
Abstract
Background:
Chronic edema (CO) is a complex condition, arising from different factors, including immobility and obesity. Edema and obesity can have a significant impact on quality of life of patients and their families. Understanding how to manage edema in obese patients is an increasing challenge for both patients and clinicians. As effective treatment options are limited for this population, it is more cost-effective for patients to lose weight before starting treatment. When patients cannot maintain weight loss, one option is to have bariatric surgery.
This study was part of LIMPRINT: Lymphedema IMpact and PRevalence INTernational, a study with the aim of identifying the prevalence and impact of CO in different countries and health care settings.
Study Purpose:
To evaluate the prevalence and impact of CO among patients in a United Kingdom bariatric surgical service.
Methods and Results:
The gold standard pitting test assessed the presence of edema. General (EuroQOL-5 Dimensions [EQ-5D], RAND 36-Item Short Form Health Survey, Version 1.0 [SF-36], Generalized Anxiety Disorder 7-Item Scale [GAD-7] and Patient Health Questionnaire–9 [PHQ-9]), and edema-specific (Lymphedema Quality of Life [LYMQOL]) quality-of-life questionnaires were used to evaluate impact of edema.
The prevalence of edema was 52.1% (25 of 48 participants had edema), potentially linked to obesity, immobility, and medications. Most participants had International Society of Lymphology (ISL) Stage I edema. There were no statistically significant differences between the quality of life of participants with and without edema. However, comparing SF-36 results and normative population data indicated that quality of life was much lower than those in the normative population.
Conclusions:
This study highlights the high prevalence of edema and low quality of life of this bariatric population. ClinicalTrials.gov ID: NCT03154593.
Introduction
Chronic edema
The definition of chronic edema (CO) is: persistent swelling, present for 3 months or more. 1 It is primarily found in the upper and lower limbs, but can be present throughout the body.1,2
CO is complex and occurs due to different causes and mechanisms, including immobility, inefficient lymph drainage, chronic venous disease, and obesity.1,2 If CO becomes worse, it can result in cellulitis and skin conditions (like chronic lipodermatosclerosis and lymphangiectasia).3,4
The main treatment of CO is through decongestive lymphedema therapy (DLT), a combination of skin care to reduce infection risk, and compression bandaging (or garments) and exercise to encourage lymphatic functioning. 4 CO can have a severe impact on the daily lives of patients and their families, affecting them physically, socially, and psychologically. 2
CO and obesity
There is a growing recognition of CO occurring in the obese population. Causes include: increased lymph production rate as the capillaries overload the normal lymphatic transport system, obesity causing raised venous pressure, local venous insufficiency contributing to high lymphatic flow, and lymphatic blockage (e.g., by surgery-associated trauma). 5 However, the true mechanisms which cause CO have not been fully examined.
Obesity is a well-recognized international epidemic. 6 In a recent study assessing patients from specialist lymphedema services in the United Kingdom, France, Italy, and Turkey, 7 34.5% of patients were obese (body mass index [BMI]: 30–39.9) and 18.4% were morbidly obese (BMI: >40).
This high prevalence in obesity causes an increase in the prevalence of health-damaging comorbidities. As well as edema, obese patients commonly have hypertension, type 2 diabetes, and cardiovascular disease.8,9 Obesity impairs quality of life (physically, mentally, and psychosocially): affecting mobility, social interaction and self-esteem. 10 Furthermore, obese patients often find weight loss difficult to achieve or maintain due to genetic and environmental influences (including hormonal, metabolic, neural, and physical factors). 11
It is a challenge for patients and clinicians to know how to manage CO in obesity. Treating patients is often impractical and inefficient through traditional methods, like DLT. 12 Obese patients often do not seem to have sustained improvement following intensive compression bandaging. Although the treatment is effective, the edema will recur if the issue of obesity is not addressed. 13 It is difficult for patients to manage their own treatment, and for clinicians to modify compression materials to exert the correct pressure on the limbs and to achieve good outcomes with regard to quality of life. 14
Bariatric surgery
As effective treatments are limited for this population, it is more cost effective for patients to lose weight before treatment plans are implemented. 15 However, if they fail to maintain weight loss through diet, exercise, or medication, one option is to have bariatric (weight loss) surgery. The aim of this surgery is to reduce food storage capacity by reducing the size of the stomach, by performing a laparoscopic gastric bypass, gastric band insertion, or sleeve gastrectomy. 16
Bariatric surgery has a strong effect on metabolic and hormonal systems, causing changes in: gastrointestinal hormone secretion and metabolism of bile acid. 17 It also affects the hypothalamus-brain stem axis (which regulates energy balance for food intake). This reduces energy intake and improves glycemic control. 18 Consequently, bariatric surgical procedures often result in patients losing and maintaining weight loss, and achieving an improved quality of life and a reduced range or severity of obesity-related comorbidities (such as Type 2 diabetes and hypertension).10,19
Current prevalence literature
Although several studies have estimated the prevalence of CO in an obese/bariatric population, and others have estimated the prevalence of obesity in an edematous population, most have methodological limitations.20–23 These limitations include: a small sample size, unclear recruitment procedures, or definitions of CO or lymphedema.
Inge et al., 24 O'Malley et al., 25 and Fife and Carter 13 adopted and described clear methodologies, however the prevalence estimates for CO in these groups of obese participants varied widely: 6.2% (93 of 1502), 33% (107 of 324), and 74% (11,100 of 15,000), respectively. These discrepancies could be due to the researchers adopting different definitions of CO or reliance on population medical records.
The authors of this article designed a prevalence study in a bariatric population, with a clear CO definition and a definitive recruitment method. The study was completed at the East-Midlands Bariatric & Metabolic Institute (EMBMI) in the Royal Derby Hospital (RDH), assessing patients new to the bariatric service who received diet and psychological advice in preparation for having bariatric surgery.
This study was part of LIMPRINT: Lymphedema IMpact and PRevalence INTernational, a study under the International Lymphedema Framework. LIMPRINT has the aim of identifying the prevalence and impact of CO within diverse health services in different countries throughout the world. 26
Objective
The study objective was to determine the prevalence and impact of CO on the health-related quality of life (HQoL) of a population of obese patients referred to a United Kingdom bariatric service in RDH for consideration of surgery to reduce their morbid obesity.
Materials and Methods
Study population and recruitment
The study was approved by the Liverpool Central Research Ethics Committee (Study IRAS ID: 198766) and took place at the EMBMI (referred to hereafter as: the bariatric clinic) in RDH. Patients were newly referred to the weight-management clinical pathway. The clinic required patients: to have a BMI of ≥40, or 35 kg/m2 with obesity-related comorbidities (e.g., diabetes and heart disease), and to have tried to lose weight previously through diet, exercise, or medication. Clinic appointments consisted of consultations with a bariatric nurse, physician, and dietician, who prepared them for having bariatric surgery. Patients who scored highly on anxiety and depression questionnaires, GAD-7 (Generalized Anxiety Disorder 7-Item Scale) and PHQ-9 (Patient Health Questionnaire–9), were also seen by a clinical psychologist.
The aim was to recruit 180 people, from new patients to the service (normally 8 each week) over a 6-month period. To reduce recruitment bias, the objective was to recruit a consecutive sample of patients. Recruitment took place during the first clinic appointment of the weight management clinical pathway, before bariatric surgery, while patients were waiting to see one or more members of the bariatric team and/or at the end of their appointment. Recruitment commenced in August, 2016 and ended in March, 2017. The inclusion criteria consisted of adult patients at their first clinic appointment, who could give informed consent and who could understand English. The study was undertaken by one researcher trained in lymphedema assessment methods (A.N.).
The study assessment methods consisted of a clinical assessment, fluid measurements (through bioimpedance and tissue dielectric constant techniques), and completion of generic and edema-specific HQoL questionnaires. Each assessment lasted 50–60 minutes.
Clinical assessment
To determine the presence and extent of CO, the researcher assessed the presence of CO at the foot, ankle, lower limb (below and above the knee), and abdomen. The pitting test (primarily) and Stemmer's sign techniques were used to assess for the presence of CO. The pitting test was the gold standard, used to define the cases of CO.
Medical and CO-related information were recorded to help determine the cause(s) of and impact on the CO (if present): blood test results, medical history, medication, and mobility; and CO-related questions: history of cellulitis, duration of CO, International Society of Lymphology (ISL) stage of CO, skin conditions, and wounds. The ISL stages of CO 27 are: slight pitting edema that subsides with limb elevation (Stage I); severe pitting edema, limb elevation alone rarely reducing the edema (Stage II); and hard (fibrotic) tissue with skin changes such as thickening and hyperpigmentation (Stage III). Furthermore, the study team looked for conditions that may cause CO, including: heart failure, history of cellulitis, and obstructive sleep apnea; and medications that could exacerbate CO, like calcium channel blockers.
Quality control checks were carried out by a clinical lymphedema specialist (V.K.). All clinical data (including foot/lower limb photographic records) were inspected by V.K. to verify the presence/absence of CO and ISL staging.
Fluid measurements
Fluid measurements were taken to determine: which technique was more effective at detecting the presence of CO and whether they could be used to define chronic CO. These results will be published separately.
Quality of life
Participants completed the following general and edema-specific HQoL questionnaires: EQ-5D (EuroQOL-5 Dimensions), 28 LYMQOL (Lymphedema Quality of Life, if the participants had CO), 29 and SF-36 (RAND 36-Item Short Form Health Survey, Version 1.0). 30 Anxiety and depression questionnaires, GAD-7, 31 and PHQ-932 were completed as part of their bariatric appointments.
As the study consisted of a heterogeneous population sample, the SF-36 questionnaire scores were compared with a normative dataset from the Health Survey for England (HSE) 1996, 33 consisting of adults 16–74 years of age living in private houses.
The EQ-5D, LYMQOL, and SF-36 questionnaires are used extensively in lymphedema trials. They were completed to enable comparisons to be made with other studies. EQ-5D is a quality-of-life health index. LYMQOL is a lymphedema-specific HQoL instrument, used for upper and lower limb CO assessments, and to assess impact of CO on HQoL. The questionnaire consists of: function, appearance, symptoms, and mood (range: 1.0–4.0, no impact to maximum impact), and HQoL (range: 1.0–10.0).
The SF-36 questionnaire measures physical health (range: 0–100.0, worst to best health scores). Although it is generic, it is sensitive to change 34 and covers many of the areas affecting people with CO: physical functioning, role limitations (RL) due to physical health, RL due to emotional problems, energy/fatigue, emotional wellbeing, social functioning, pain, and general health.
Using both edema-specific (LYMQOL) and generic (EQ-5D and SF-36) questionnaires is valuable. Solely using generic questionnaires may not prove sensitive enough to assess changes in a particular condition because they are designed to assess HQoL across a variety of conditions. However, using condition-specific questionnaires in combination with generic questionnaires should provide more sensitivity to change because they have been designed with specific patient groups in mind. 35
The GAD-7 and PHQ-9 questionnaires measured anxiety and depression. The bariatric clinic patients completed them as part of their appointment, therefore their data were extracted from the participants' medical records.
Statistical analysis
The statistical programs, Stata and SPSS, were used. Data from the pitting test (number of participants to have CO) were analyzed to determine the proportion (with 95% confidence intervals) of participants with CO. Student's t and chi-squared tests were applied to demographic characteristics and cellulitis histories to compare participants with and without CO. T-tests were calculated to compare the HQoL of participants with and without CO to determine if the values differed significantly (significance: ≤0.05). These t-tests analyzed the impact of CO on HQoL, health utility, anxiety, and depression.
Chi-squared tests were applied to the data derived from PHQ-9 Question 10: “If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people?” The tests were run to compare the HQoL of participants with and without CO to determine the statistical significance.
Results
Prevalence of CO
Out of the 183 new patients attending the bariatric clinic during the recruitment period, 48 met the inclusion criteria and consented to take part, and 30 patients declined (Fig. 1). The prevalence of CO in this bariatric population was 52.1% (95% confidence intervals: 37.4%–66.7%) with 25 of the 48 participants having CO.
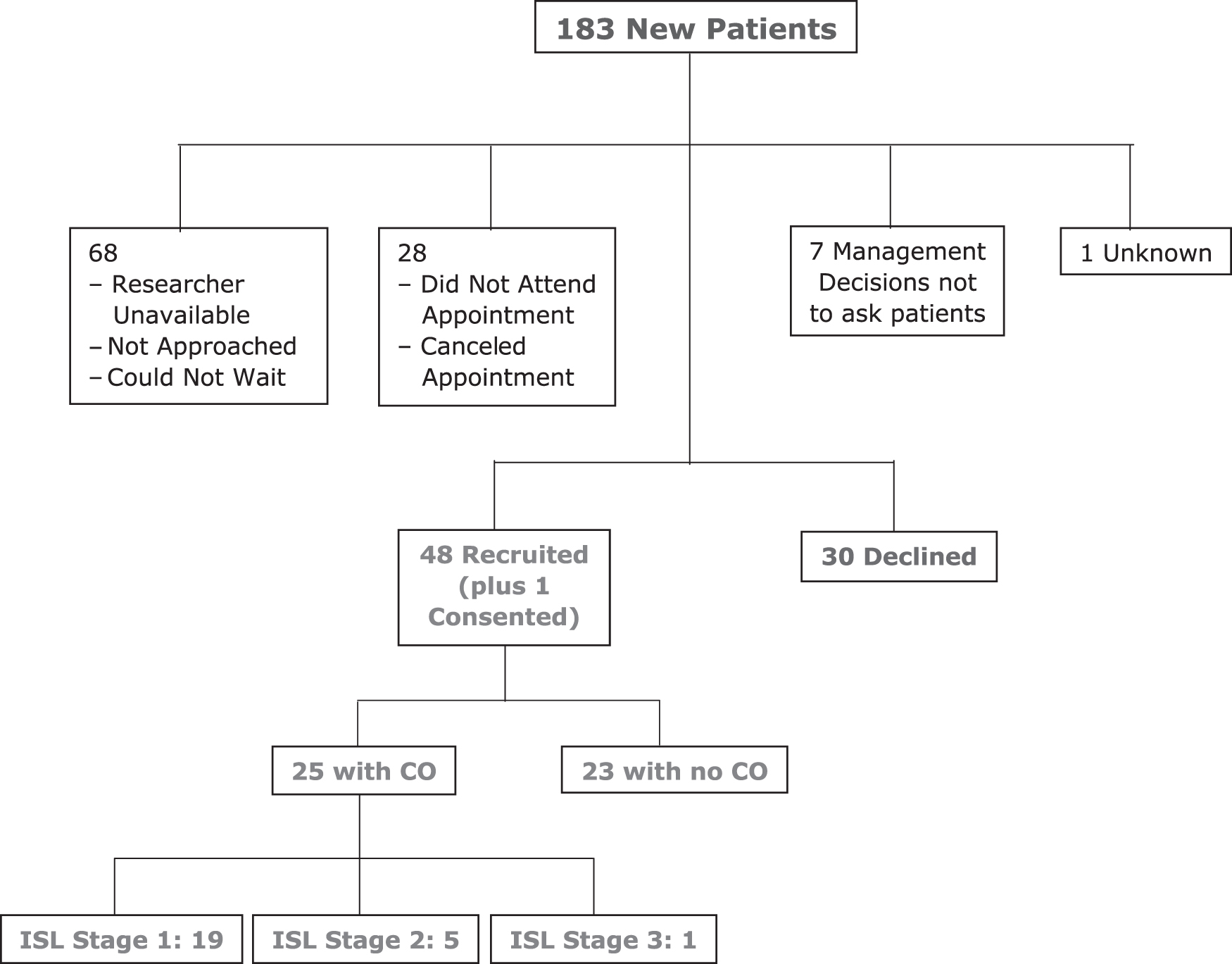
Screening log.
Demographic characteristics were recorded and statistical tests run to compare participants with and without CO (Table 1 and Supplementary Tables S1, S2). The comparison demonstrated that those with CO had a higher age and weight range, and a greater number of histories of cellulitis. Their age range and cellulitis history were significantly different than those without CO. The majority of participants with CO were in the 50–60 kg/m2 BMI category (Table 2).
Comparison of Characteristics Between Participants With and Without Chronic Edema
Bold: significant difference.
BMI, body mass index; CE, chronic edema; NCO, no chronic edema.
Body Mass Index Classification
Total number of participants compared with those with CO are identified next to their appropriate BMI class.
BMI classification reported by: World Health Organization. 36
Participants with CO had a greater number of positive Stemmer's signs (n = 6 compared with n = 1). They also had severe skin conditions on their lower limbs, including chronic lipodermatosclerosis (n = 6), lymphangiectasia (n = 2), and hemosiderin staining (n = 1).
Severity of CO
Most of the 25 participants with CO had soft ISL Stage I edema on their feet and shins (Fig. 1, n = 19). Other edema locations included ankles and lower arms. Six participants had ISL Stage II (n = 5) or ISL Stage III (n = 1) edema. Five had chronic lipodermatosclerosis or lymphangiectasia, however one participant with ISL Stage II edema only had skin creases with severe pitting CO.
The duration of edema was recorded as ranging from less than 6 months to greater than 10 years. One participant was unaware of her edema. Only five participants had been told the reason for their CO (including fluid retention, lymphedema, and right knee surgery).
Potential contributors of CO
Blood test results, comorbidities, medications, and hormone treatments were reviewed to highlight any that could have contributed to the participants' CO (Table 3). High brain natriuretic peptide (BNP) levels in two participants with CO were identified (671 and 862 ng/L), indicating that heart failure may have contributed to their CO. Although a considerable number of medications and hormone treatments had a potential side effect of CO (Table 4), a comparison indicated that these were commonly taken by participants with and without CO. However, a higher percentage of participants with CO (24%) took calcium channel blockers compared with participants without edema (10.9%). A higher percentage of those with CO also took HMG-CoA reductase inhibitors (statins) (24%, compared with 13%).
Comparison of Potential Edema Contributors Between Participants With and Without Chronic Edema
Frequency of Chronic Edema Contributors
Impact of CO
A comparison between SF-36 study data and HSE normative data (Table 5) indicated that the study participants had a much lower HQoL than others of the same age and gender who were not morbidly obese.
Comparison of 36-Item Short Form Health Survey Scores and Health Survey for England Normative Data
The means of study SF-36 questionnaire scores were compared with normative data from HSE 1996 (HSE population norm). 33
HSE, Health Survey for England; RL, role limitations; SF-36, 36-Item Short Form Health Survey.
EQ-5D data
There were no statistically significant differences in the t-test values for EQ-5D Euroqol (p = 0.91) and EQ-5D Health State (p = 0.91) between participants with and without CO (Supplementary Table S3).
SF-36 data
There were no statistically significant differences in each of the nine sections of the SF-36 data between participants with and without CO: physical functioning (p = 0.25), RL due to physical health (p = 0.99), RL due to emotional problems (p = 0.84), energy/fatigue (p = 0.18), social functioning (p = 0.87), pain (p = 0.90), general health (p = 0.11), and general health (compared with 1 year ago) (p = 0.89) (Supplementary Table S4). However, the t-test value for emotional wellbeing (p = 0.06) was approaching significance and in a larger sample may be significant.
GAD-7 and PHQ-9 data
There were no statistically significant differences between the participants with and without CO for the GAD-7 (p = 0.22) and PHQ-9 (p = 0.61) t-test values, regarding anxiety and depression (Supplementary Table S5). The chi-squared test for PHQ-9 Question 10 (p = 0.36) also indicated no statistically significant difference (Supplementary Table S6).
LYMQOL data
T-tests could not be run on LYMQOL data as the questionnaire was designed to only be completed by participants with CO. Instead, means of the lower limb LYMQOL data were calculated to provide an evaluation of the impact of CO on the participants' function (2.1: medium impact), appearance (2.3: medium), symptoms (1.9: low), mood (1.8: low), and HQoL (5.9: medium) (Supplementary Table S7). The presence of CO impacted the participants in varying levels, from not at all to a lot (1.0–4.0), with the highest impact on function and appearance.
Upper limb data were not analyzed statistically due to low sample size (n = 2). However, the highest impact on HQol for the upper limb was on appearance and mood (means of 2.5 and 2.1 out of 4.0, respectively).
Discussion
Prevalence of CO
This study has confirmed that CO in a bariatric population is common: 52.1% (n = 25 out of 183). However, the corresponding confidence intervals gave a fairly wide 95% confidence that the true prevalence was between 37.4% and 66.7%.
Previously, prevalence studies assessing the prevalence of CO in obese populations included: Inge et al., 24 O'Malley et al., 25 and Fife and Carter 13 with prevalences of 6.2%, 33%, and 74%, respectively. However, these studies have assessment limitations. Inge et al. 24 assessed undefined venous edema, so it is unclear whether this was defined by a physical assessment or participants' symptoms or questionnaire methods. O'Malley et al. 25 relied on participants' symptoms (lower limb skin changes, feeling their lower limbs were swollen, tight or heavy) (Tomás Ahern, personal communication). However, mild CO is not always apparent and cannot be identified by participants consistently, therefore some CO may have been missed. Fife and Carter 13 based their prevalence data from medical records so consistent physical CO assessment cannot be relied upon.
Although the prevalence figure obtained in this study differed from those outlined above, the study followed a clear definition of CO and utilized robust physical assessment methods with the gold standard pitting test and fluid measurement techniques (bioimpedance and tissue dielectric constant).
Severity and impact of CO
The high incidence of participants with CO having histories of cellulitis (n = 10 of 25, six with ISL Stage I edema, and four with ISL Stage II edema) argues the importance of managing CO with early intervention and treatment, to reduce the risk of further episodes of cellulitis. A study by Burian et al. 3 showed that severe stages of edema are associated with cellulitis, but edema controlled by compression reduces the risk of developing cellulitis, with the potential for it not to occur at all.
Most of the 25 participants with CO were able to give a rough estimate of the duration of their CO. However, one participant was not aware of her CO (ISL Stage I, both feet) and another knew about his ankle CO but had not noticed his lower leg CO. This indicates that CO can begin and even spread without people realizing, with the potential to cause immobility and further comorbidities. Furthermore, both of these participants produced low LYMQOL scores in the impact (low, no impact) section, reflecting a good quality of life as shown in the overall QoL (9, 10 out of 10) section. This may imply that the participants who were not aware of their CO, as well as those whose CO did not affect them, were likely to have high QoL scores (as long as they did not associate any bodily pain with the CO).
It should be noted that nine participants with CO were taking diuretics (Bumetanide, Furosemide, Indapamide, and/or Spironolactone), medications sometimes used to treat CO. For the eight participants that completed the LYMQOL questionnaire (the ninth left before the study assessment was completed), the scores indicate a high impact of CO on their lives, demonstrated by each of the sections (function, appearance, symptoms, mood, and overall HQoL). Although commonly prescribed, diuretics are not the best medication for treating CO (or improving the HQoL of participants with CO), unless there are other causes such as heart failure. DLT, including compression bandaging, is the most effective treatment. 4
Only five participants had been told the reason for their CO. This implies that most of the participants (including four out of the six participants with Stage II or III CO) had not been referred to lymphedema clinics. Without proper help or advice in improving their CO, it is likely to grow worse, resulting in cellulitis, immobility, and skin conditions (like chronic lipodermatosclerosis and lymphangiectasia). 4
Lymphedema Quality of Life
This study confirms the high impact on HQoL on bariatric patients, when assessed using the LYMQOL questionnaire, which is sensitive to CO. The highest impact of CO on lower limb HQoL was on function and appearance. This impact is supported by Mercier et al., 37 whose study resulted in similar LYMQOL data, which showed a high impact on the function and appearance of participants who have lower limb edema.
Most participants (n = 19) had mild, pitting ISL Stage I edema, with only six having moderate or severe ISL Stage II or III edema. However, 10 participants with ISL Stage I edema still produced high LYMQOL scores, indicating that their CO had a severe impact on their HQoL. Even among the six participants with ISL Stage II and III edema, the responses were varied. One participant had medium HQoL (6.0) with high function (3.0) and appearance (3.3) impact, medium symptoms (2.4) impact, and low mood (1.8) impact. The second participant left before completing the study assessment, but the other four participants (including the participant with ISL Stage III edema) scored low-impact (1.0–2.0) and high HQoL (8.0–10.0) scores. Their awareness of their CO and their different comorbidities, mobility, and personalities should be taken into account, as multiple factors may contribute to the development of CO and impact HQoL differently.37,38
Causal analysis
All study participants had obesity, which can have a devastating impact on the lymphatic system, leaving the body vulnerable to developing CO. 39 However, heart failure (indicated by high BNP blood test levels), comorbidities, hormones, and medications may also have caused (or intensified) the CO (Tables 3 and 4). Recent research has shown the important relationship between cellulitis, the development of CO and its relationship to a bariatric population. 3
Two participants had high BNP levels (671 and 862 ng/L) when their blood test levels were reviewed as part of their study assessment. Both were still being treated for heart failure, male and female participants, who had a heart attack 9 years before the study assessment and right heart failure 6 months before the study assessment, respectively. Their heart failure would have contributed to their CO. 40
As stated earlier, venous pressure, venous insufficiency, and surgery are known causes for CO occurring in the obese population. 5 This matches the study results as six participants suffered from venous disease: venous flow dysfunction initiating skin changes (like chronic lipodermatosclerosis and hemosiderin staining) and, in severe cases, lymphatic dysfunction. 4 Three participants had histories of having an accident or knee surgery, which can cause trauma and dysfunction to the lymphatic system. 5
Furthermore, obesity leads to less mobility, which leads to less exercise of the calf muscles, causing poor venous circulation, lymphatic return, and CO. 41 Again, this links with the study as 14 participants with CO suffered from upper and lower body immobility.
Among the medications listed in Table 4, more participants with CO took calcium channel blockers and HMG-CoA reductase inhibitors (statins) (both 24%) than those without CO (10.9% and 13%, respectively). Calcium channel blockers are a major group of drugs, prescribed to lower blood pressure. One of their major side effects is that they cause CO by peripheral arteriolar vasodilation. 42 Edema is also known to be a side effect of the statins, Atorvastatin and Simvastatin (0.1%–1% and 1%–10%, respectively). 43
Five out of six participants with ISL Stage II and III edema had mobility limitations, venous disease, and/or were taking CO-contributing medications (calcium channel blockers and HMG-CoA reductase inhibitors). However, one participant with ISL Stage II edema did not appear to have any comorbidities or medications that would have caused/affected the CO. Furthermore, a large number of participants (n = 19) were taking CO-contributing medications but they did not have CO. An article by Moffatt et al. 38 states that many complex factors can contribute to the development of CO. A variety of causative factors can be involved, including heart failure, hypertension, immobility, medications, and even genetic and venous factors.
Lymphedema-associated BMI threshold
Greene et al. 44 performed a study that demonstrated a “lymphedema-associated BMI threshold,” an association between BMI and impaired lymphatic function (resulting in CO). The results of this study are compared with the study results for this article, to test the threshold alongside the study paper BMIs.
Greene et al. 44 assessed 33 obese patients, with a BMI greater than 30 kg/m2, for the presence of lymphedema, using lymphoscintigraphy scans. The group consisted of patients who were at their maximum BMI (had not yet lost weight through bariatric surgery or diet), which is similar to the study article's patients. Abnormal lymphatic function was defined as: the radiolabeled colloid (used in the scan) taking longer than 45 minutes to travel through the lymphatic channels, dermal backflow, and/or the presence of tortuous lymphatic channels with evidence of collateral flow through alternate pathways.
Of the four patients with BMIs between 50 and 60 kg/m2, two had normal and two had abnormal lymphatic function, indicating a BMI threshold at which lymphatic dysfunction begins (Table 6).
Summary of Greene et al. 44 Results
Investigating and comparing the results of both studies is not straightforward. Although 23 participants in our study had BMIs between 40 and 50 kg/m2 and therefore would have had “normal” lymphoscintigrams according to the Greene et al. 44 study, 10 of the study participants had CO (Table 7).
Comparison of Greene et al. 44 and Study Article with Lymphoscintigram Values
The BMI values highlighted by Greene et al. 44 lymphoscintigram results and the results of the study presented in this article were compared. (N = 47, as one participant had a BMI <40 kg/m2).
Greene et al. 44 used qualitative lymphoscintigraphy in their study, which visualizes lymph nodes and vessels. 45 The authors seemed to suggest that having a normal lymphoscintigram result meant that the participants did not have CO. However, patients can have CO with a normal lymphoscintigram. 45 Venous hypertension leads to increased lymph flow until the maximum capacity is reached. If capillary filtration exceeds lymphatic drainage, CO develops even if lymphatic drainage is increased above baseline levels (high output failure of the lymphatic system). In fact, this is theoretically the stage when the edema could be reversible. If high output failure persists, the lymphatics become damaged resulting in irreversible CO (lymphedema). 38
Comparing the BMIs of Greene et al. 44 and this study article, both sets of participants were obese with high BMI ranges (30–83.3 kg/m2 BMI and 37.2–66.9 kg/m2 BMI, respectively). However, the study populations had different thresholds for CO occurring. Not only did the study article participants have CO in the ‘Normal’ BMI range (Table 7), but half of the participants in the ‘Abnormal’ range did not have CO. One explanation could be that other factors, such as comorbidities and medications, can contribute to the production of edema and may alter the apparent BMI threshold. 38
Impact on quality of life
As presented in Table 5, most of the study SF-36 questionnaire scores were lower than the HSE population normality scores, highlighting that the bariatric patients had a poor HQoL compared with the normal population. Even within the constraints of a small sample size, the participants' HQoL was low, impacting each area of life (physical, energy, and pain), including psychosocial health (emotional and social). This shows the big impact of morbid obesity on HQoL, vastly different from the normative population. 10
The HQoL of participants with CO was not significantly different from participants without CO. One explanation is the mild nature of the CO (n = 19 out of 25). The participants' HQoL was already impacted by morbid obesity, immobility, and comorbidities (like diabetes and heart disease), so their CO did not greatly affect their HQoL. Although the impact of CO could not be realized in this study, other studies have demonstrated that those living with CO experience a poor HQoL, especially regarding appearance and symptoms in the upper limb CO, and function and appearance in the lower limb CO. An increased level of CO leads to an increased impact on HQoL.37,46
Managing the CO of bariatric patients is always complex and challenging. Obesity impacts significantly on treatment, as using traditional methods like DLT are not effective long term.47,48 A study by Morgan et al. 47 demonstrated that professionals always struggle to know how to treat these patients and have to adapt traditional treatments to battle with limb distortion and complex comorbidities. The patients are associated with complex presentations of CO, which result in longer treatment episodes and poor outcomes. This impacts on their quality of life, particularly their psychosocial health and social life.
Comparison of populations
Keeley et al. 7 performed a study that provided the profile of patients from specialist lymphedema services in the United Kingdom, France, Italy, and Turkey. Table 8 compares the United Kingdom lymphedema service population from Keeley et al. 7 with the bariatric population recruited to this study.
Comparison of United Kingdom Lymphedema Population with Study Bariatric Population
Comparison between United Kingdom LIMPRINT patients (with completed ISL scale) and Study CO patients. All patients were classified as having morbid obesity.
Bold: significant difference.
CI, confidence interval; ISL, International Society of Lymphology; LIMPRINT, Lymphedema IMpact and PRevalence INTernational.
Although both populations had a comparable level of obesity (morbid obesity), the bariatric population were younger (p value: <0.001) and had significantly different ISL stages (p value: <0.001). The lymphedema service population had greater ISL Stages II and III (n = 53 and 16), compared to the bariatric population with greater ISL Stage I (n = 19). Furthermore, the left Stemmers sign was significantly different (p value: <0.001) and the right Stemmers sign almost significant (p value: 0.069). For left and right sides, the lymphedema service population had a greater number of positive than negative Stemmers signs and the bariatric population more negative than positive. This corresponds with the lymphedema service population consisting of patients with more severe CO (ISL Stages II and III).
This comparison highlights the different levels of CO severity in the lymphedema service and bariatric populations. Although both were morbidly obese, the bariatric population had a milder CO, indicating that having a high BMI does not necessarily mean a greater severity of CO. It is unclear why these populations were different. As they had similar BMIs, the CO severity was expected to be similar. However, the comparison has shown that the lymphedema services see morbidly obese patients with severe CO and the bariatric service sees morbidly obese patients with mild CO.
Identification of CO among morbidly obese patients needs to be integrated into clinical assessments. Early recognition by weight management programs and management by intervention (compression, DLT, self-care) may alleviate the CO and prevent it from progressing to the more severe, ‘difficult-to-treat’ stages that lymphedema services often see. 4
Study limitations
Recruitment in this study was challenging due to the following: assessment length, busy bariatric clinic schedule, and clinic structure. Of the 183 patients, 30 patients declined. Reasons included: patient was in pain and needed to leave, and time issues. For seven other participants, the researcher and bariatric team made management decisions on the clinic day not to ask them to take part in the study. Reasons included: the patients being in pain, stressed, or immobile. A large number of patients (n = 68) were not recruited due to the following reasons: they were not approached due to the busy clinic, the patients could not wait for the length of the assessment, or the researcher was unavailable to assess them.
The small sample size (n = 48) means that caution should be given when generalizing the results. Roughly eight new patients attended the clinic each week, but only two to three patients were recruited per week, depending on clinic schedule organization and the number of new patients. Patients that were likely to consent to take part in the study were those who did not need to leave quickly (no work that day, no concern of car parking costs).
Conclusion
This study was established to determine the prevalence and impact of CO on the HQoL of a population of bariatric patients. Although this complex population was challenging to study, a high prevalence of CO was highlighted in the bariatric service. The participants' HQoL was impacted in varying degrees by the CO, with most participants having mild pitting CO. The major impact on CO was obesity, immobility, and calcium channel blocker medications. The SF-36 study data highlighted the low HQoL of the participants, indicating the big impact of morbid obesity on HQoL.
Even though most CO was mild, over 50% of study participants had CO. This points to an unrecognized problem in the bariatric service. Identification needs to be integrated into the bariatric assessment to prevent any CO from becoming unnecessarily worse. Managing CO early also reduces the risk of developing cellulitis. It is imperative that clinical staff are trained in how common CO and associated skin conditions are in obese patients and that they are treatable. They need to recognize the preventable impact that immobility, medication, and obesity can have on the lymphatic system. Furthermore, in lymphedema services, patients with a high BMI end up having severe CO. It is important to discover why lymphedema and bariatric service populations have different CO severity, even though they have common BMIs.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank the following: (1) All participants who took the time to contribute to the study. (2) The Lymphedema and Bariatric teams at the Royal Derby Hospital for their support. (3) Peter J. Franks for his wonderful statistical help and advice. (4) The University of Nottingham for sponsoring the study.
Author Disclosure Statement
Amy Newman and Christine J. Moffatt—The study was supported by the registered charity International Lymphoedema Framework (ILF).
Iskandar Idris—Received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from: Astra Zenica, Eli Lilly, Novo Nordisk and Boehringer.
Funding Information
The study was funded by the registered charity International Lymphedema Framework.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.