
Abstract
Background:
Most existing research in chronic edema (CO) care takes place in high-income countries and is both clinically and medically focused, although often accorded low prestige and status. A myriad of challenges define the problems and important gaps in understanding and translating what we know into sustainable practice. Less considered, however, are the consequences and socioeconomic significance of this “knowledge gap” in an increasingly globalized world. This article seeks to address this lacuna by suggesting a political economy approach across three different income settings, the United Kingdom (high), Kerala in India (middle), and Uganda (low), to learn from international practice and understand the contribution of local (community-specific) health traditions.
Methods and Result:
We used a comparative case study approach. In the three case studies we demonstrate how particular thinking, sets of power relationships, and resource distributions influence and structure the provision of CO management more generally. We demonstrate how these intertwined and often invisible processes reflect a market-led biomedical hierarchization that focuses on high-interventionist, high-cost approaches that are then imposed on lower income settings. At the same time, low-cost but evidence-based local knowledge innovation in wound and CO care from low- or middle-income countries is neither recognized nor valued.
Conclusion:
We conclude that unpacking these dynamics is a necessary route to providing a more equitable health delivery accessible for the many rather than the few.
Introduction
In high-income settings within a globalized economy, the care of wounds and chronic edema (CO) is both highly clinically and medically focused yet often accorded low prestige and status. Dealing with conditions such as chronic wounds that are offensive has been considered dirty work 1 often devolved down. At the same time, there is a small but growing group of patients in high-income countries (HICs) who are suffering from primary lymphedema and who are having both genetic testing and undergoing complex investigations such as magnetic resonance imaging and receive pharmaceutical and surgical interventions at a high cost. This is an emerging area of medical interest that is growing exponentially. In the context of low- and middle-income countries (LMICs), CO is often unrecognized or discussed within the neglected tropical diseases (NTDs) model. Like all diseases, it is shaped by the income distributions that reinforce global health inequities, best understood within the social determinants of health and social capital framework. 2 However, what is often missing in this analysis is an understanding of the wider “determinants of the determinants” of health and how sets of hidden power relationship structure factors across different settings. 3 This gap in health understanding simply serves to maintain the status quo of powerful medical institutions and corporate actors working in HICs.
This article moves to “glocalize” by thinking globally (learning from international practice) while also seeing the potential in local (community-specific) health traditions. It does this by applying a political economy approach to CO across three different income settings: the United Kingdom (high), Kerala in India (middle), and Uganda (low). Political economy (PE) is the social science of resource distribution (i.e., consideration given to who gets what, why, when, and how), and offers a useful entry point for engaging in substantive debates regarding sustainable practice unhampered by contemporary medicalized prejudices where there is a perception that there is little that can be done. At an epistemological level, PE gives fresh significance to the historical context in interpreting health care thinking. The case studies we use allow tentative correlations between low-cost, local healers, and high-cost (biomedical) treatments within variable geographical locations, each with different resource limitations and understandings about CO.
The PE of health
It has been argued that the political nature of health is public health's “biggest idea.” 3 When Rudolf Virchow wrote, “medicine is a social science, and politics nothing but medicine at a larger scale” 4 he was recognizing, as Fredrich Engels had in Conditions of the Working Classes (1848) 5 3 years earlier, that the material and structural conditions under which we work produce, and reproduce, health inequalities. A credible critique, but the real nub of such thinking is more nuanced: “health,” “medicine,” “politics,” and “economics” cannot be understood separately because medicine, health, and economy knowledge is already political in its origins and consequences. Here knowledge is both a form of power and wealth. As such it has different distributions: access enriches, exclusion impoverishes. How should we then proceed to think in the first instance? Whose health care knowledge have we come to rely upon and why? A PE methodology usefully speaks truth to power and wealth in both its constitutive and practical manifestations.
The analysis of PE has an ancient pedigree. Aristotle's word for “politics” was politike (short for politike episteme or “political science”) and was the most authoritative of all sciences concerned with the production of human well-being. Oikonomos, conversely, was the science that considered how public organizations could best serve the “body politic.” Here economics was always the regulated servant in service to “healthy” politics. The contemporary view that politics and economics are distinct areas of activity would be considered deeply counterintuitive. Put another way, the very idea that the spheres of “politics,” “economics,” and “health” are to be approached separately is post-Enlightenment and traceable to the birth of a modern hegemonic political system: capitalism. It must be understood, however, that we are describing not simply the globalization of “barter and exchange,” but rather a mode of economic organization that is completely novel through its radical separation of producers from the means of production and insatiable demand for profitability.
In the five centuries since its inception, capitalism has transformed the terms of health care knowledge. A powerful symbiotic relationship has developed between medicine, modernity, and the dynamics of capitalist growth. On one hand, the rise of capitalism is best understood as the key constituent in the triumph of Western models of (scientistic) thinking. Western health care has thereby become the standard-bearer of modern (rationalist, capitalist) civilization. Like liberal democracy, modern health care demonstrates the universal superiority of an all-knowing Western mind and we can travel untrammeled lines from the Hippocrates 5th BCE oath to the use of artificial intelligence in today's high-technology operation theatres. On the other hand, despite rhetoric to the contrary, Western health care thinking is usually imperialistic. Even within the confines of Western societies, health care has normally been elitist, and a tool wielded by white, rich, powerful males. We see this in the contributions of philanthropists such as Chamberlain, Rowntree, and Chadwick in the 19th century through to Gates, Bezos, and Zuckerberg today. It is this reality that largely determines our health care knowledge and what is included or excluded from the discussion.
Here the question of trust becomes center stage in shaping practice. Different forms of health care have acquired variable trust statuses, with the most obvious being the split between high-cost (“high value”) medicalized knowledge and low-cost (“low value”) local health traditions. Epistemological and methodological privileging has meant that community-specific voices have become part of a delegitimized, peripheral (premodern, crude) nexus in opposition to a legitimate, core (modern, sophisticated) world view. Race, racism, and gender are deeply embedded in this hierarchization.
A PE methodology demonstrates there are at least two potential consequences of the intimate relationship between capitalism and the production of health care knowledge. First, modern (read: Western) biomedical health care thinking has displaced traditional healing and dismissed local practices as irregular. This is not to say Western science cannot be relied on, but to question whether we simply accept it as the sole agency with which to make all decisions about health. There are other voices to consider. Second, we are witness to the reinforcing of a modern approach to health care that has taken Western models of thinking regarding “profitability” as its implicit norm. Here politics has become the servant to and agent of economics. And this is not a healthy turn of events.
We now present three case studies to demonstrate how these themes of privilege, wealth, and resource distribution play out with CO in both theory and practice across different income settings.
Case Study 1: Uganda
Inequality in Uganda is on the increase with a rise in the country's Gini coefficient from 38.5% in 2013 to 42.8% today.6,7 The level of inequality within the country varies with populations living in rural settings experiencing the highest vulnerability. 7 CO is observed in lymphatic filariasis (LF), a condition with a prevalence of 0.4%–30.7% among school children. 8 Transmission is largely by Wuchereria bancrofti, which is transmitted by the Aedes aegypti mosquito. CO is also observed in a condition called podoconiosis (podo) at a prevalence of 4.5%. 8 This is nonfilarial elephantiasis unique to areas with volcanic soils. Although its pathogenesis is not well understood, it is associated with continuous contact with irritant minerals. The risk of contracting LF and podo thus results from geographical, environmental, genetic, socioeconomic, and cultural factors. 9
There is a vector control division within the national level of the Ugandan health system (Fig. 1) that categorizes NTDs into preventive chemotherapy (PC-NTDs), LF inclusive and those controlled through case management (CM-NTDs) such as podo. As in general health care, NTDs service delivery is broadly cut across public and private sectors. Within the public sector, health care providers such as clinicians, nurses, and community health workers, locally known as village health teams (VHTs), provide services in hospitals, health centers, and villages (Fig. 1). The role of private actors, including those working in the profit and not-for-profit organizations, is gaining prominence. 10 NTDs service delivery is also supported by international agencies and donors. A recent study indicated that in Uganda, 70% of health financing is from donor funding. 11 Another category of actors in NTDs, although not part of formal health care delivery, are family members. These provide basic LF and podo care, particularly where access to formal health care is limited.
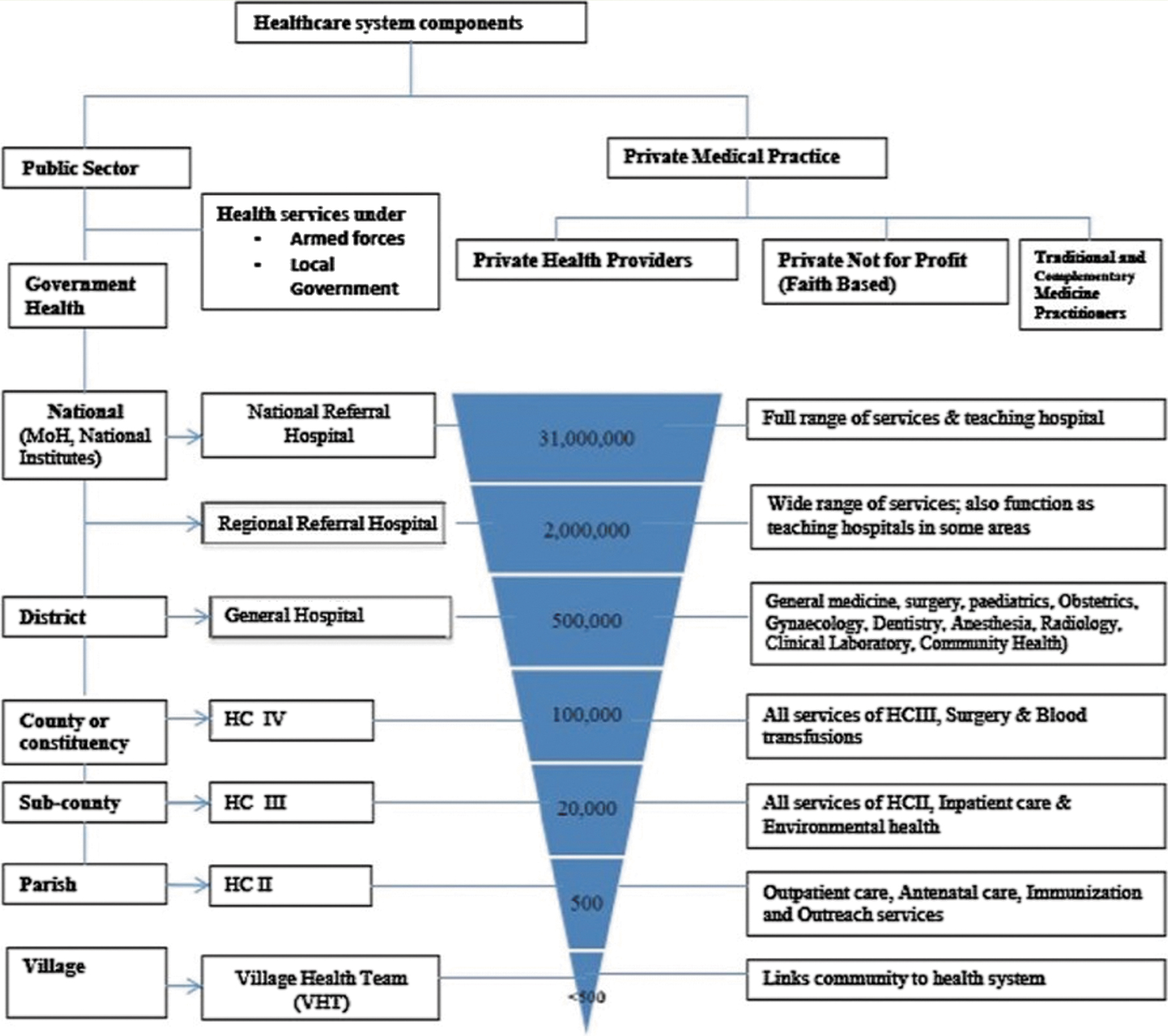
The health system structure in Uganda (Acup et al. 12 ). Color images are available online.
Traditional healers, or community-specific health care, utilize local medicines and natural therapeutics.12,13 They constitute key private actors although their contribution to the health care system, specifically NTDs control, is not fully understood. 13 It is estimated that up to 79% of the total Ugandan population utilize indigenous traditional practitioners, while between 1% and 19% utilize complementary services such as acupuncture and osteopathy. 14 Studies 15 on health care utilization reveal that patients perceive traditional healers in Uganda to be more caring, and engagement here is mostly based on peer referral. On the contrary, biomedical health care patient/provider relationships were characterized by neglect and abuse (ibid). These authors also state that the utilization of modern health care technology was sometimes intentionally avoided because of invasive procedures such as limp amputation. 15 The National NTDs control programmes have attracted free drugs worth millions of dollars to interrupt the cycle of infection. Community distribution targets adults through trained VHTs who distribute albendazole and ivermectin drugs door to door, and through mass community distribution of donor-donated mosquito nets. As required by the Global Programme for Elimination of Lymphatic Filariasis (GPELF), 16 mass drug administration (MDA) programmes are also carried out through dedicated lay health workers operating in endemic NTDs communities. 17
There are few documented traditional approaches to the treatment of podo in Uganda. Tekola, Damen, and Gail 18 recommend that wearing protective footwear such as closed leather shoes early on in life in endemic zones prevents contact with the irritant soil. Based on their study in southwestern Uganda, Dwek et al. 19 argue that poverty hinders the purchase of appropriate footwear. They also recommend improved awareness of the diseases among health care practitioners to increase early detection. Primary prevention and home-based treatment include daily foot washing with soap and water, as well as the use of compresses or bandages (Fig. 2). Experts recommend that patients soak their legs in antiseptic water and massage with oil-based emollients such as Vaseline together with wound care including bandaging and socks.
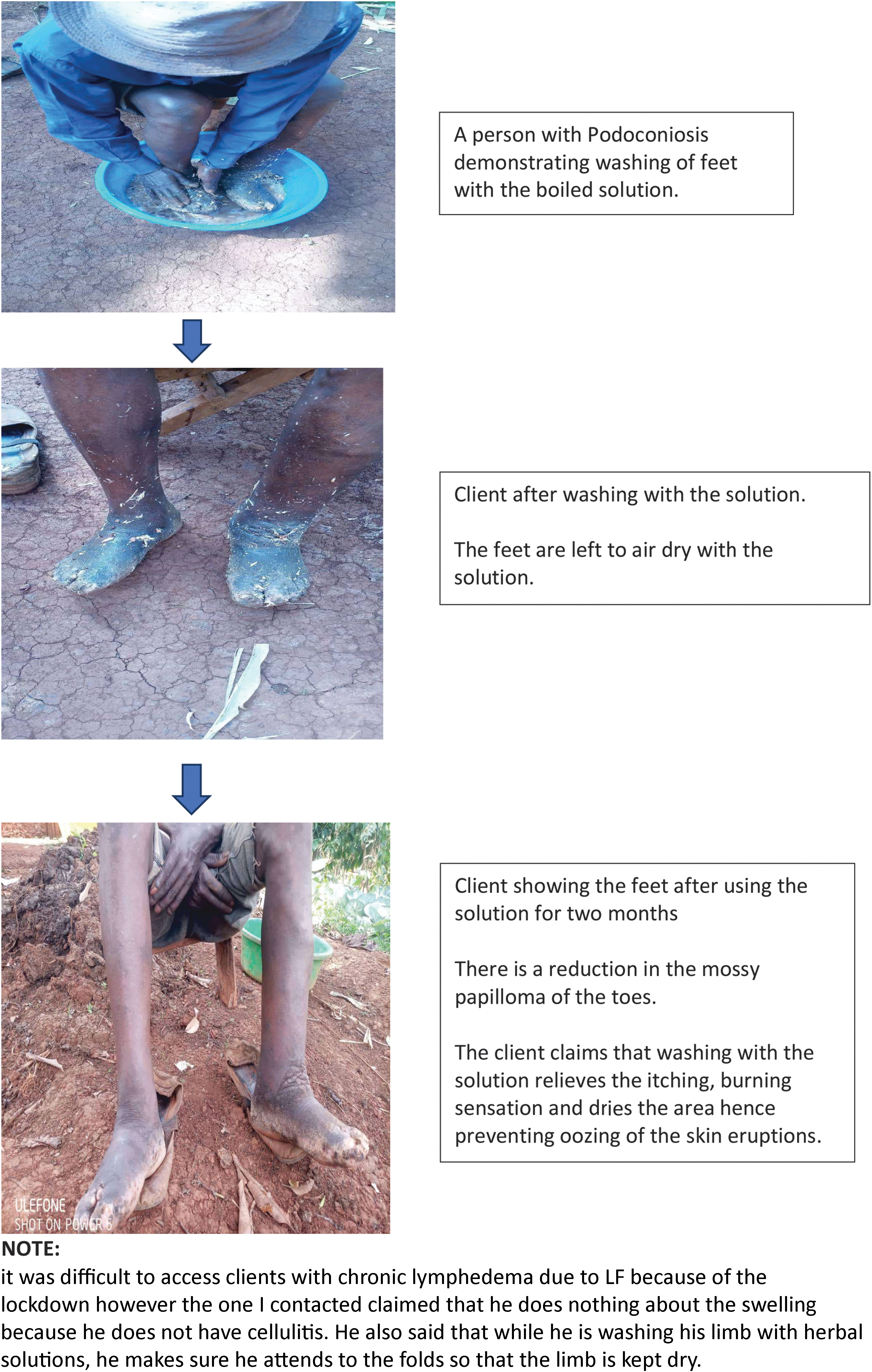
Home care/alternative management for podo. Photograph credit: Lydia Kabiri (Uganda). Podo, podoconiosis. Color images are available online.
Health facilities are supplied with ivermectin and albendazole for prevention chemotherapy and other drugs such as doxycycline to manage acute LF. The infected wounds are cleaned with saline water and hydrogen peroxide 6%. A topical antibiotic ointment is applied after cleaning the wound. Sometimes an intramuscular antibiotic injection is given to manage secondary infection often defined as acute inflammatory episodes. CO patients often prefer receiving health care from privately owned clinics than from government facilities as they are more trusted and accessible. Those who go to the clinics are taught about home wound care and discharged with supplies such as hydrogen peroxide 6% and antibiotics. Heavy emphasis on home care reflects the country's reliance on health promotion. In the 2019/2020 financial year, local governments contributed 20% of their primary health care budgets to health promotion. 14 Health promotion started in the 1940s and has evolved to include relevant hygiene practices such as “Bulungi bwa nsi” where communities meet and clean wells and roads, 20 but the implementation of community activities is donor dependent and leads to inconsistencies in providing preventive chemotherapy such as ivermectin, which is supposed to be given in combination with albendazole. The lack of knowledge among health care workers in the diagnosis and management of LF has affected surveillance of the condition hitting drug procurement and availability. Poor health literacy about CO in terms of the health system and health delivery also leads to poor health-seeking behaviors.
Case Study 2: Kerala, India
Low-cost, high-quality, and overall scalable public health is vital particularly in a huge country with a Gini index 35.7 (0.35) in 2021. Health governance in India is complex (Fig. 3). Public health services are executed mainly by state governments and the Kerala State is a model for hierarchy-based decision and execution (https://dhs.kerala.gov.in/wp-content/uploads/2021/02/chart.pdf). The private health sector dominates curative treatment services. Health services available include Western biomedicine, Ayurveda Yoga, Unani, Siddha, and Homeopathy (AYUSH), and traditional family practices of treating common illnesses by experience gained through generations (traditional healers). The National Health Policy 21 emphasized integrative medicine for chronic noncommunicable diseases. However, all services are compartmentalized. One blanket protocol does not work in India. For example, the maternal mortality rate in Kerala is 12 against the Indian average of 42 and women's literacy (93%) against the national average of 65%. 22
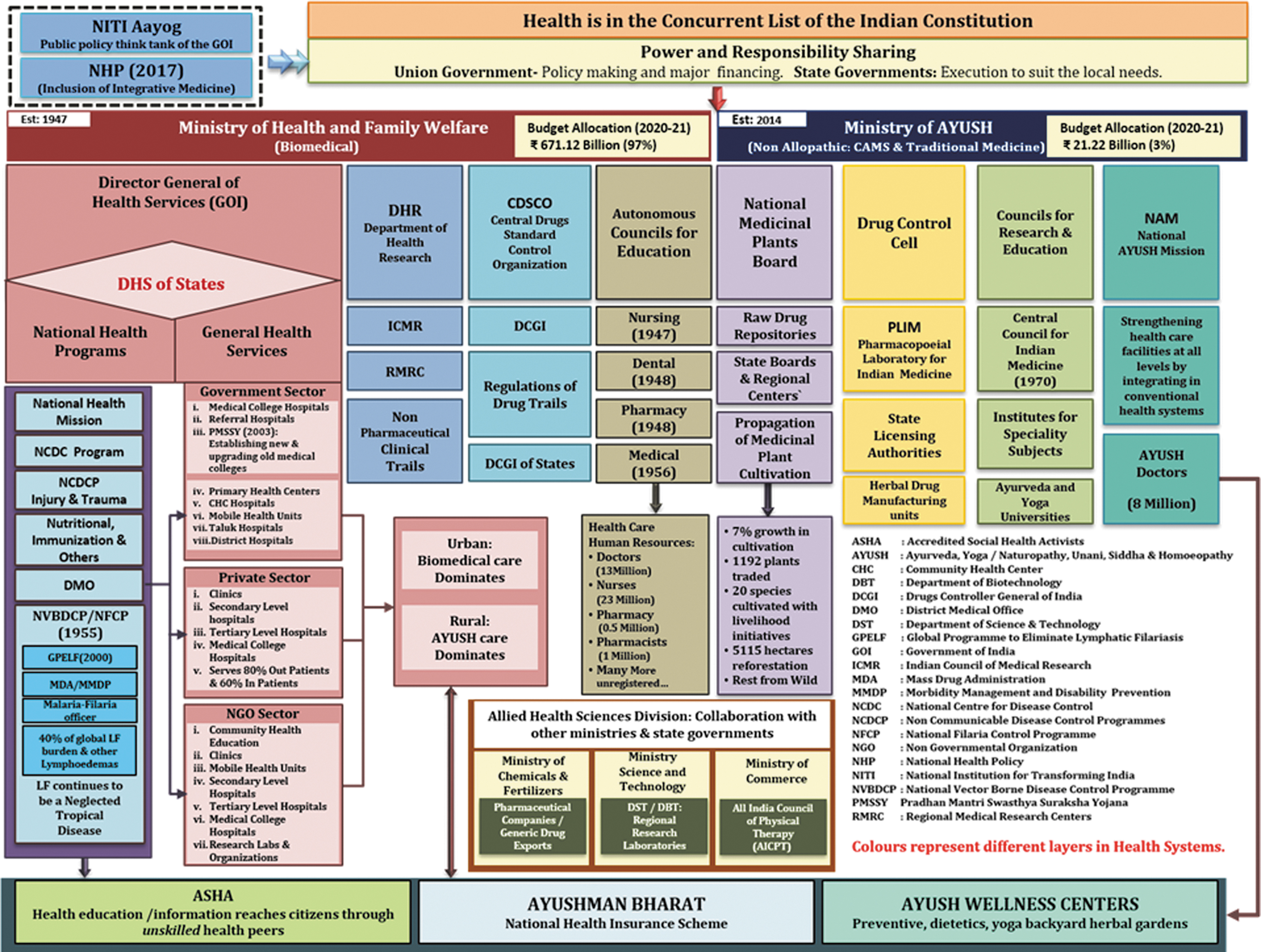
Medical diversity within the complex Indian health systems (population: 1.4 billion). Color images are available online.
Lymphedema caused by LF is recognized as a major public health problem since 1955 through the National Filaria Control Programme (NFCP). 23 The lower leg lymphedema and hydrocele are the stigmatic clinical diseases caused by LF. Forty percent of global LF patients live in India with 460 million population at risk of infection. Since the launch of the GPELF in 2000, the government has periodically shifted the goalposts to eliminate LF. NFCP is one among tens of national health care or eradication programmes. This suggests the low priority given in fund allocation even if LF gets a higher priority in terms of policy and articles. LF continues to be an NTD of the poor.
Biomedical doctors commonly prescribe compression therapy for lymphedema. All hospitals provide services for routine surgical dressings to all types of leg ulcers. A few medical colleges, plastic surgery departments, individual surgical clinics, expensive corporate hospitals, and physiotherapists are beginning to take the initiative in surgical treatments and European complex decongestive therapies. However, surgeons continue to use conventional combined physiotherapy before and after surgery.
Ayurveda is a widely used system among AYUSH (Fig. 4). It serves mainly as the primary care in villages. Ayurveda is written in Sanskrit. Its origin is traced to 300–200 BC 24 and has been treating lymphedema (known as Sleepada; slee =elephant paada = leg) since that time. Integrative medicine for LF (IML) is the therapeutic integration of biomedicine with Ayurveda and Yoga (Fig. 5). Studies have shown that IML has the potential to fit both an academic medical center and a remote Indian village. Each treatment component of IML is cheap, easily provided after brief training, culturally sensitive, and capable of widespread compliance. The Institute of Applied Dermatology (IAD) is a dedicated center for IML. 25
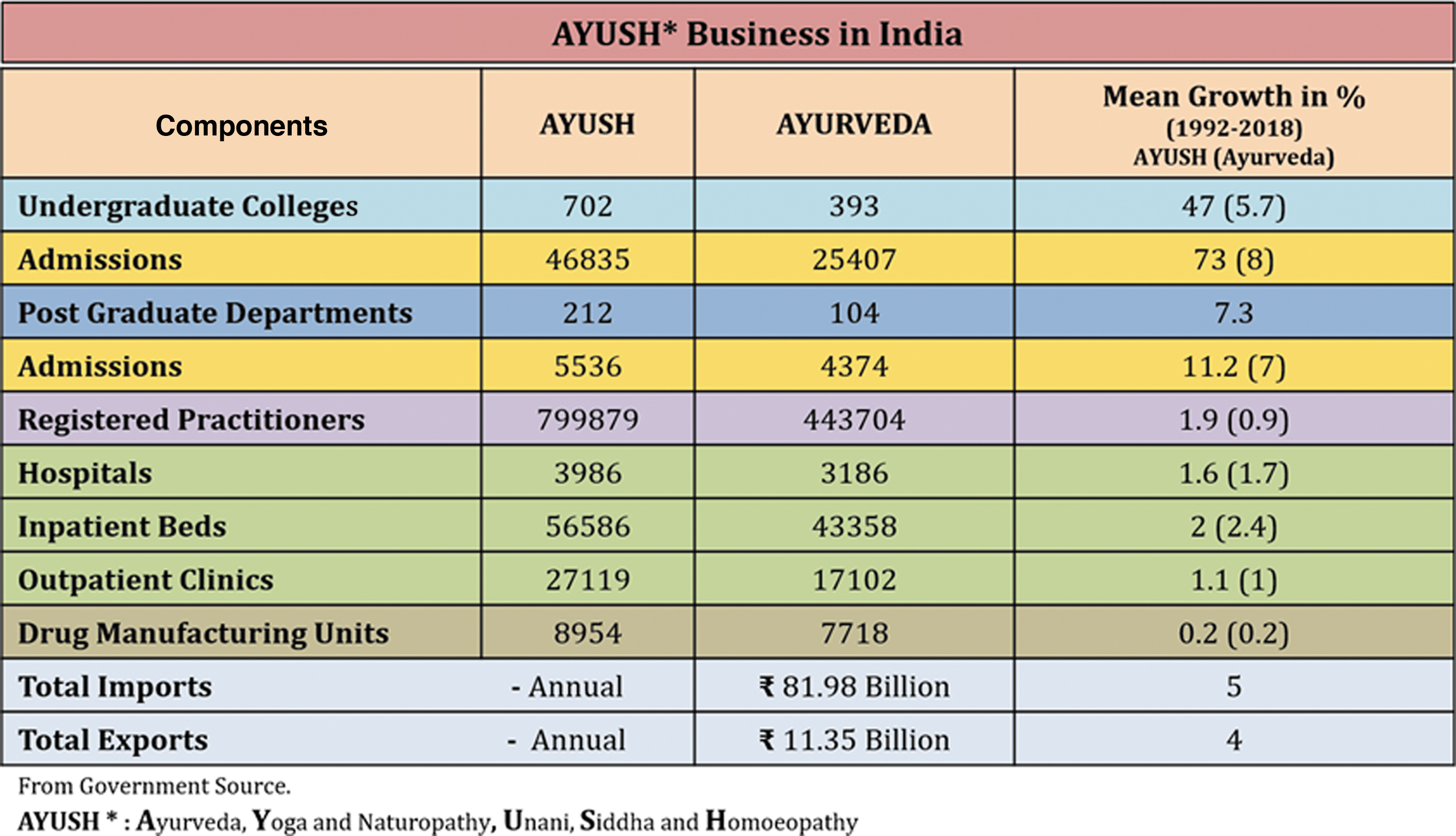
Ayurveda, Yoga, and Naturopathy, Unani, Siddha, and Homoeopathy. Color images are available online.
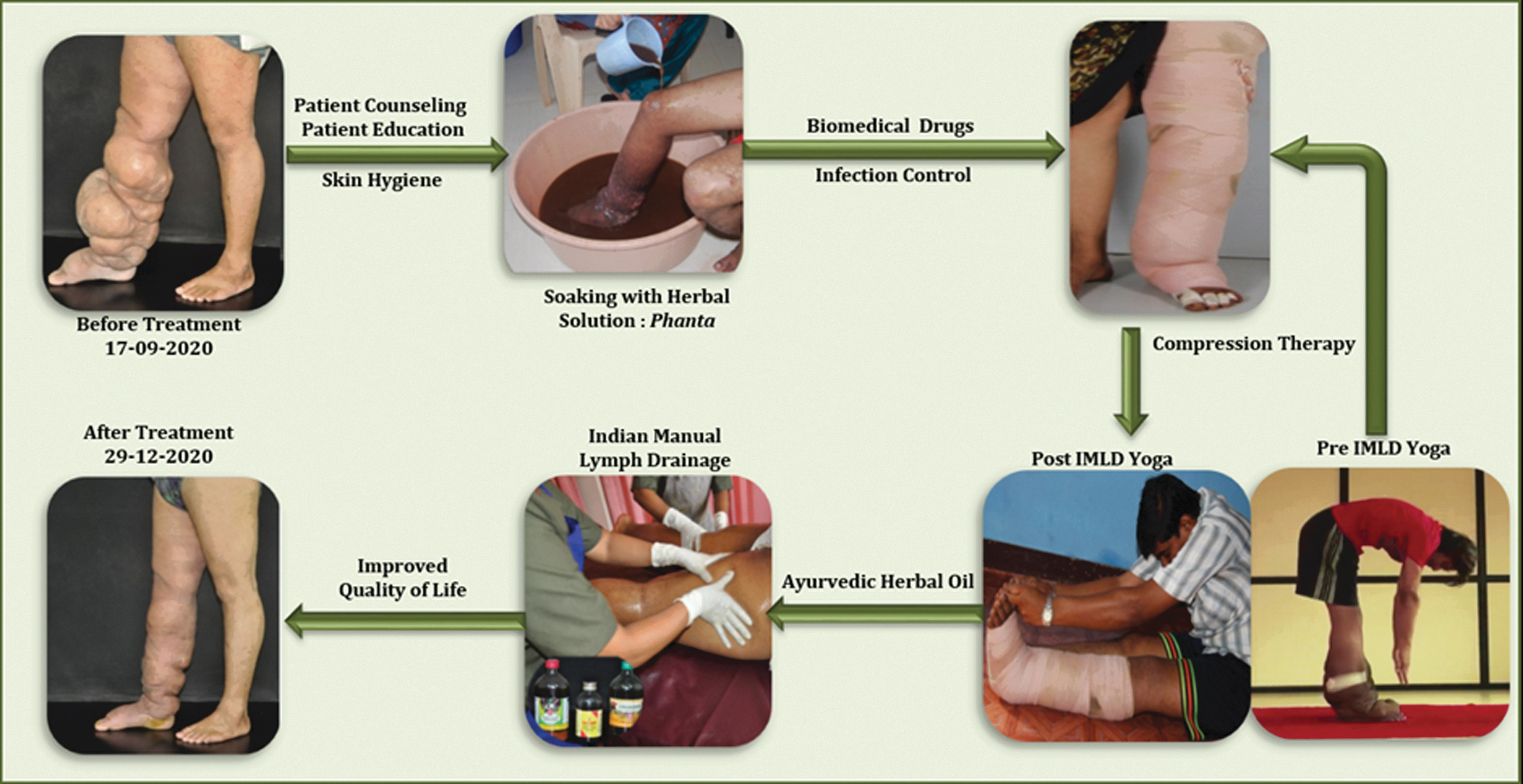
Integrative medicine treatment for LF at the IAD: simultaneous use of biomedicine, Yoga, and Ayurveda provides significant outcomes in lower leg lymphedema. IAD, Institute of Applied Dermatology; LF, lymphatic filariasis. Color images are available online.
Compression therapy at the IAD is done using long (elastic) stretch compression bandages. During the last 5 years, new compression devices and high-technology bandages are available in the market. However, they are expensive for LF patients. It is challenging to locate a competitive supplier for quality bandages. There are concerns about batch variations in the stretchability and durability of these bandages and the standards and testing regulations. The Textile Association (India) and Textile Research Associations of the Union Government encourage the industry to export, including compression bandage materials, as an important source of foreign currency revenue. Compression bandages consume 72% cost of medicines and materials for a patient with a unilateral lymphedema leg of 7–18 L volume. IAD also spends 49.3% of the total personnel expenditure on the lymphedema caregiver and support team as IML is a labor-intensive regimen for patients.
GPELF is encouraging LF endemic countries to roll out morbidity management and disability prevention (MMDP) with LF spread widely in the subcontinent of India. However, there are many other causes of lymphedema. The MMDP rollout is likely to face formidable challenges over and above the corruption that exists in the government and society at large. However, global accomplishment requires India, with over a third of the disease burden, to execute MMDP successfully. IML could be a standard uniform intervention in the densely populated, culturally diverse, resource-limited Indian settings. As a complementary and alternative medicine system, Ayurveda teaching allows local modifications and individualized treatment. IML is low cost, locally available, and culturally acceptable. Counseling as part of IML is repeatedly given to help individual patients come out of personal vulnerability and to live in dignity when possible with economic viability. Because it involves Ayurveda and Yoga, IML is not high on technology, and field trials have shown that locally recruited teams can easily be trained.
Case Study 3: the United Kingdom
The UK wealth distribution is roughly the average of all Organisation for Economic Co-operation and Development (OECD) countries (73.2%), but compared with other developed countries, the United Kingdom has a very unequal distribution of income with a Gini index of 34.8 (0.35) in 2021, making it one of the most unequal of all European countries. The UK National Health Service (NHS) is publicly funded and was established in 1948 to provide free care at the point of delivery. All UK residents have access to a general practitioner and hospital care funded through tax and national insurance. The UK government devolves responsibility for care to the Scottish and Welsh Governments and Northern Irish Assembly. There is no overall health policy for lymphedema in the United Kingdom, however, Wales has a national strategy. The UK National Wound Care Strategy (NWCS) tangentially refers to CO in relation to leg ulceration. 26 NICE guidance for lymphedema is limited to breast cancer and liposuction. 27
The UK has led the way in defining the epidemiology of CO with recent studies predicting around half a million cases, however, this is likely to be a significant underestimate due to poor professional knowledge.28–31 A recent study showed that almost 57% of patients who are treated in their own homes by community nurses suffer from CO. 32 It is also common in European hospitals with 38% of hospital inpatients affected. Patients are also found in social care settings such as nursing homes although the data are limited. Risk factors for developing CO include venous disease, cellulitis, cancer, increased age, obesity, reduced mobility, diabetes mellitus, and heart failure. 32
Lymphedema care in the United Kingdom is exclusively biomedical. Historically, services were based in cancer services due to the belief that it was predominately a complication of cancer treatment with other patient groups denied access. The pattern is changing, but access to specialist services is still based on a “postcode lottery” with many areas lacking care provision. Professional knowledge remains poor and a lack of clarity over who requires specialist intervention leads to unnecessary complications such as cellulitis, which frequently requires hospital admission with a lifetime risk of 37.4%. 33 The UK has an active patient support group The Lymphoedema Support Network (LSN), who with the British Lymphology Society (BLS) representing health care professionals is the main advocate for improved care.
A major factor influencing a coordinated approach to care in the United Kingdom is the heterogeneity of the patient population. No single medical discipline takes ownership of the problem and services are largely developed around clinics that are interested in the area and include palliative, wound care, dermatology, and vascular services. There are interdisciplinary services for complex patients in parts of the United Kingdom. The national center at St George's Hospital, London, includes a genetic screening programme with a second site in the East Midlands. The models of care elsewhere in the country are highly varied and include a mixture of public and private clinics, many of which are run by lymphoedema therapists (predominantly nurses and physiotherapists).
Models of care are paternalistic with an emphasis on a period of intensive daily treatment (skincare, manual lymphatic drainage [MLD], exercise, compression bandaging) in outpatients or primary care. Daily self-management is recommended although clear guidance is lacking despite it being labor intensive and quite a burden on the patient and family.2,34 Availability of MLD is sporadic with some patients having to pay privately. This is due to the limited evidence of its clinical and cost-effectiveness, except in the early stages of the disease. While most treatment is aimed at the prevention of secondary complications, some attempts are now being made to address primary prevention. This is limited to surveillance and early introduction of compression in cancer populations such as breast cancer. Lack of access to products for treating lymphoedema, except in hospitals, led the UK National drug tariff in 2006 to include a new category. As a result, there has been a rapid expansion in the range of products available and investment by the medical device industry. While this has dramatically widened the access to products, professional knowledge and service redesign have not kept pace with these changes.
Many of the current wound care products such as honey dressings, have their origins in traditional medicine, which have been adopted and developed by the medical device industry.35,36 One of the oldest treatments is recorded on a clay tablet in 2200BC and refers to the use of clay, plants, and herbs and describes washing, plasters, and bandaging. Bandages have been described in Roman, Indian, Egyptian, and Chinese cultures. 37 There has been a long awareness of the importance of protection and management of exudate with the use of oil in many cultures. During different centuries, lay beliefs significantly influenced the use of materials. During the Middle Ages, wounds were viewed with fear and were seen to be a release of “evil humours.” 38 The concept of “laudable pus” 39 was seen to be an integral part of the patient journey in which many succumbed to overwhelming sepsis, with a minority recovering. While the UK may be considered a high-resource country and boast a comprehensive and available health system, provision of care for people with lymphoedema is patchy and inconsistent. There is a lack of policy to support sustainable change, which is aggravated by the complexity and lack of a clear definition of who pays for care and is responsible.
Discussion
Knowledge gaps and knowledge production
CO looks very different in different parts of the world, but there are two recurring and interrelated themes emanating from our case studies that suggest unity rather than division: first, the knowledge gap in CO translates into poor health literacy in terms of health providers, systems, and delivery, but within this space, it is clear we see the hegemony of biomedicine (i.e., medical establishments in different income settings tend to structure the “known and unknowns” of CO care in remarkably similar ways); second, and by no means unrelated, lack of interest, governance, and control leads to an increasing reliance on market-led and market-based solutions to questions of CO. Once again we ask: whose knowledge do we rely on and why?
The initial point to be reminded of when discussing CO care is always the contested nature of definitions. Across the case studies, we can see the globalizing force of biomedicine in the treatment of CO and NTDs. A key feature of a globalized biomedical approach is that there is no alternative discourse offered to that of clinical treatment and self-management rather than prevention. There has, to date, been very little analysis of the social determinants of health “upstream” (except for Nairn, 2019) approach in that framing discussion. For example, in India and Uganda, it is tropical LF that captures attention in the academic and clinical literature,1,40 but in the United Kingdom, the condition is more associated with cancer treatment, injury, inflammation, or lack of movement (inactivity). However, little is known on the proportion of those who suffer from other forms of lymphedema seen in high-resource countries, for example, secondary to cancer. It is likely that these types of patients do exist in these countries but are described as having LF. Lack of access to facts widens knowledge gaps.
In India and Uganda, LF is a disease of the poor. Uganda has the added burden of podo care. Podo is also a disease of the poor and often a disease of the poorest of the poor together with being one of the most neglected of all neglected diseases. In all examples, a complex combination of employment patterns, socioeconomic, geographical, cultural, lifestyle, and (sometimes) genetic factors plays out. The risk of contracting podo, for example, is highest in those who work with or in the proximity of volcanic soil—farmers, potters, miners, weavers, and so on. In the UK, we know that nearly half of all cancers are caused by four lifestyle factors—smoking, unhealthy diets, alcohol, and obesity (www.cancerresearchuk.org/). Although LF generates academic interest, it is still a low priority clinically. This means a knowledge gap exists both in terms of the construction of knowledge about the condition and as a consequence of what should be understood as an appropriate and successful intervention.
A problem with definition exists particularly where it leads to a lack of clarity regarding who, what, or which actor should properly own the issue. Should states or markets lead? Is care primarily a question for hospitals, community carers, or informed homecare? Is it of international, national, or simply individual concern? Education is key. We also know that the condition is highly stigmatized, and consequently, hidden meaning and access to facts is difficult. All three case studies suggest something sociologists might call a “Moral Panic” and “Folk Devil” scenario. 41 This trait is keenly exhibited in Uganda where sufferers are believed to be cursed and find themselves excluded from social gatherings, places of worship, and even private spaces by their own family and friends. Breaking these social barriers requires education. However, education is more challenging in socially deprived conditions where illiteracy is rife and few people can read or write. Misinformation and “fake news” encourage fear and irrationalism.
Governance and Control
Currently, filariasis and podoconiosis are treated as NTDs, while in the UK, the need for lymphedema services is neglected. Many LMIC governments such as Uganda and India have increasingly come to rely on donor funding to provide access to drugs and technologies as they are unable to afford the products themselves. 42 MDA as we saw being used in the Uganda and Kerala case studies is offered by an increasingly concentrated medical technology industry as the solution to addressing targeted diseases such as filariasis and other NTDs. Globally, treatment and care for people with lymphedema take place in many settings from self-management in the family and community (ILF; World Alliance) and clinical hospital-based services, although accurate data on prevalence are again problematic. 43 However, treatment options tend to focus on medical interventions rather than preventative programmes.
In many HICs, it has increasingly become recognized as a clinical nursing specialty across wound care and tissue viability with an attendant multimillion-dollar industry in specialized dressings and treatments. The “advanced product segment,” which covers wound dressings for the treatment of chronic and nonhealing wounds, for example, accounts for the biggest revenue growth of over 34% in 2020. 44 These very specialized dressings often contain antimicrobial agents drawn from traditional remedies of honey and silver with randomized-controlled trials used to extract the active ingredient for use in products.
In 2020, the global wound care market size was estimated at USD 19.83 billion and is expected to reach USD 20.59 billion in 2021, 44 with 13 companies adopting strategies, such as mergers and acquisitions and partnerships, to strengthen their market position to accelerate the development of advanced wound management product portfolios. These initiatives are anticipated to expand their customer base. The domination of the global market in health care and the powerful advance of large transnational corporations emerged with the rise of the neoliberal era in the development sector represented by structural adjustment programmes imposed on LMICs such as Uganda and India by the World Bank and the IMF (International Monetary Fund) in the 1980s onward.
In India, we noted that the 2017 attempt to integrate treatment for chronic noncommunicable diseases via a National Health Policy has not worked to integrate a workable approach to LF prevention and treatment. Services remain compartmentalized. International agencies (such as GPELF) encourage MMDP, but the rollout is often challenging due to mismanagement and corruption. The pharmaceutical and medical technology industries have championed the “magic bullet” approach of providing new drugs or medical devices/technologies and in strong alliance with biomedicine present as the only solution. As a consequence, health care costs become inflated and, combined with the patenting system, this leads to a divide in access to their products globally due to price. There are many, many examples to choose from, but lack of access to antiretroviral drugs in Africa during the height of the HIV pandemic 45 and, more recently, lack of access to vaccines globally in the COVID19 pandemic 46 demonstrate that despite increasing recognition of the problem and calls for bridging the gap of inequalities, global disparities remain. Unequal access to medicine and its technologies due to “for-profit” companies seeking to protect their margins and market share remains despite strong critique of the sector. 47
At the same time, the solutions offered by the medical technology companies are accompanied by the rhetoric of working with communities, providing health education and local ownership. Problems of weak local infrastructure and issues in distribution chains lead to a return to vertical, externally audited, biomedical interventions as Allotey et al.'s study demonstrated. 48 A critical reading of the interface of global health technologies, expertise, and programmes led by donors with local community-based initiatives demonstrate that they merely deflect responsibility away from the need to invest in strengthening public health systems. MDAs and cross-subsidizing of products for developing countries, as we saw in the Uganda case study, are presented as a “healing the suffering of the poor” narrative by large transnational companies, and plays into the heroic nature of (Western) scientific advances, reinforcing development narratives around “aid.” This then has the effect of creating dependency markets for the medical technology industries.
In the treatment of wound care and lymphedema, the prescription and investment in clinical care have led to the emergence of a huge transnational market in medical products for wound care as illustrated above. Lymphedema is positioned in LMICs as an NTD, yet a social determinants of health analysis of NTDs reveals wider structural inequalities that intersect with their incidence: for example, poverty; access to water and sanitation; housing; gender; social exclusion/displacement; and migration to name a few. 49
The dominance of the biomedical approach in research funding also means there is little discussion of the social causes of the disease or the preventative approach to reducing incidence. The focus is on changing individual behavior and ensuring treatment compliance rather than tackling the systemic causes of ill health and investing in health within and across systems and structures as advocated by global health promotion agencies. The poor have little agency and are disproportionately disadvantaged within the largely invisible social and political structures. Farmer 50 argues that this is a form of structural violence exerted against the poor. This also speaks to Foucault's “governmentality and biopower” 51 as hidden forms of power relationships that essentially keep the poor, poor and the wealthy, wealthy. Despite all the rhetoric of development agencies, the poor remain excluded from global public goods.
Whose Knowledge Should We Value?
While the UK is considered an HIC and boasts a comprehensive and available health system, the provision of care for people with lymphedema is as patchy and inconsistent as the country's income distribution. There is a lack of policy to support sustainable change, which is aggravated by the complexity and lack of a clear definition of who pays for care and who is responsible for it. Care provision is largely based on biomedical, hierarchical, and paternalistic models rather than embracing empowerment models of health promotion, education, and prevention. And this is very much related to the creation of new markets in this area.
As any good economist will remind us, new markets never spontaneously emerge rather they are made by the activities of businesses who correctly sense a latent need and shift financial resources to make money. 52 In Uganda and Kerala, the poor have little agency and are disproportionately disadvantaged within the largely invisible social and political structures. De Maio 53 in a discussion of Farmer's work on structural violence demonstrates it is a PE analysis that exposes the root causes of inequality through understanding the nature of power relationships in the field of global health.
Other narratives and approaches to health beyond biomedicine emerge from more critical readings of public health. The “3rd public health revolution” 54 demands a new social contract that recognizes and values health in the following ways: as a public global good; a component of global security; strong systems of global governance; ethical business practices and social responsibility; and a social justice ethic. As a result, critical perspectives in global health have emerged that are both challenging the dominant biomedical narrative 55 and presenting different ways of approaching health problems.
In HICs such as the UK, some traditional health knowledges do survive, but largely in the informal and private health care sector, 56 but a bid for integration of complementary and alternative medicines into the NHS in the 2000s was never successful against a powerful medical lobby. As noted in the UK case study many of the current high-technology dressings and technologies for wound and lymphedema care have their roots in historical and traditional practices. It is common practice for Pharma to isolate the active compounds of a herb or traditional remedy, patent it, and market it at vastly inflated prices. An obvious example here is the journey of aspirin from willow bark to acetylsalicylic acid, but we are now seeing the increasing demands for chronic wound and lymphedema care driving European manufacturers to develop technologically sophisticated compression products. 57 The magnitude, the resources, and the power relationships behind scientific medicine mean that Illich's 58 warning of the power of medicine to overtake cultural ways of dealing with health and illness by presenting a medical approach as the only solution to our health problems, that is, cultural iatrogenesis, has become the dominant focus.
In terms of treatment of LF, compression therapy is widely accepted as the most appropriate with particular emphasis on skin hygiene (soaking with herbal solutions) and massage (with herbal oils). Costs here depend on location and the product utilized. Elastic and inelastic compression bandages are popular, but in the last 5 years, new compression devices and high-technolgy bandages are now being pushed by the medical devices industry. These are expensive. Bandages account for nearly ¾ of the cost of medicine and materials in India and it is increasingly difficult to locate competitive local suppliers of quality bandages. This is ironic as many of the new breeds of high-technology bandages are manufactured in India. The Indian Textile Association encourages the industry to export cotton-based products as an important source of foreign currency revenue. Here we see clear tension between local needs and foreign currency accumulation for wider development purposes. Yet pluralistic approaches to health can and do exist in tandem with biomedical systems in many LMIC settings, where biomedicine remains out of reach or too expensive for the many. As we have seen in India, Ayurvedic and AYUSH systems of medicine are culturally embedded and have been integrated into the Indian health care system although tensions exist.
The situation in Uganda is more mixed. While in theory, treatment is free at government-level facilities, in practice, stock-outs are frequent and access to medicines relies heavily on international donor-led programmes. As in much of Africa, the neoliberal forces of globalization and “development” have shaped and are shaping therapeutic landscapes in Uganda. The anthropologist Reynolds Whyte 59 talks about a “therapeutic marketplace” operating in the urban and increasingly rural areas that to counteract weak state provision, health infrastructures combine lifestyle, private, and pharmaceutical products to provide a mixture of biomedical, herbal, and traditional treatments for all sorts of health conditions. Traditional medicine is heavily used especially in rural areas, and so, while few studies exist about its use in LF, it is certainly an area for further exploration.
Traditional and cultural knowledge systems of health and healing have existed for many centuries, but in modern capitalist societies have been pushed aside in pursuit of scientific progress. These traditional perspectives understand and successfully hold multiple ways of knowing about health and illness based on different epistemologies. Local indigenous knowledge(s) draw on existing cultural and social capital. These systems have the potential to offer local, low-cost solutions, and the World Health Organization (WHO) 60 has long recognized the value in implementing policies that strengthen the role of traditional medicine in keeping populations healthy.
We have much to learn or maybe remember from these traditional contextual ways of doing health, as we saw in the Kerala case study, which demonstrates the variety of approaches that can be used to address the problem of lymphedema globally. Signs of progress come through the Indian model that seeks to integrate biomedicine with Ayurveda and Yoga. Cheap and successful, they are easily applied to both rural and urban settings and heterogeneous populations. The procedure, however, is labour-intensive requiring strict adherence. Education is key again. The Kerala case study demonstrates that IML offers opportunities to standardize interventions in densely populated, culturally diverse, resource-limited settings. However, even in India, private health and the market dominate. Yet, alternative and traditional care delivery systems are cheap, easily accessible, can be easily self-managed, and are culturally acceptable in Uganda and India. They are also more sustainable.
This leads us then to ask if the UK and other HICs could potentially strategize to adopt such models through their existing systems and learn from global South health systems. As well as exporting the best of clinical biomedical innovations and rolling them out globally and equitably, we would argue that there are also “low-technology” solutions and local knowledge(s) about treating LF that HICs can benefit from: that is, applying a “reverse knowledge innovation” in the treatment of lymphedema to the benefit of patients and also health systems. Western medical thinking has always been partly intuitive or speculative (even “nonscientific”). Limits to understanding have usually been recognized and there is very much an underlying disorder to health care understanding. This is its secret center.
The COVID crisis, for example, shows we know that we do not know, but how we respond institutionally to knowing that we do not know matters and is always political. This rather mysterious paradox has not, however, made health care knowledge less technical and more cautious. The opposite is true. Health care has become increasingly technical and assertive in its “knowing” and in so doing ever-more connected to the demands of capital and income generation. We also suggest that more understanding of the self-management of CO globally in all settings using a range of epistemological approaches can only add value to this new and emerging field of study.
Conclusion
The medical disease hierarchy affords CO care with a low status. This means at least two things: first, there is a knowledge gap as to the best way to tackle questions of definition, prevention, and treatment. Second, consequently, questions of prevention and treatment tend to be approached via biomedical imperial modeling that tends to negate more pluralistic and community-based thinking. These are issues that require us to rethink the wider “determinants of the determinants” of health and how they map in three diverse geographical, environmental, and socioeconomic settings.
We have tried to demonstrate how sets of power relationships and resource distributions influence and structure the provision of CO care globally. These intertwined and often invisible processes reflect a set of power relationships that do little to challenge the dominance of a model that focuses on high-technology, high-interventionist approaches then come to define the field yet are imposed onto LMIC settings. At the same time, evidence-based knowledge innovation in CO from LMICs is neither recognized nor valued. Understanding this PE of care in CO is a route to potentially providing more equitable health systems and joins the debate about achieving a comprehensive primary health delivery that IS accessible for the many rather than the few.
It is not just “politics” but more precisely PE—the interaction between politics and economics—that is the beating heart of true health promotion because it is here we pay attention to those who control, manage, and distribute financial resources. Here too the framing effect of a scientistic (biomedical in this case) epistemology—the standard health care professionals tend to use to judge—means health care knowledge has come to be legitimized using natural science standards. This should be problematized if the who gets what, when, where, and why questions are marginalized, ignored, or lost in translation. However, this should not come as a surprise to us.
Footnotes
Acknowledgment
The authors would like to acknowledge the support provided by the International Lymphoedema Framework in support of this study and article.
Authors' Contributions
L.G., J.G., and C.J.M. were involved in article conceptualization and design. S.N., S.N.K., C.J.M., E.D., L.K., A.N., and D.I. undertook the data collection for the case studies. All authors were involved in the evolvement of the study conceptualization, interpretation of cases, and article writing. All authors read and approved the final article.
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research (NIHR), or the Department of Health and Social Care.
Author Disclosure Statement
D.I. is funded by the National Institute for Health Research (NIHR) Applied Research Collaboration Kent, Surrey, Sussex. The authors L.G., C.J.M., J.G., A.N., S.N., L.K., E.D., and S.N.K. declare no competing or conflicts of interest in producing this original article.
Funding Information
D.I. is funded by the NIHR Applied Research Collaboration Kent, Surrey, Sussex.