
Abstract
Background:
To estimate the prevalence and impact of chronic edema (CE) in two Irish health care settings as part of LIMPRINT, an international study developed and co-ordinated by the International Lymphoedema Framework (ILF), and researched in Ireland by the National Lymphoedema Framework Ireland (NLFI).
Methods and Results:
Data were collected using clinical assessment tools previously validated by the ILF. Three hospital settings were chosen, both an in-patient and out-patient oncology unit in Galway and a vascular out-patient unit in Dublin. Patients attending an oncology clinic or in an in-patient ward on a specified day were invited to participate as desired, and all patients attending vascular out-patients for a 4-week period were included in the study. All patients were assessed for the presence of CE, and if present, patients were asked to answer several questionnaires regarding diagnosis, available services, quality of life, and wound care where appropriate. The collection of data was anonymized and was inputted to a central database (Clindex). A total of 152 patients were assessed, 76 from the oncology service and 76 from the vascular service. Eighty-seven (57%) patients were female and 65 (43%) patients were male. The mean age was 65 years with a range 15–93 years. Twenty-five patients (16%) had CE, 8 (11%) in the oncology service and 17 (22%) in the vascular service. All the oncology patients were normal weight while almost 60% (n = 10) of the vascular patients were obese. Two (25%) of the oncology patients had a history of cellulitis, whereas seven (41%) of the vascular patients had a history of cellulitis. Four of the oncology patients (50%) received full lymphedema management whereas two oncology patients (20%) received no treatment at all. In contrast, in the vascular group, only two patients (12%) received full lymphedema management. Eight patients (47%) were receiving no treatment at all and seven (41%) were in compression garments and received skin care advice only.
Conclusion:
Though number of patients are small, these results highlight the high prevalence of CE in both oncology and vascular service patients as well as the disparities in management. In addition, there is a high incidence of cellulitis reported that is possibly not surprising given the low number of patients receiving full lymphedema care. Good data collection is essential if we are to provide and fund a comprehensive service in the future.
Introduction
Lymphedema is a chronic swelling due to lymphatic system failure. It can be primary, resulting from failure of lymphatic development or function, or secondary, after damage to the lymphatic system (e.g., cancer treatment, injury). It can affect any part of the body, but most commonly affects the limbs. Its prevalence is often reported as increasing due to improved cancer survivorship, but equally important is its improved recognition in other diseases, for example, venous disease, cardiac failure, obesity, and immobility.1–4 Chronic edema (CE) is defined as edema that has been present for greater than three months regardless of its etiology. LIMPRINT (Lymphoedema IMpact and PRevalence—INTernational) was an international study aimed at capturing the size and impact of CE in different countries and health services across the world. 5 The project was co-ordinated by the International Lymphoedema Framework (ILF) through its participating national frameworks. LIMPRINT was a two-phased study. Phase 1 was conducted from June 2013 to 2014 with the validation of the core tools used in phase 2. Phase 2 involved the roll out of these tools to 9 countries and 40 sites. Ireland joined in the last few months of phase 2.
LIMPRINT's primary aim was to identify the number of people with CE within differing countries and to determine its impact on patients. It believed that these data would
establish the size of the problem of CE,
provide the basis for evidence-based practice, and
be used to facilitate improved reimbursement.
An international data set of >13,000 patients was collected. The study was supported by an electronic data capture system and data collection tools that had been previously validated (Clindex). The National Lymphoedema Framework Ireland (NLFI) was set up in November 2015 and as one of the ILF frameworks requested to and was invited to join the study despite proximity to its completion. The recent HSE Model of Care for Lymphoedema/Lipoedema 6 has highlighted the lack of Irish data, and NLFI joined the international study to help gather relevant local data as part of the effort to inform and influence education, management, and resources allocation for those medical conditions that can give rise to CE.
Materials and Methods
Data were collected using clinical assessments tools previously validated by the ILF. These tools included the Core Tool, Quality of Life Tool, EQ-5D, upper limb and lower limb-specific Lymqol Quality of Life Tool, details of Swelling tool, Cancer Tool and Wound Tool. Three hospital settings were chosen, both an in-patient and out-patient oncology unit in Galway and a vascular out-patient unit in Dublin. Patients attending an oncology clinic or in an in-patient ward on a specified day were invited to participate, and all patients attending vascular out-patients for a 4-week period were included in the study. Inclusion was not age limited as it was considered important to gather information if possible, on children. Parental consent was obtained in this instance.
All participating patients were assessed for the presence of CE by clinically eliciting a positive pitting test or a positive Stemmer Sign. The duration of swelling was obtained from the patient. Patients who were diagnosed as having CE (present for >3 months) were then asked to complete a series of validated questionnaires, already described, depending on the etiology of their edema and/or the presence or absence of wounds. The collection of data was anonymized and was inputted to a central database (Clindex). Country-specific data were generated and returned to each individual country. The Irish data were also validated locally.
Results
A total of 152 patients were assessed, 76 from the oncology service and 76 from the vascular service. Eighty-seven (57%) patients were female and 65 (43%) patients were male. The mean age was 65 years with a range 15–93 years. Twenty-five patients (16%) had CE: eight (11%) in the oncology service and 17 (22%) in the vascular service.
Figure 1 shows the age range of both the overall population and the patients with edema.
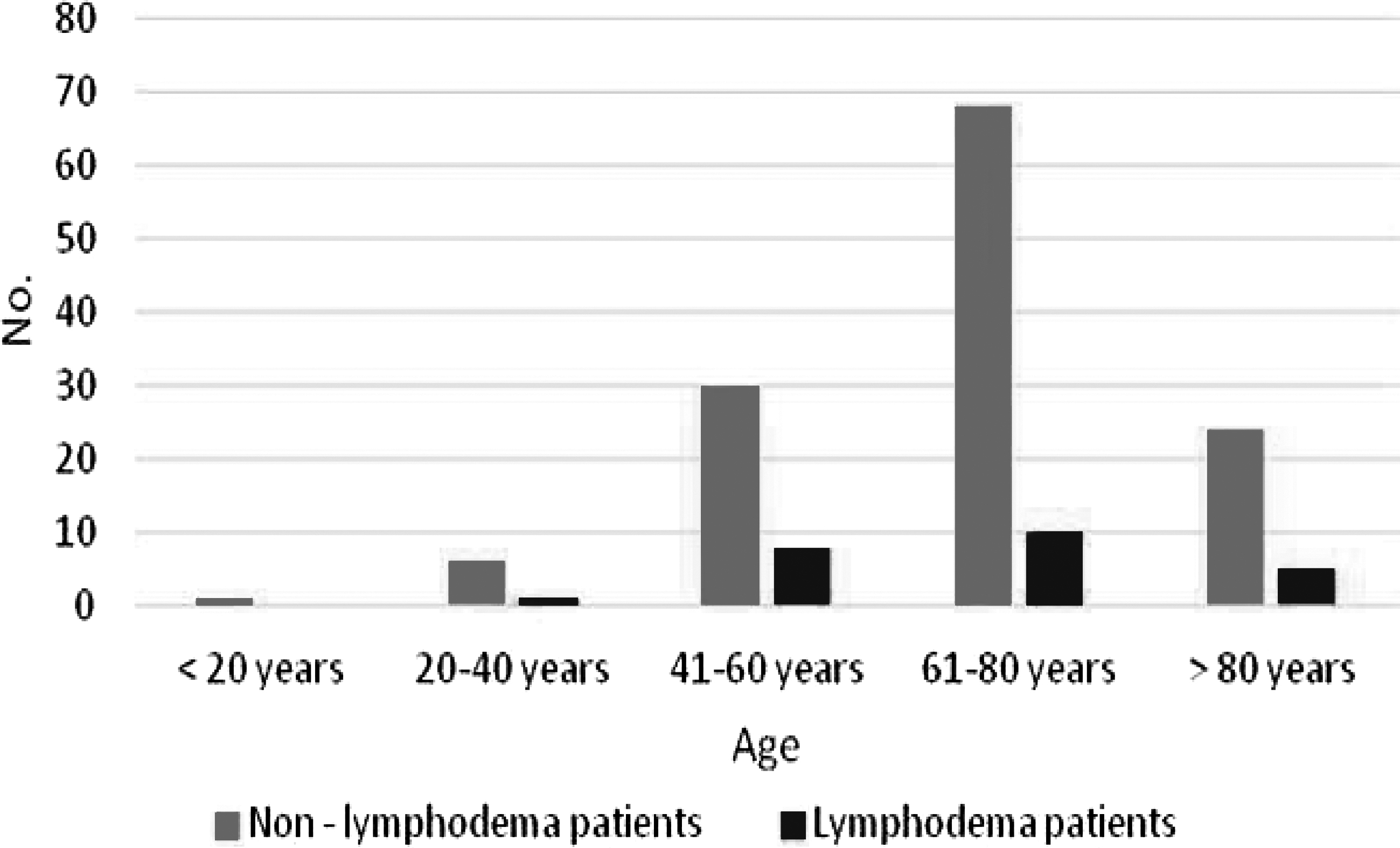
Age distribution.
The highest incidence of CE was found in the age group 41–60 years where the incidence was 27%. There were a total of 30 patients in this age group: 21 oncology patients and 9 vascular patients. Three of the 21 oncology patients had CE, whereas 5 of the 9 vascular patients had CE. Also of interest is the high incidence (21%) in the older age group (>80 years); all of these patients were in the vascular cohort.
There was a wide variation in the length of history of the presence of CE, varying from <6 months to >10 years (Fig. 2). Seventy percent of the vascular patients had a history in excess of 5 years.
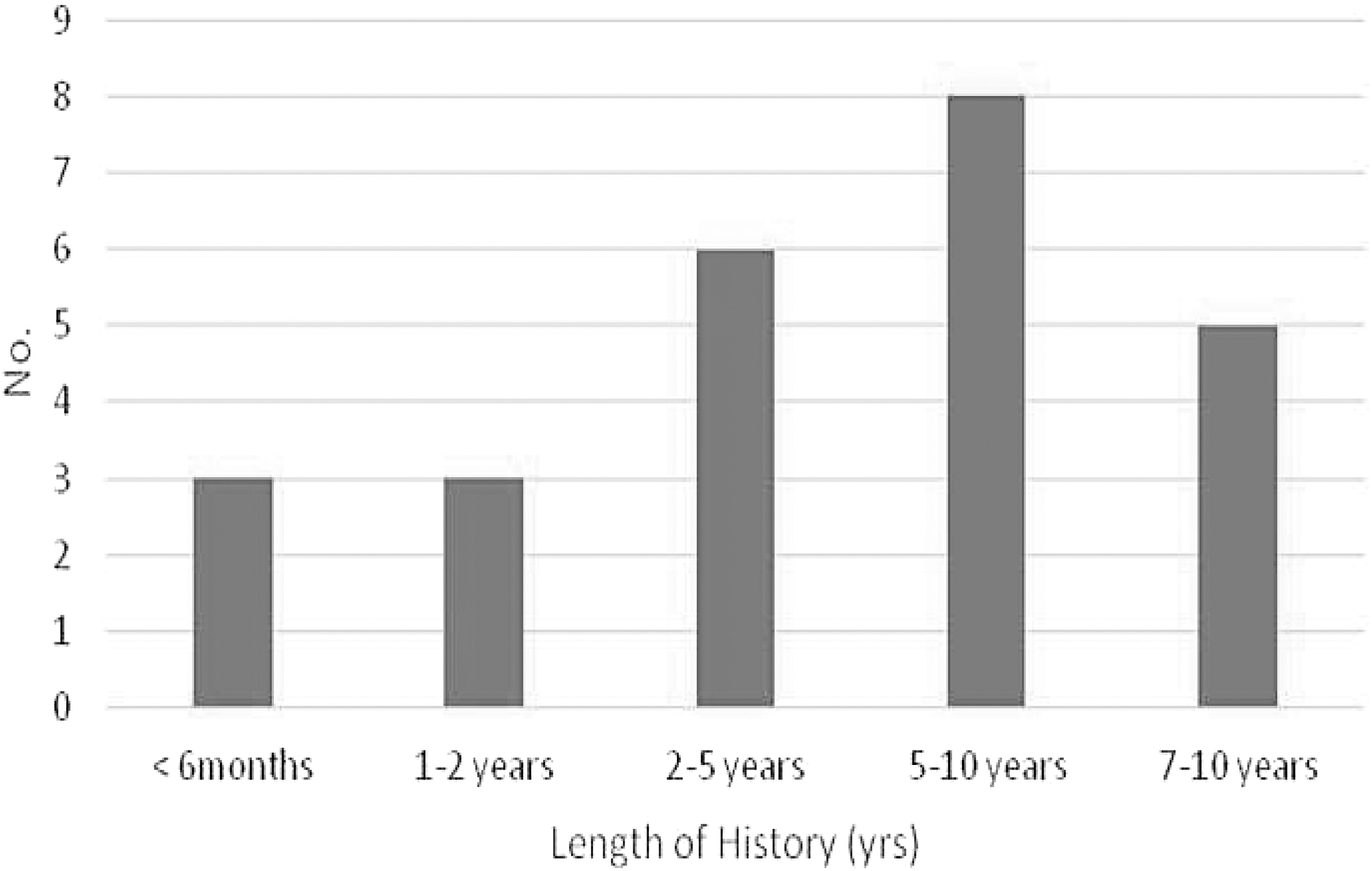
Length of history.
Figure 3 shows the etiology of the lymphedema. Twenty-eight percent (n = 7) had primary lymphedema. Thirty-six percent (n = 9) had edema secondary to cancer, whereas 20% had edema associated with underlying venous disease (n = 5). Two patients had lipedema and in the remaining two patients their CE was considered secondary to immobility and obesity, respectively.
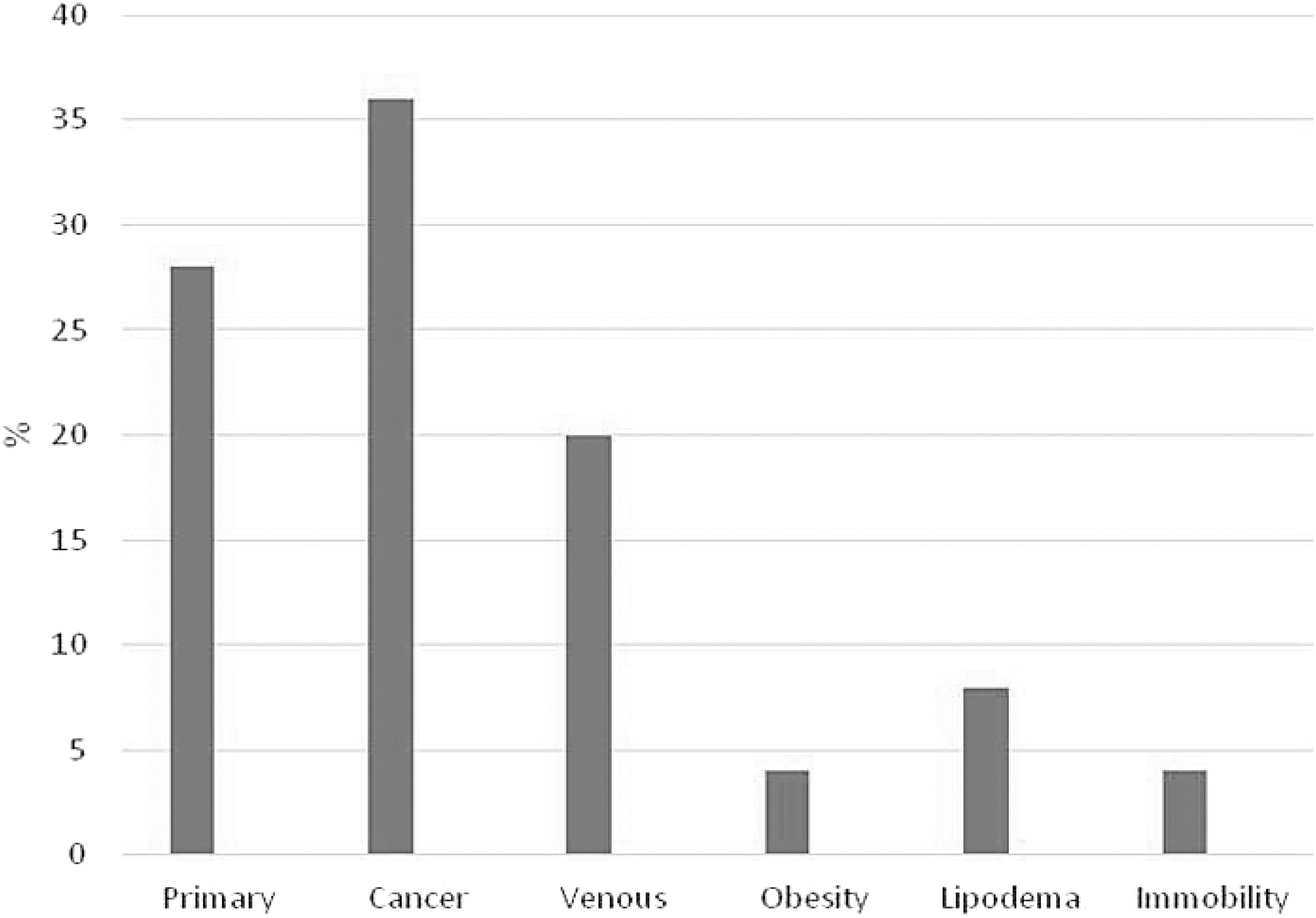
Etiology of chronic edema.
The lower limbs alone were affected in all the vascular patients. In the oncology group, three patients had unilateral upper limb swelling, two had unilateral lower limb swelling, and three had bilateral lower extremity swelling with one patient also complaining of abdominal edema.
None of the oncology patients were overweight, whereas 10 (59%) of the vascular patients were obese. Unfortunately, this information on the remaining cohort of patients who did not have CE is not available. Figure 4 shows the percentage obesity by age in the CE group. This varies from 100% in the younger age group to 50% in the old age groups.
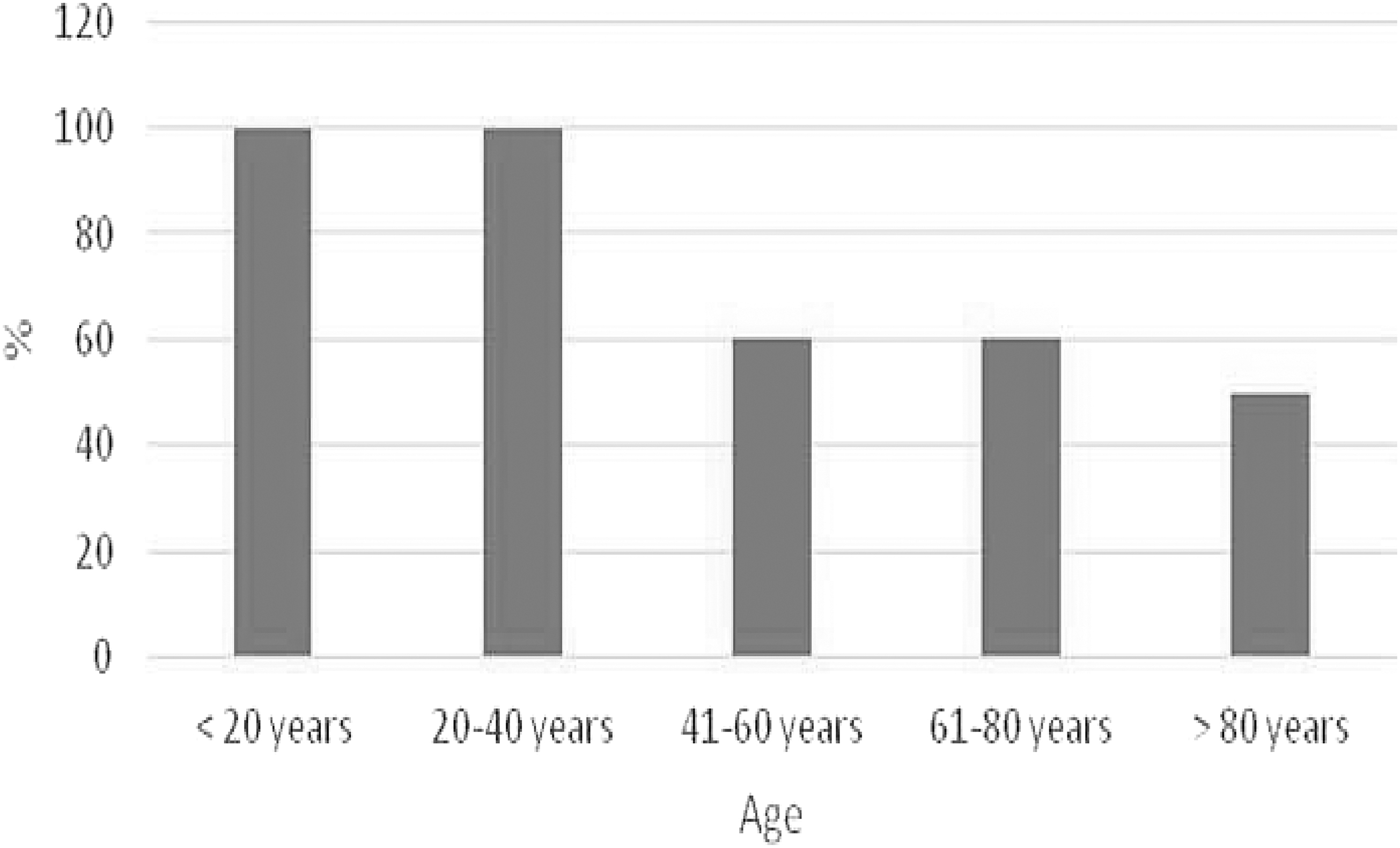
Obesity and age distribution.
A history of cellulitis was elicited in a total of nine patients: two in the oncology group (25%) and seven in the vascular group (41%). It was >1 year since either of the oncology patients suffered an episode of cellulitis and neither had ever required hospitalization for cellulitis. Only one of the vascular patients had been hospitalized for cellulitis in the past year.
Nine patients (36%) reported wounds, two in the oncology group and seven in the vascular group. One of the oncology wounds was a surgical wound and the other after cancer management. Seven of the 17 vascular patients (41%) had wounds related to their leg swelling. All were treated with compression bandages.
In terms of management of their edema, again there was wide variation (Fig. 5) among patients. Unfortunately, nearly one in three patients received no treatment. Forty percent received compression alone and only six patients (24%) received the full range of treatment: two vascular and four oncology. Some of the main categories of treatment reported as received included skin care advice, wound dressings, antibiotics, massage (including MLD), physiotherapy (not massage), compression garments, exercise advice, and cellulitis advice.
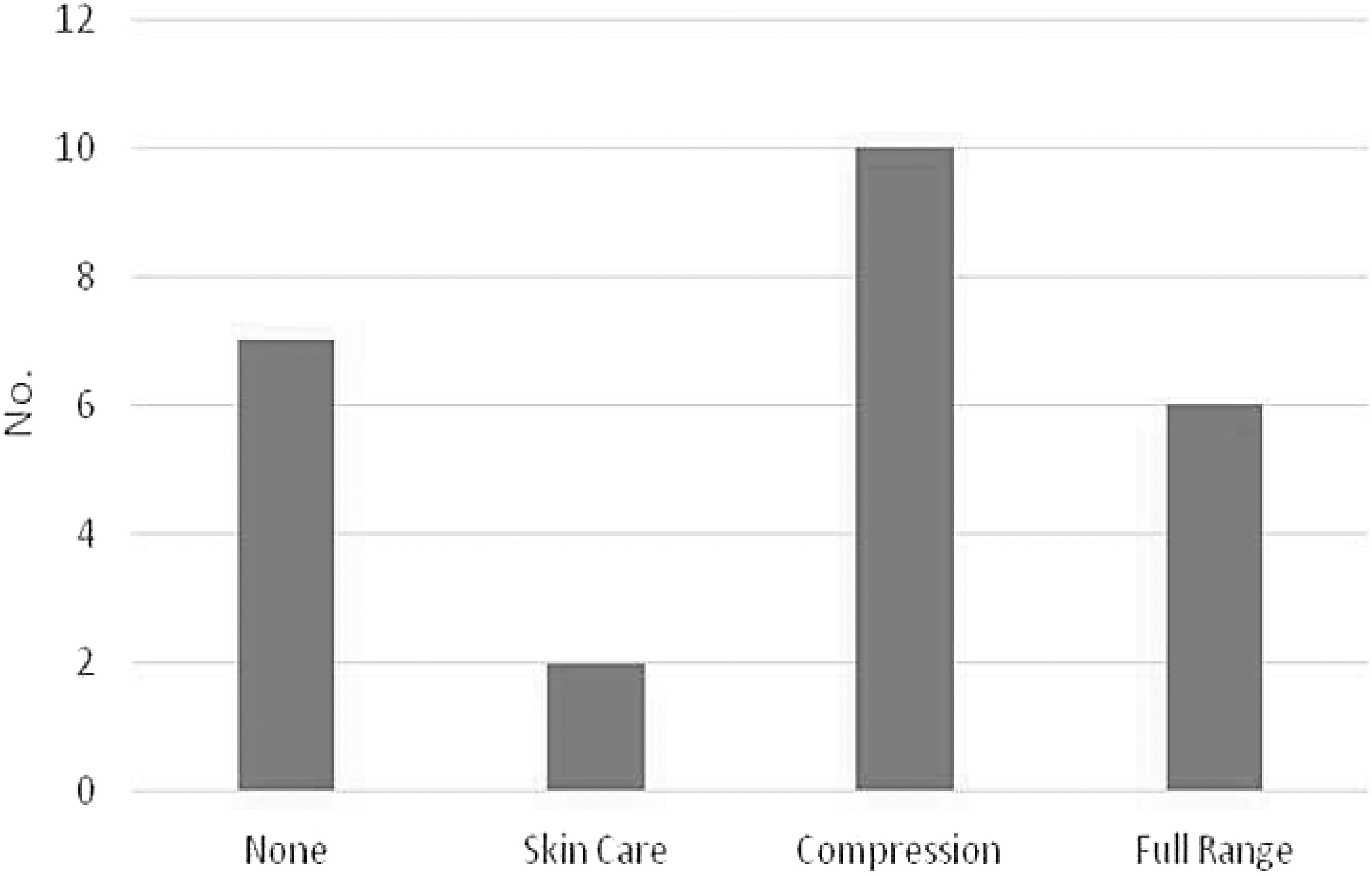
Received treatment.
Participating patients were asked to rate their quality of life on a 10-point visual analogue scale with 0 being poor and 10 excellent. Figure 6 shows that CE reduces quality of life in the majority of patients.
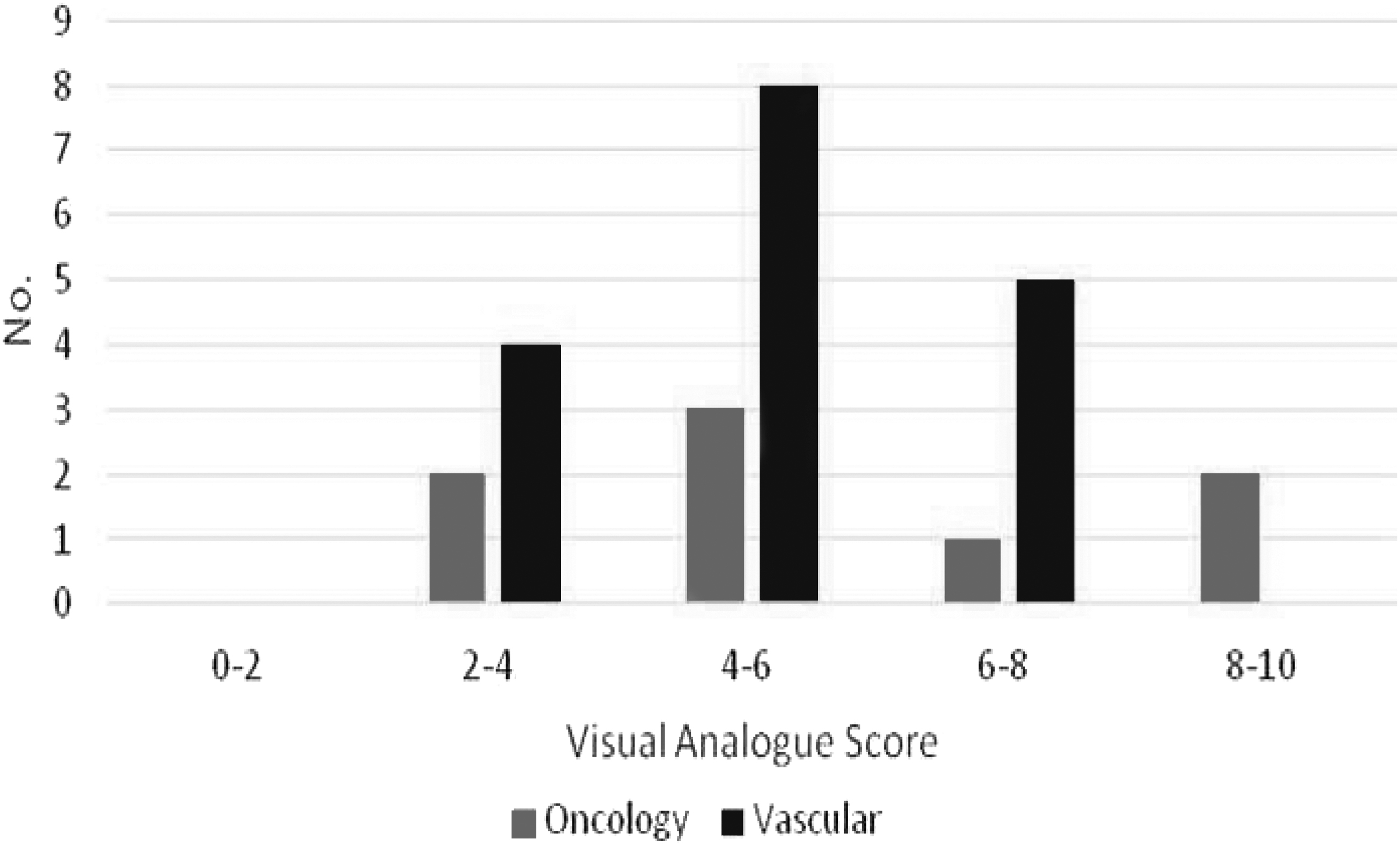
Quality of life.
Discussion
Lymphedema/CE is a chronic swelling that is often overlooked by clinicians. It can occur at any age, and if left untreated can have debilitating consequences.
LIMPRINT's primary aim was to identify the number of people with CE within differing countries and to determine its impact on patients. 5 Unfortunately, there is no Irish data on the prevalence of lymphedema and the recent HSE Model of Care looked to the United Kingdom to extrapolate the number of patients in Ireland with lymphedema/CE. One of the first reports was by Moffatt in 2003, 1 wherein a prevalence of 1.33 per 1,000 population was reported that rose to 5.4/1,000 in the >65-year olds. In 2017, Moffatt et al. 2 reported a prevalence of 3.99/1,000 population, whereas in Northern Ireland, a prevalence of 4.83/1,000 was also reported. An excellent meta-analysis from Torgbenu et al. 7 in 2020 suggested a 27% incidence of arm lymphedema postbreast cancer. There were insufficient data to make meaningful assessment of leg lymphedema. Although our incidence of 11% in cancer patients is lower than reported studies,7–9 our population was small, included a mix of cancer diagnoses and patients were at varying stages of their cancer treatment.
More attention has been given of late to the noncancer secondary edema as this population is often overlooked. This cohort may have complex underlying medical conditions and may have the greatest impact on the health service in the future in terms of morbidity and cost.10,11 We report an incidence of 22% in this group. If one looks at the combined LIMPRINT data, an in-hospital incidence of 38% was reported, 12 whereas in nursing communities a staggering 56% were found to have CE. 13 These findings emphasize the underestimation of CE in the population which, in turn, raises issues for health funding.
The HSE Model of Care concluded that “service provision for lymphoedema/lipedema is inadequate in most parts of Ireland with significant gaps across the country and inequity of access for nononcology related lymphoedema.” 6 Our findings would confirm this conclusion. We found that only a quarter of all patients were receiving a full range of treatment. To our surprise, 25% of cancer-related lymphedema patients were receiving no treatment and only half were receiving a full range of treatments. Less surprisingly, only two of the vascular patients (12%) were receiving a full range of treatment. Fifty percent of the vascular patients were in compression and would have hopefully progressed from compression bandages to compression garments. However, in the absence of ancillary lymphedema care, one would have to question how good long-term compliance would be.
The association of CE and wounds is well accepted, and our findings mirror those of the Canadian Limprint group who reported an incidence of 40%. 14 This emphasizes the additional costs associated with this patient cohort. Wound care costs have been estimated at £7600.00 for treating a single venous leg ulcer. 15 Wounds secondary to CE are often more difficult to heal, suggesting this cost will be greater. Leg ulcer services should be utilized to help identify patients with CE and ensure adequate long-term care.
Collective LIMPRINT data from specialist Lymphedema Services in four countries found a history of cellulitis was reported in 32% with primary lymphedema compared with 35% of those with secondary edema. 16 These findings are very similar to ours. Two of our five patients (40%) with primary lymphedema reported a history of cellulitis. Of the remaining 20 patients with secondary lymphedema, 8 (40%) reported a history of cellulitis with 1 being hospitalized in the past year. In a very recent report by Burian et al., 17 they reported a significant reduction in the incidence of cellulitis in CE by the simple use of compression.
Although our study is limited by small number of patients, our findings mirror those of others throughout the world. It is clear that the prevalence of CE is underestimated. It is associated with a high incidence of cellulitis and obesity. Our findings confirm the conclusions of the HSE Model of Care in terms of access to treatment. The provision of accurate epidemiological data is essential to provide a basis for accurate service provision and funding. We hope this snapshot of CE in Ireland will encourage others to collect data on this often overlooked patient group and will be an integral part of the HSE Model of Care as it is rolled out.
Footnotes
Acknowledgments
We thank the personnel who helped with data collection. These included Catherine O'Sullivan, Fionnuala Ginty, Fiona Melia, and Miriam Flatley from the Physiotherapy Department in Galway University Hospital and nursing students from Trinity College Dublin and St. James's Hospital.
Authors' Contributions
M.-P.C. contributed to writing—original draft, review, and editing (lead), data curation, and formal analysis. N.K. was involved in writing support and editing, data collection, and input. B.H. took care of writing support and editing, data collection, and input. E.G. carried out database software support and data input. K.M. was involved in data collection. M.M.S. carried out conceptualization, co-ordinator with ILF to secure NLFI involvement, and secure research tools. All authors were involved in the revision and final approval of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.