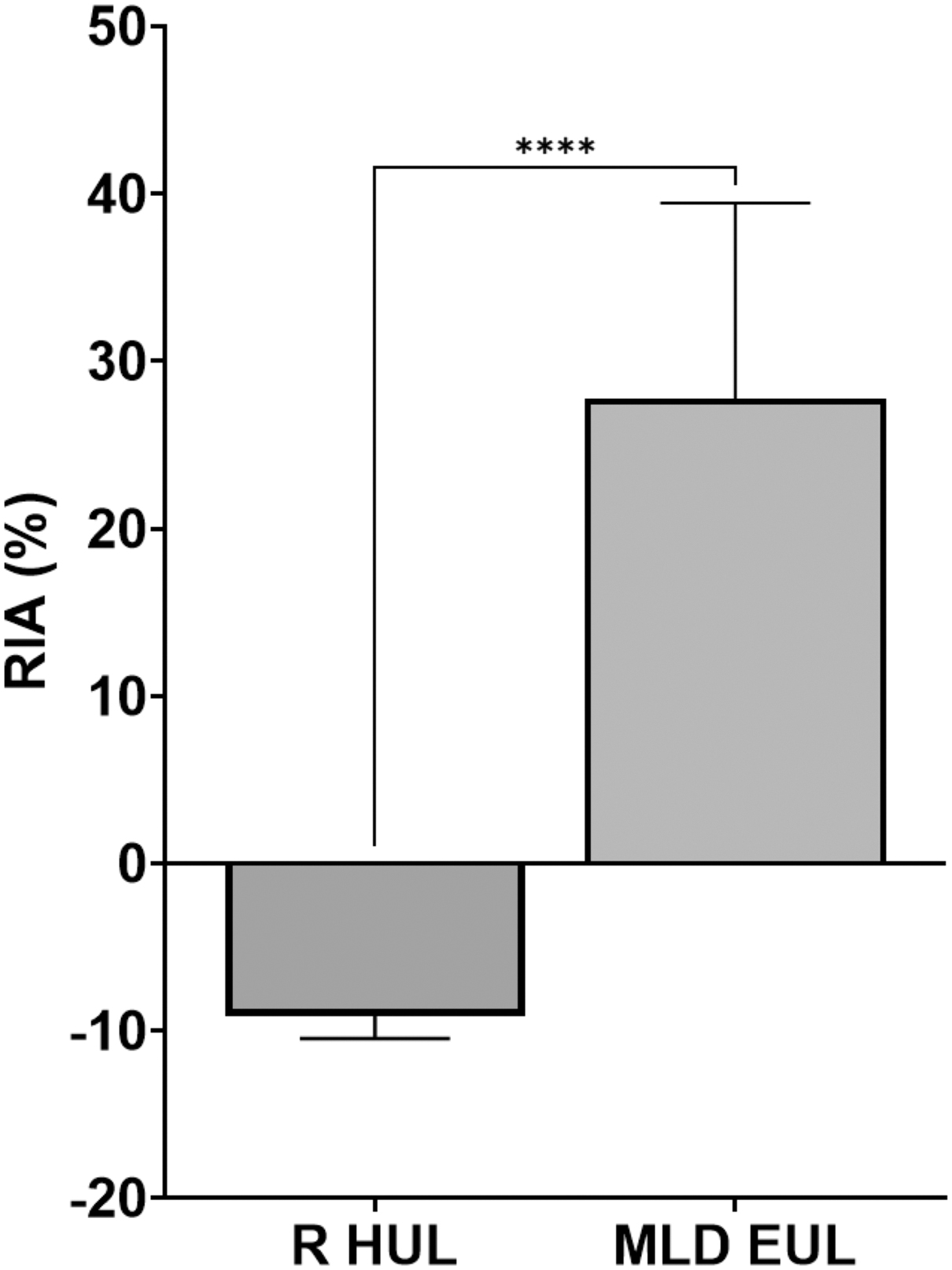
Average quantification in RIA of the lymphatic nodes during a period of rest in the HUL compared with the lymphatic nodes during a session of MLD in the EUL with statistical results. HUL, healthy upper limb; EUL, edematous upper limb. ****Highest statistical significance reached.
Average Quantification in the Lymphatic Nodes During the First Session of MLD and the Second Session of MLD for the St-MLD Group and LG-MLD Group with Statistical Results Using the Mann–Whitney Test (Between Groups) and Wilcoxon Test (Within Groups)
Statistical significance is reached.
High statistical significance is reached.
The results in the ratio of increased activity of the two consecutive phases of MLD for the filling of the lymphatic nodes show that there is no significant difference between the test group and the control group following the first phase of St-MLD. This means that the two populations are statistically similar.
In contrast, there was a significant difference between the two groups for the second phases of MLD, showing that LG-MLD was 19% more efficient than St-MLD for filling the lymphatic nodes. For the control group, a second 15-minute period of St-MLD tends to increase the lymphatic node activity on average by ∼4% compared with ∼21% for the first period of MLD, indicating a significant difference. Concerning the test group, a 15-minute period of LG-MLD tended to increase the lymphatic node activity on average by ∼23% compared with ∼35% for the first period of MLD, indicating no significant difference (Fig. 4).
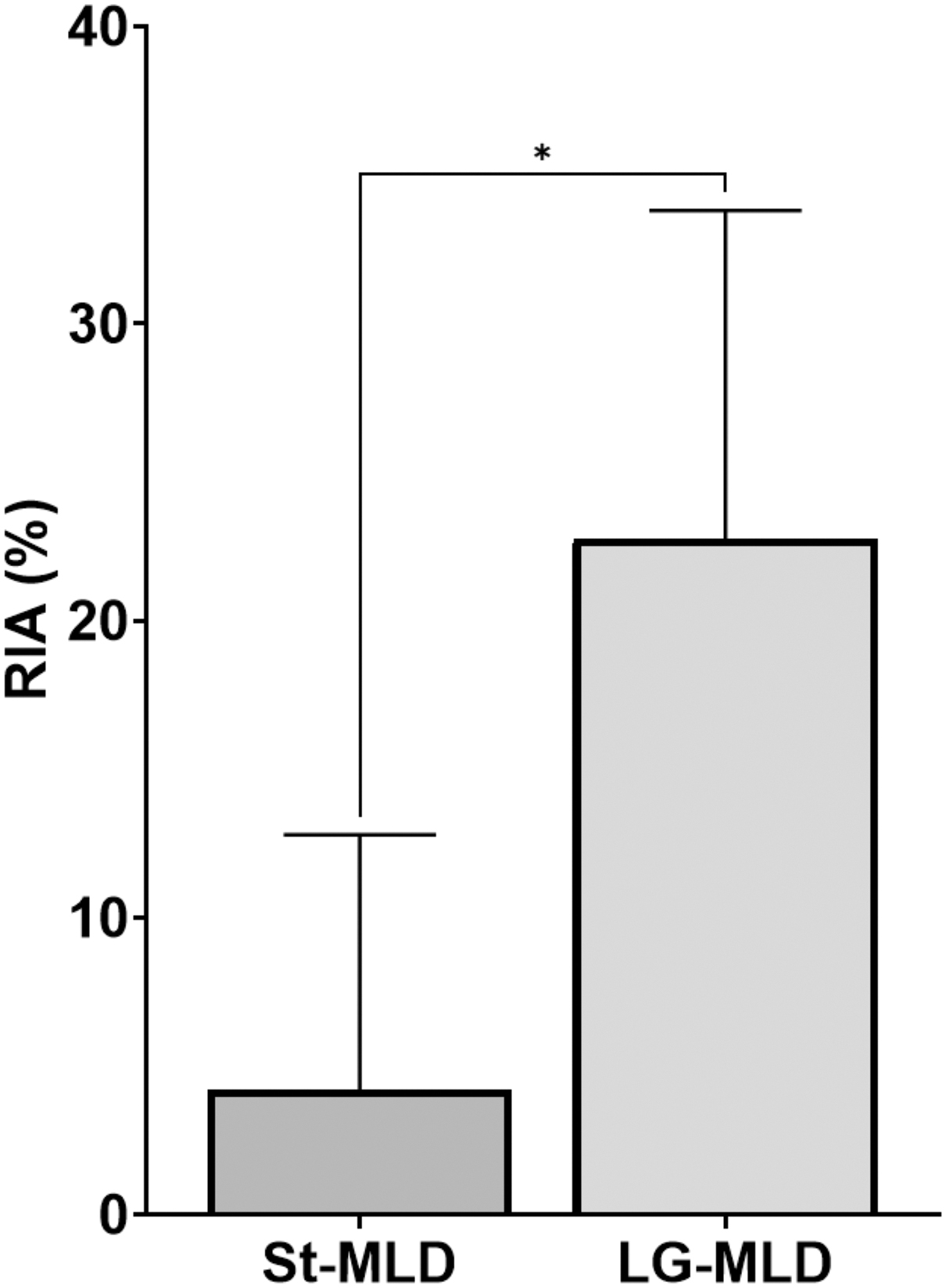
Comparison between the St-MLD and the LG-MLD in RIA of the lymphatic nodes with statistical results. St-MLD, standardized MLD; LG-MLD, lymphoscintigraphically MLD. *Statistical significance reached.
Discussion
MLD is a physical therapy technique vastly described in the scientific literature, and its lymphoscintigraphical assessment has been discussed by several authors.13,21,22 In fact, the literature describes a rather good evaluation of MLD efficiency when assessed by lymphoscintigraphy7,13,22 but also when assessed by near-infrared fluorescence imaging.16,23 Part of the MLD technique was even based on lymphoscintigraphy assessment. Indeed, O. Leduc in 1988 showed that resorption maneuvers were effective in increasing tracer uptake by the lymphatic system and that inciting maneuvers were effective in increasing lymphatic flow. 24 In 1992, De Groot et al. showed that MLD could help normalize lymphatic drainage in 13 patients with lower limb lymphedema. 22 Ferrandez J. C for its part studied the effects of MLD on the lymphoscintigraphical assessment of 47 patients suffering from breast cancer–related upper limb lymphedema. 13 He observed that 53.2% of the patients experienced increased progression of the tracer following MLD. He concluded that MLD was an efficient physical therapy technique regardless of the patient's age, the severity of the edema, its age, or its appearance delay following the surgical intervention. Another study by Sarri Al 7 concluded that MLD stimulated the lymphatic system and efficiently increased lymphatic flow. Our results are also in favor of the MLD by showing that not only is the MLD efficient in increasing the lymphatic flow toward the root of the limb, as Ferrandez and Sarri described, but it can also help to discharge the areas of the DBF. Areas of DBF are commonly seen in patients with lymphedema25,26 and can be defined as a lymph reflux through the avalvular dermal lymphatic system owing to increased intralymphatic pressure itself because of the abnormal lymphatic flow, which will ultimately provoke an extravasated lymph into the interstitial space. 27 This is quite a common phenomenon in cases of lymphedema 26 and is thus an important imaging factor for lymphedema diagnosis. 28 Therefore, it seems logical that one of the priorities for lymphedema management should be to increase the lymphatic flow toward the root of the limb while decreasing the amount of lymph into the dermal lymphatic system to stop extravasation and thus swelling.
Our results suggest not only an increased lymphatic flow following MLD application but also that MLD can decrease the amount of lymph in the areas of DBF. This is in accordance with the case report written by Pereira de Godoy et al. in 2012, where they observed a decrease in dermal reflux following MLD application. 29
This brings us to the second important point of this study, which is to observe whether the lymphoscintigraphy assessment itself can have a role in the therapeutic management of lymphedema. Usually, lymphoscintigraphy is important as the gold standard for the diagnosis of lymphatic function or to evaluate possible treatments.5,30,31 As such, this imaging technique can bring lots of anatomical and physiological information on the patient's lymphatic drainage to the physical therapist. Thus, the physical therapist can choose to adapt the treatment not to the pathology itself but to the patient to obtain greater results. Physical medicine and rehabilitation in general, particularly the approach to pain management, are most effective when they are focused on the whole patient, especially in multidisciplinary approaches in which the specialists of various disciplines are contributing for the patient's sake. 29 This study indicates that lymphedema is no exception because LG-MLD can increase the filling of the LN by 20%, which is more than five times the results obtained in the control group.
However, clinical proof assessing the efficiency of MLD in patients suffering from secondary lymphedema is missing. Indeed, if the MLD is still an important part of lymphedema management, a study in 2016 showed by analyzing >700 studies that although MLD might be efficient, there are not enough clinical results to accept it as a fact. 32 Ezzo et al. in 2015 for the Cochrane Library had the same results that there was a lack of clinical proof to recommend MLD alone as a treatment for lymphedema. 17 However, in their review, they concluded by saying that MLD is safe and well tolerated but mostly that MLD may offer additional benefit when added to intensive compression bandaging for reducing swelling. For us, trying to evaluate the clinical efficiency of MLD alone is not a priority because it is only a part of the physical therapy for lymphedema for which the gold standard is complex decongestive therapy following the principles of the International Society of Lymphology (ISL) 2020 Consensus. 2
In this study, we quantified the MLD technique efficiency through the use of static imaging, but in 2012, de Godoy et al. published a case report showing that combined static and dynamic imaging can be used to quantify the activity gain in axillary lymphatic nodes. 29 We used static imaging because we wanted to individually quantify the MLD efficiency in a larger population. In contrast, dynamic imaging is more effective for showing quantification over time for a certain region of interest in one individual. Although these results are relevant for physical therapy of lymphedema, it only shows short-term functional changes following LG-MLD. Further studies should investigate the improvement following LG-MLD on long-term clinical outcomes like volume reduction and quality of life.
Conclusion
For patients with secondary upper limb lymphedema, MLD can increase the lymphatic flow toward the lymphatic nodes at the root of the limb on average by 28% and can decrease the charge in the areas of DBF on average by 11%. Moreover, if the LG-MLD and St-MLD decrease the charge in the areas of DBF with the same intensity, the LG-MLD increases the lymphatic flow by 19% more than the St-MLD. This means that the patient's lymphatic system imaging can provide valuable information to the physical therapist, which can help improve the treatment by adapting it to the patient's anatomy and physiology.
Footnotes
Acknowledgments
This is a randomized clinical trial that analyzes clinical imaging with respect for patient anonymity and in agreement with the Jules Bordet Institute Ethics Committee (EC 2048). Therefore, no informed consent was needed.
Contribution of Paper
New evidence concerning the efficiency of Manual Lymphatic Drainage (MLD) technique in the management of lymphedema. Gives to the physical therapists reflexion concerning their treatment and the management of their patients with lymphedema by adapting their treatment to the patients pathophysiology. This study is based on a large number of patients that provides precise and steady results.
Authors' Contributions
R.B.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing–Original Draft; S.D.: Formal analysis, Investigation; A.P.: Formal analysis, Investigation; K.E.: Formal analysis, Investigation; M.M.R.: Formal analysis, Writing—Original Draft; O.L.: Writing—Review and Editing, Validation; A.L.: Writing—Review and Editing, Validation; P.B.: Conceptualization, Validation, Writing—Review and Editing, Resources, Methodology, Project administration; S.P.: Project administration, Supervision, Validation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.