
Abstract
Abstract
Various techniques are available for measuring the status of lymphedema. A modified imaging technique using ultrasonography was developed to measure the structure of soft tissue area in a cost-effective manner. The purpose of this study was to measure the reliability and the accuracy of this new method. Ultrasonography was performed on both arms of twenty healthy female participants. At 10 cm above (AE) and below (BE) the elbow crease, soft tissue thickness at medial, lateral, inferior, and superior locations were measured by two examiners with minimal unnecessary pressure. After measuring twice on 16 sites for each participant, the amount of soft tissue in the cross-sectional area (ΔCSA) was acquired by a designed formulation. The ΔCSA was also compared with volumetry data (Perometer®). Cronbach's alpha coefficient test was used for statistics. The intra-class and inter-class reliability measurements for all soft tissue areas were very strong (α=0.980 and 0.960, respectively; p<0.01). All AE and BE reliabilities showed very strong correlation and strong correlation of inter-BE measurement. All reliabilities of ΔCSA were very strong (≥0.950). All CCs (correlation coefficients) between ΔCSA, circumference, and volumetry were strong for AE and BE measurements, except for ΔCSA and circumference at BE. The strongest CC was between volumetry and circumference measurements. This study suggests that measuring the ΔCSA by ultrasonography could be an alternative way to measure the status of soft tissue indirectly with structural consideration.
Introduction
L
To measure improvement of lymphedema after treatment, various techniques have been tested, including volume and structural measurements.17–23 In the clinic, arm circumference measurement is the most popular; however, it cannot evaluate structural changes in the subcutaneous tissues, and technical errors can be made by uncontrolled tape measurement pressure, inaccurately marked points, or an improper angle relative to the long axis of the limb.17,24
Another method of volume measure is volumetry using either water or an infrared light beam.232,24 Although this method can measure the volume automatically, it is unable to identify structural changes in tissues because it measures the whole limb (including lymphedema, muscle, bone, and other soft tissues). In addition, it is also time-consuming and is not suitable for assessing restricted joint movement.17,24,26 All volume measurement methods can also be affected by changes in body weight.
For measuring the structure and volume of subcutaneous tissues, image analysis by magnetic resonance imaging (MRI) and computed tomography (CT) have been applied.24,27–29 These methods can measure the amount of lymphedema more precisely by calculating the cross-sectional area of the lymphedema at a localized area. However, the cost is high, and patients may be exposed to excessive radiation if applied repeatedly. Recently, dual energy x-ray absorptiometry and bioelectrical impedance spectroscopy was used for the measurement of lymphedema.18,19 However, the systemic method with calculated data may not reflect the real body composition of the specific part of the body.
Ultrasonography is commonly used because of its simplicity.2,3,4,16,26,30 Lymphedema volume can be measured by the soft tissue thickness at a localized area by ultrasonography, and the thickness of the tissue components (including fluid collections) can be measured at the examined area. However, this method only measures the thickness of lymphedema at the examined areas; thickness changes at other areas cannot be determined, and the total amount of lymphedema is not measurable.
Recently, Kim et al. 16 reported a new measurement method for lymphedema. By measuring soft tissue compliance with pressure, the authors evaluated the structural and softness changes of the soft tissues in healthy participants. This could be a good method for the measurement of structural changes in soft tissue by pressure compression. Although measuring tissue softness is also an important factor in the evaluation of improvement of lymphedema following treatment, it is difficult to show the real volume change of the lymphedema, and results can be variable when tested in lymphedema patients. Unlike in healthy young patients, the affected limbs can be thicker and softer. Therefore, these findings are affected to a greater degree by the practitioner and pressure.
Consequently, a modified imaging technique was adapted to measure the soft tissue volume and structure in a cost-effective manner. In this study, the authors describe a new measurement method using ultrasonography in a cross-sectional view, which is theoretically capable of showing the status of soft tissue separately from the other structures (such as bone and muscle). Since our method measures the soft tissue directly, it may be ideal for volume measurement in lymphedema patients. However, our method could not measure the exact whole volume of soft tissue and can only measure the two-dimensional soft tissue amount in cross sectional area. Theoretically, it could reflect the status of soft tissue volume indirectly.
The aim of this study is to determine if the new volume measurement technique is a reliable method for assessing upper extremity subcutaneous soft tissue in healthy participants. In order to test the robustness of this method, measurements were also made using the conventional method, and the outcomes of the two methods were correlated for linearity.
Materials and Methods
Subjects
Twenty healthy female volunteers were recruited for the study. All participants had no infections or other musculoskeletal diseases of the upper extremities. Informed consent was obtained from all participants prior to the study. The Samsung Medical Center Department of Health Institutional Review Board approved this study.
Ultrasonography measurement
Ultrasonography was performed on both arms of each participant. The participants were placed on a bed with the arm extended. At 10 cm above and below the elbow crease, the superior (a), medial (b), inferior (c), and lateral (d) directions were marked to measure the desired cross-section (Fig. 1). The circumferences at 10 cm above and below the elbow crease were measured with measuring tape. Care was taken not to apply excessive pressure during circumference measurement. The amount of soft tissue was measured using a 7.5 MHz transducer (Sonoline G50®, Siemens Medical Solutions, USA). A large quantity of ultrasound gel was applied liberally on the skin, and the probe was placed transversely on the target areas. Minimal pressure was applied to reduce the pressure discrepancy made on the tissue by the two examiners. The thickness of the soft tissue was measured as the distance between the skin and the fascia of the muscle. When the examiner asked the participants to move the elbow or wrist joint, the mobile structures were considered to be muscle, and the fascia could be separated from the muscle layers.
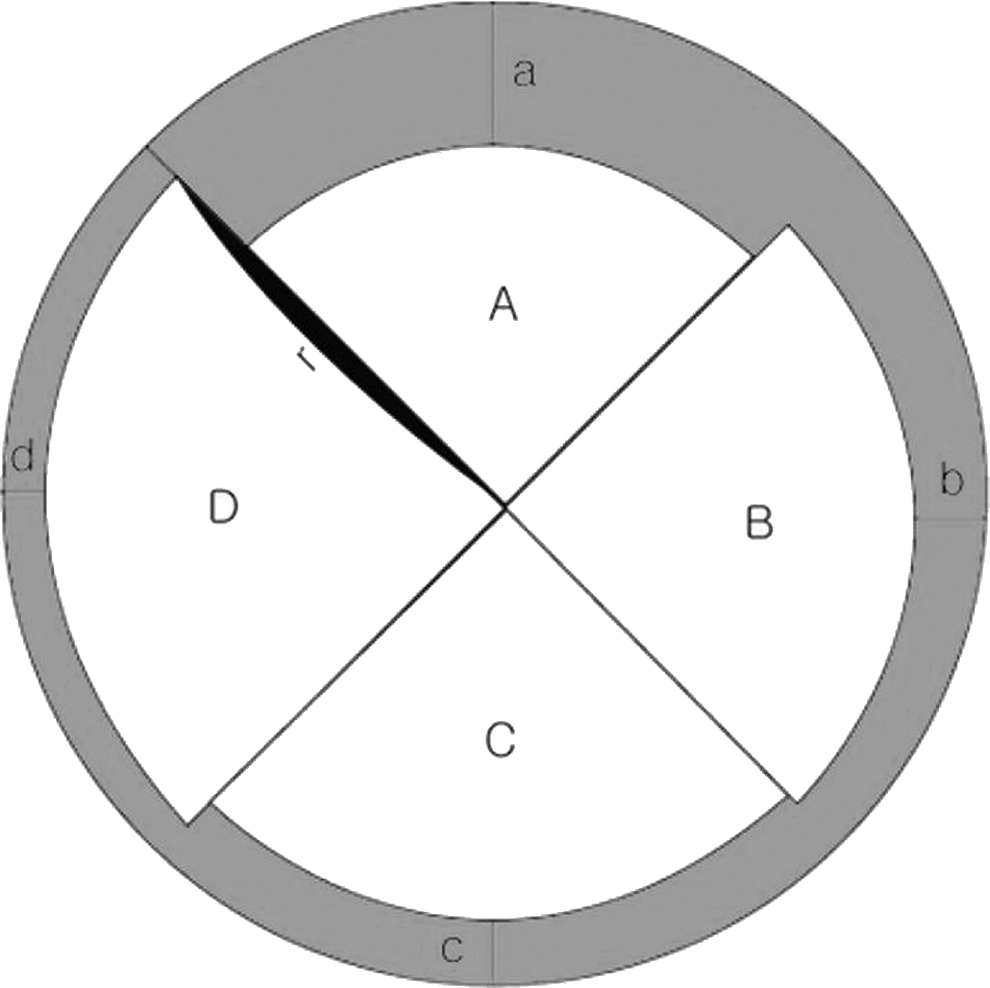
Ultrasonographic measurements at 10 cm above and below the elbow crease (
A total of 16 areas from above and below the elbow on both arms were examined on each participant. At each location, the radius of the quarter area of the soft tissue was measured (Fig. 1a–d), and circumferences were recorded (y in Fig. 1). Using the measured circumference of the examined area, the total cross-sectional area could be acquired; by measuring the distances (Fig. 1a–d), the imaginary inner area (Fig. 1A–D) of the cross-section could be calculated using the following formulation. By subtracting the inner area out from the total cross-sectional area, the ΔCSA (Δ cross-sectional area of the soft tissue) is calculated.
Formulation
Circumference (Y)=2 πr
Measurement of depth (two times by each examiner): a, b, c, d at four locations on the limb at 10 cm above and below the elbow crease
Therefore, the equation can be formulated as:
The eight areas from above and below the elbow crease were examined by two examiners. Measurements were taken twice by each examiner to determine intra-rater variation.
Volumetry (Perometer)
The perometer is an optoelectronic device consisting of a square measuring frame positioned on a rail that can be moved along the long axis of the extremity to be measured.
The participant was seated in an adjustable chair with the arm to be measured positioned centrally within the measuring frame. The measuring frame was then manually moved along the rail along the length of the arm from the original starting point at the finger towards the upper arm, then returned to the original starting point. As the frame passes over the arm, the limb interrupts the paths of the optoelectronic beams. The diameter of the limb was determined by the number of light diodes obstructed by the limb. 24 In this study, we measured the volume from 10 cm below the elbow crease to 10 cm above the elbow crease.
Data analysis
All statistical analyses were performed with SPSS/PC+software version 17.0 (SPSS Inc., Chicago, IL, USA). The intra- and inter-rater reliabilities were determined using intraclass correlation coefficients (ICCs) with 95% confidence intervals. Cronbach alpha coefficients were calculated between the circumference with tape and the measurement made with ultrasonography.
Results
Demographic data
Twenty healthy participants were recruited for this study. A total of 40 upper extremities were examined with tape measurement, volumetry, and ultrasonography. The demographic data of the participants were shown in Table 1.
Intra-rater and inter-rater reliabilities
Intra-rater reliability
The total reliability at all soft tissue locations was very strong for both intra-rater (r=0.980) and inter-rater (α=0.960) measurements (p<0.01). There was no significant difference in reliability between the AE and BE measurements for intra-rater measurement (0.966 and 0.931, respectively). For both AE and BE, the reliability at c was the lowest (0.905 and 0.906, respectively). The reliability of ΔCSA was also very high at both AE and BE (0.981 and 0.956, respectively) (Table 2).
Inter-rater reliability
The total inter-rater reliability was also very strong (0.960). The value at BE was slightly lower (0.876) than the AE measurement (0.939). The lowest reliability was noted at point d for AE and c for BE (0.734 and 0.811, respectively). The reliability of ΔCSA was very strong for AE and BE measurements (0.969 and 0.950, respectively) (Table 2).
Correlation coefficients
The correlation coefficients between
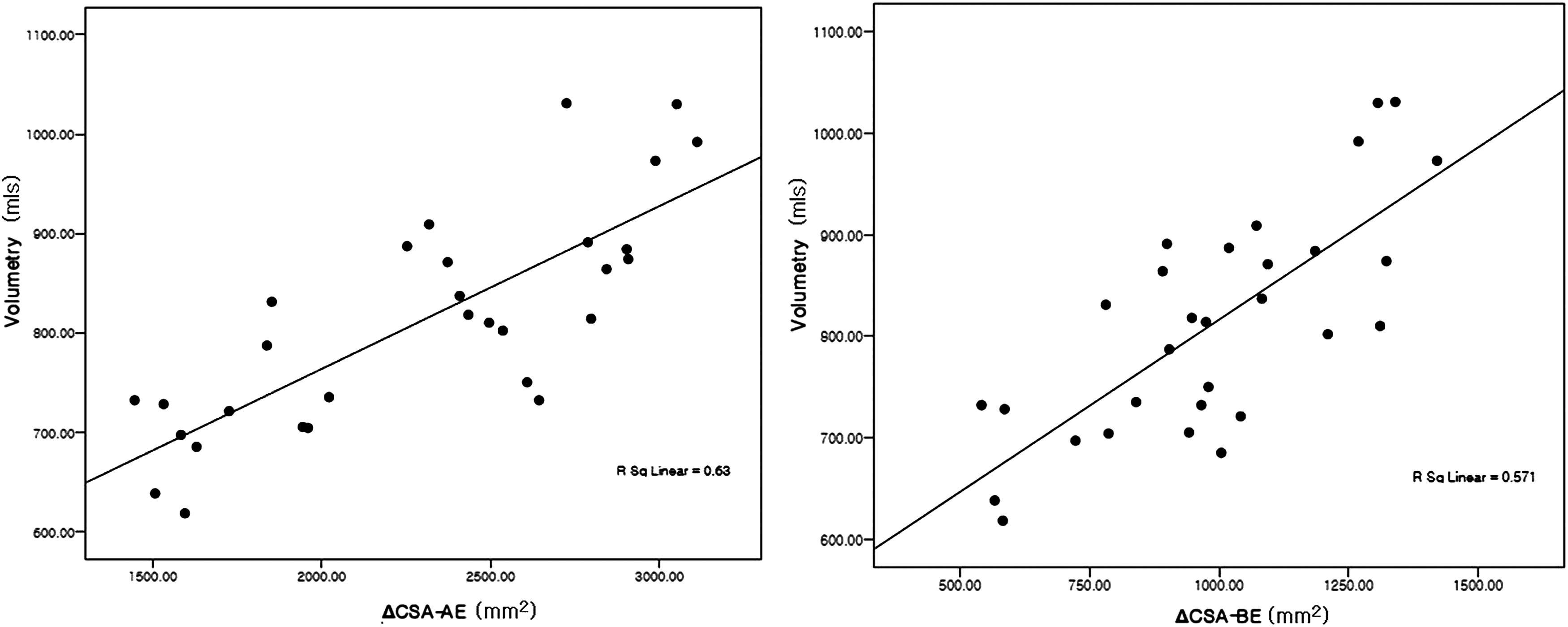
The correlation between ΔCSA (AE and BE) and volumetry has strong statistical significance.
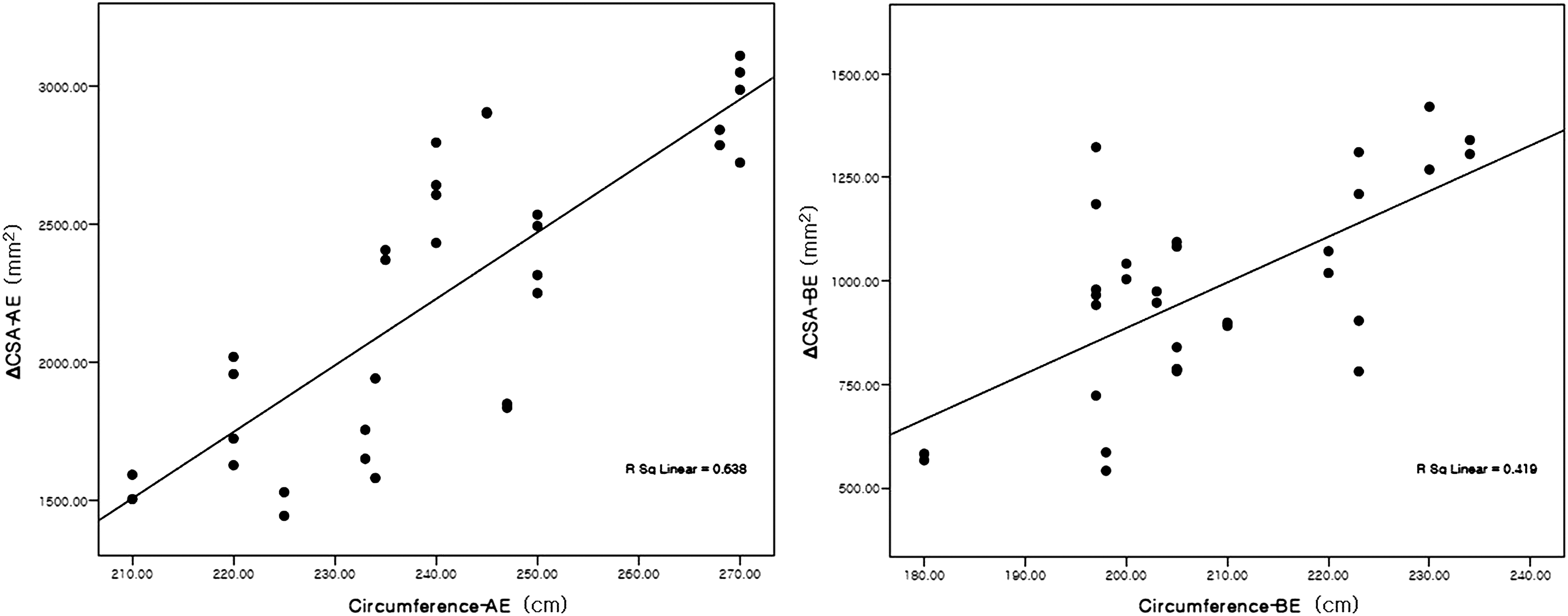
The correlation between ΔCSA (AE and BE) and circumference has strong statistical significance for AE and moderate for BE.
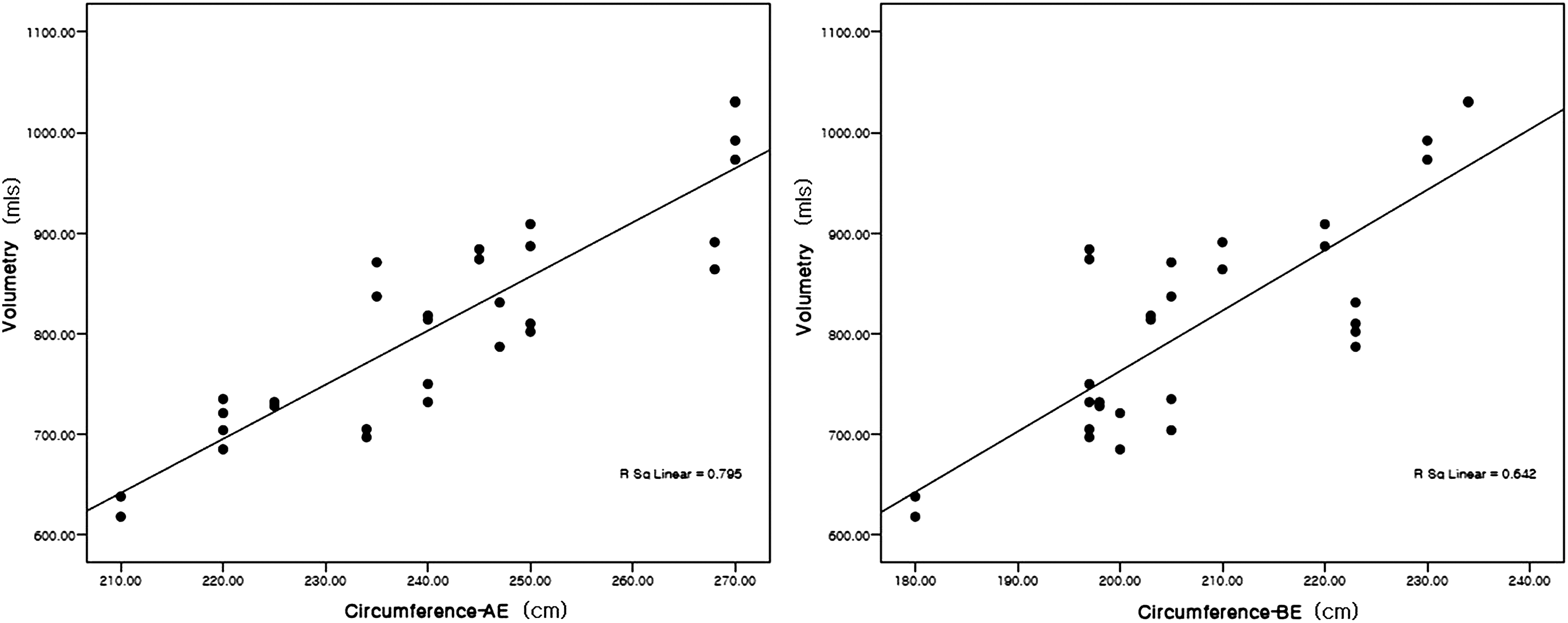
The correlation between volumetry (AE and BE) and circumference has strong statistical significance at both AE and BE.
Discussion
There have been several trials that have attempted to measure the real amount of lymphedema in cancer patients and primary lymphedema patients.4,6,7 Arm circumference measurement using a tape measure is the most commonly used method in the clinic, while volumetry is another objective measurement option. CT and MRI may be ideal tools for measurement and identification of soft tissue structural changes; however, due to cost ineffectiveness and inconvenience, MRI and CT are not commonly available in clinics.
The compliance study of Kim et al. 16 could be conveniently used in clinics. However, this method can only measure the compliance at a localized area and cannot evaluate structural changes in the subcutaneous tissues or whole volumes.
In this study, we have developed a new ultrasound-based method for the measurement of the structural volume of soft tissue. Because ultrasonography is safe, easy to use, and inexpensive, our new method may be a good alternative way to measure the status of soft tissue indirectly. Since we could not measure the whole amount of volume directly, it still could not reflect the real volume of the limb.
In our results, both intra-rater and inter-rater reliabilities of soft tissue thickness measurements were very strong. Intra-class measurements of c at AE and BE had relatively low reliability, but still showed strong reliability overall (0.905 and 0.906, respectively) (Table 2). Possible explanations for the low value at c include the thick soft tissue in this area and position change during examination (shoulder forward flexion in AE and elbow flexion in BE). During position change by examiners, the original position (neutral position of shoulder and elbow) changed, and the relative difficulty in probe application position may result in some differences. Measurements at locations d for AE and c for BE showed the lowest inter-rater reliability value. Generally, the reliabilities of the BE were lower value than those of AE; this may be due to relatively closer distance from skin to the outer fascia at BE measurements.
Overall, these findings demonstrate strong reliability if the measurement is performed by the same examiner at the same anatomic area, which suggests that this method could be an ideal for measurements of the amount of soft tissue. However, more consideration will be needed to reduce the technical inter-examiner error when measuring at BE.
The correlation coefficients of the new technique with volumetry and circumference measurements were strong. However, they were lower than the correlation coefficient between volumetry and circumference measurement. This is possibly due to the fact that our new technique can measure the volume with consideration of structure, while the two other methods cannot evaluate the real structure of the soft tissue. Because of the different proportions of soft tissue of each participant, the data for each participant could be different. Therefore, the correlation between simple measurement tools without structural consideration was stronger than the correlations involving ΔCSA.
There are several advantages to our CSA measurements. First, our method correctly tells the real component of the volume by measuring the area of the examined cross-section. Second, because ultrasonography is used, the measurements are safe and can be repeatedly used with relatively less time. Third, observations of structural changes and dynamic evaluation are possible while measuring the volume change. Fourth, it costs less than other expensive methods capable of measuring structural changes in cross-sections, such as CT and MRI.
However, there are also some disadvantages to our new method. First, like other measurements using ultrasonography, our method may be relatively subjective. Therefore, even if there is strong correlation between examiners, there could be sources of measurement variability (including pressure control and use of the same anatomical measuring point). In particular, in an area in which there is lymphedema, the examiner should be careful to apply the same pressure for exact measurement in a series of studies. In this study, we measured the soft tissue cross-sectional area in healthy participants. However, the characteristics of soft tissue in lymphedema patients may differ from those of a healthy participant, and tissue compliance may be more pressure-dependent than with healthy soft tissue. Second, ultrasonography measurements require more time, as compared to methods, such as tape measurement and volumetry. Multiple probe applications with dynamic muscle action tests should be used for better distinction of lymphedema from muscle when applied to lymphedema patients. Third, if the lesion is too thick as the case of lymphedema, the thickness of the soft tissue cannot be acquired. Due to resolution limitations, if the thickness exceeded more than 4 cm using our equipment, the thickness could not be measured. Fourth, swelling occurring on a joint area (such as the ankle, elbow, or wrist) is difficult to measure. Areas surfacing the bone will differ from areas for which all sides are surrounded by edema. Fifth, the local assessment may not be representative of all the lymphedematous change.
However, despite these disadvantages, our newly invented ultrasonographic method could be an alternative way to measure the status of soft tissue indirectly with structural consideration.
Conclusion
This study suggests that measuring the ΔCSA by ultrasonography could be an alternative way to measure the status of soft tissue indirectly with structural consideration.
Author Disclosure Statement
The authors declared no conflict of interest.
This study was supported by a 2012 research grant from Pusan National University Yangsan Hospital.