
Abstract
Aim:
The aim of this study was to assess the efficacy of the snare traction technique in assisting the endoscopic resection (ER) procedure in gastric submucosal tumors (SMTs) ≥ 2 cm.
Methods:
Between January 2015 and December 2022, we retrospectively reviewed data from patients with gastric SMTs ≥ 2 cm who were treated by ER at the first affiliated hospital of Zhengzhou University. Then, propensity score matching (PSM) (1:3) between snare traction–assisted and conventional ER procedures was used to overcome selection bias. The success rate, en bloc resection rate, dissection time, dissection speed, and perioperative complications were compared.
Results:
A total of 314 patients were included in this study. After PSM, 34 patients were enrolled in the snare traction-assisted endoscopic resection group (STAER) and 102 patients were enrolled in the conventional endoscopic resection group (CER). STAER group had a higher dissection speed (6.60 vs. 5.20 mm2/min; P = .030) and shorter dissection time (76.00 vs. 76.50 minutes, P = .003). There were no significant differences in technique success rate, en bloc resection rate, and perioperative complications between the two groups. In subgroup analysis, the dissection speed of STAER was significantly higher than that of CER when the lesion length was 2–5 cm, underwent endoscopic full-thickness resection, and was located in the gastric antrum.
Conclusions:
STAER demonstrated a higher efficiency for gastric SMTs ≥ 2 cm, without increasing the perioperative complications. Further prospective studies are needed to assess the efficiency and safety of the STAER method.
Introduction
Endoscopic resection (ER) technique achieved considerable progress, including endoscopic submucosal dissection (ESD), endoscopic submucosal excavation (ESE), and endoscopic full-thickness resection (EFTR), which provide minimal invasiveness and effective outcomes in patients with gastric submucosal tumors (SMTs).1–4 Several studies have demonstrated that ER for relatively small gastric SMTs was safe, effective, and quick.5,6 However, the application of ER in clinical practice was limited by the complexity of operation, especially in difficult-to-access locations or relatively large lesions.
Several traction techniques have been developed to overcome these difficulties. 7 Moderate tension was applied in the submucosal layer of the tumor, allowing easier identification of the dissection plane and blood vessels. Thus, traction could increase the resection speed, shorten operation time, and reduce perioperative complications. The dental floss with clip method was common and easy to perform in assisting ER.8,9 However, this method can only achieve single-way traction toward the oral side. In addition, dental floss is extremely thin resulting in poor controllability. Other traction methods, such as the S-O clip or magnetic method, could facilitate dissection effectively, but they either require additional maneuvers or costly adjunct devices, which are not available in some hospitals. 10
Snare applied in traction is worth exploring because it is a commonly used endoscopic accessory and is easier to master. Snare traction could achieve double-way traction of pushing and pulling. In this study, the effectiveness and safety of a snare traction-assisted endoscopic resection (STAER) group were compared with conventional endoscopic resection group (CER) through a propensity score matching (PSM) analysis.
Methods
Patients
From January 2015 to December 2022, we collected and reviewed data from patients with gastric SMTs, which were treated by ER at the first affiliated hospital of Zhengzhou University (Fig. 1). Endoscopic ultrasonography (EUS) and/or computed tomography (CT) were used to assess the tumors prior to ER.
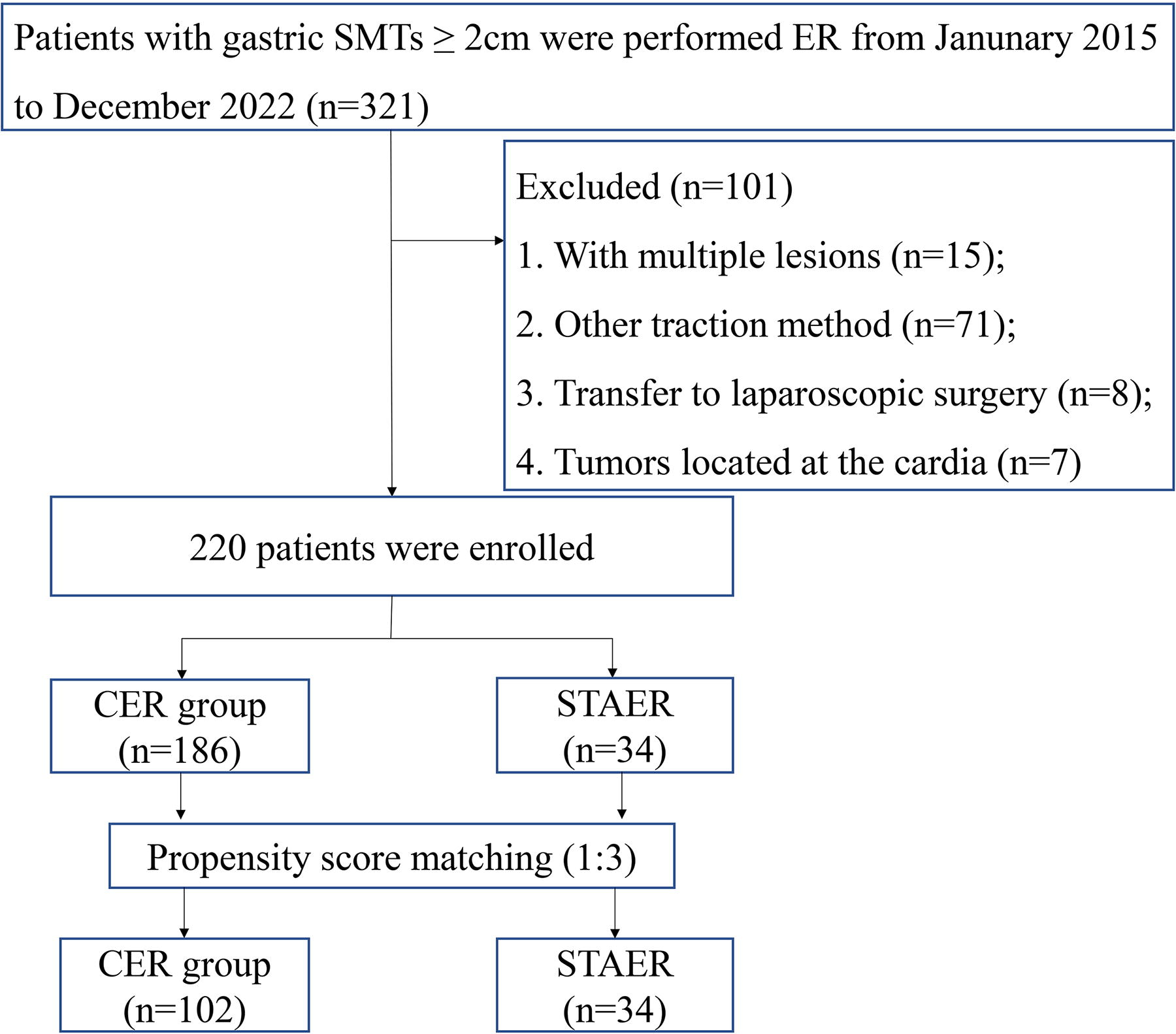
Flowchart of enrolled patients.
The inclusion criteria were as follows: (1) gastric SMTs were detected by EUS or CT and did not show metastasis; (2) tumor size ≥ 2 cm; (3) patients were willing to undergo tumor resection by ER. Exclusion criteria included the following: (1) patients with multiple lesions; (2) patients who underwent ER with other traction methods; (3) patients who were transferred to laparoscopic surgery; (4) tumors located at the cardia. Patients who underwent ER with snare traction were classified into STAER group, while those without any additional traction assistance were classified into a CER group (Figs. 2 and 3). Informed consent was obtained from all patients prior to the ER operation. This study was conducted in accordance with the ethical standards of the Helsinki Declaration of 1975 and was approved by the institutional review board of the first affiliated hospital of Zhengzhou University.
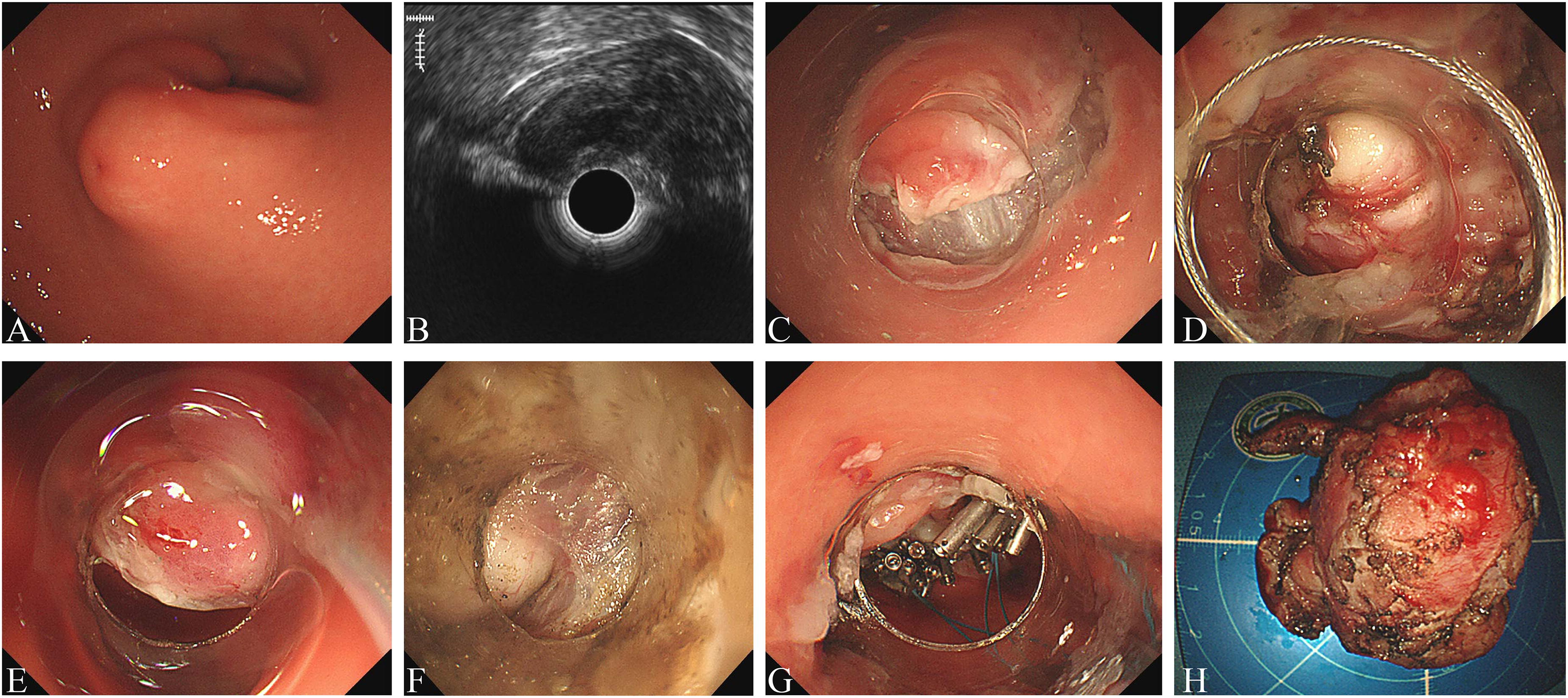
Snare traction-assisted endoscopic resection procedure.
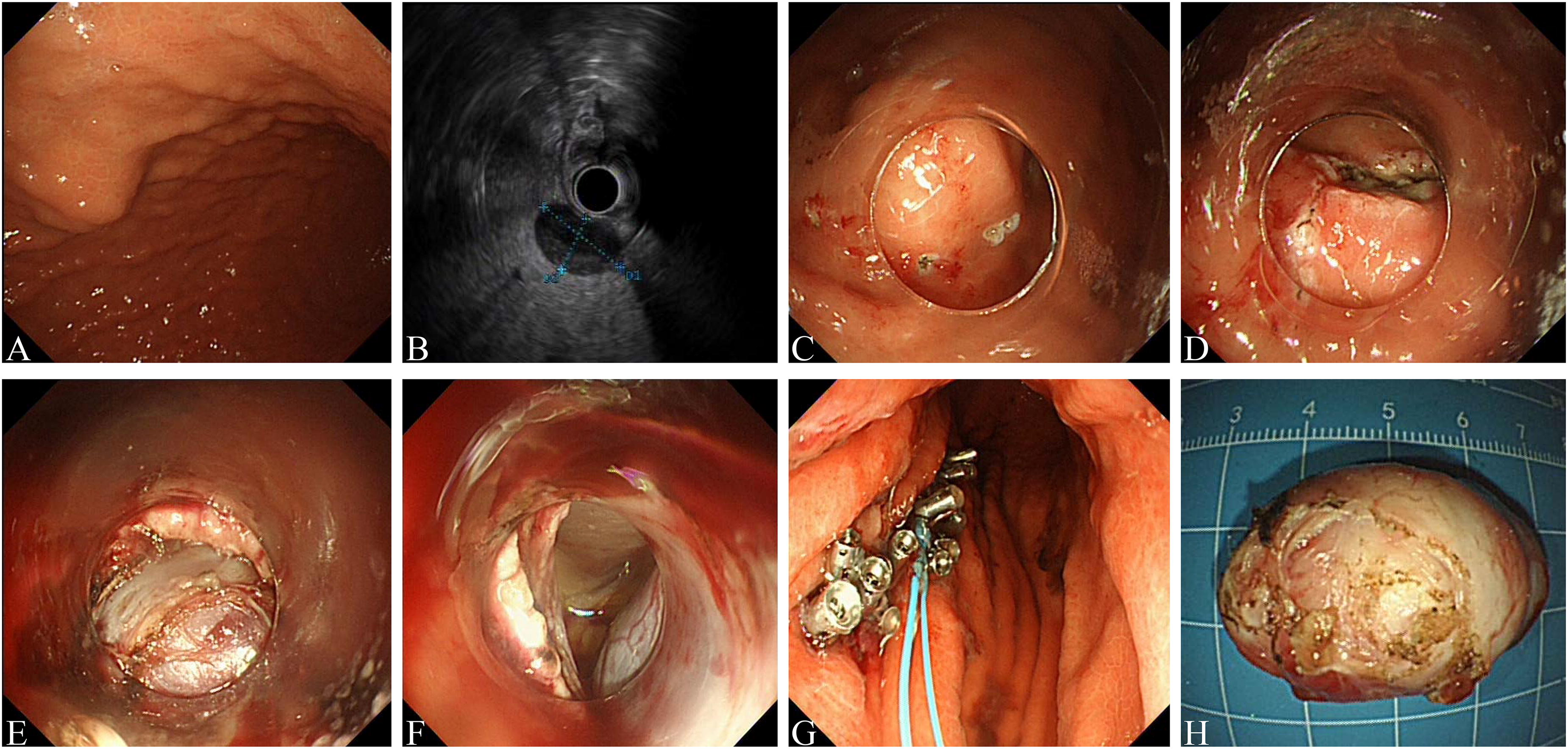
Conventional endoscopic resection procedure.
Previous studies have reported tumor size and location were the major factors affecting the operation time and difficulty. 11 Therefore, PSM was conducted to balance the potential confounders. Tumor location, length and width, operation technique, and pathology were identified as potential confounders. Then, the subjects in the STAER group and CER group were matched at a 1:3 ratio based on the propensity value. Only patients matched with PSM were included in the subsequent analysis. The matching was optimal in the sense that the sum of the absolute pairwise distances in the matched sample was as small as possible.
Snare traction-assisted endoscopic resection procedure
All patients received general anesthesia with airway intubation. Conventional ESD, ESE, and EFR were described as previously reported. For snare traction procedure, the endoscope with a transparent cap and a snare attached was introduced into the stomach. The tumor was grasped with/without the help of biopsy forceps and the snare was released to ligate the tumor. The anchoring sites were determined according to the endoscopists.
Definitions
The dissection time was defined as from marking the tumor to the end of tumor removal. The tumor area was calculated using the following formula: area (mm2) = [smaller diameter (mm)/2] × [larger diameter (mm)/2] × π. Dissection speed (DS) was referred to the area of the resected specimen divided by dissection time (mm2/min). En bloc resection was referred to the removal of the whole tumor in a single piece. Among them, after the en bloc resection of the tumor, some tumors are too large to be removed through the esophagus, thus we resected part of the tumor for subsequent histopathological examination. Intraoperative bleeding was defined as that cannot be controlled by ER procedure. Delayed bleeding was referred to clinical evidence of bleeding, requiring blood transfusion or endoscopic or surgical intervention. The complication of perforation did not include the intentional perforation caused by EFTR.
Statistical analysis
Continuous variables were expressed as median (interquartile). Categorical variables were shown as frequencies and percentages. The continuous data were compared by the Wilcoxon rank-sum test or the Student’s t-test, and the categorical data were compared by the chi-squared test or Fisher’s exact test. P < 0.05 was considered statistically significant. All analyses were performed by SPSS26.0 (IBM Corp., Armonk, NY, USA).
Results
As showed in Figure 1, a total of 220 gastric SMTs were enrolled in this study. The STAER and CER group differed with respect to the pathology type and location of the tumor. In order to mitigate confounding, patients were matched at a 1:3 ratio through PSM analysis, resulting in 34 in the STAER group and 102 in the CER group.
Baseline characteristics before and after PSM
Before PSM, there were significant differences in the tumor location and pathology type between the two groups (Table 1). After PSM, baseline characteristics and operation-related variables were balanced between the two groups.
Baseline Characteristics of Patients with Gastric SMT ≥ 2 cm Before and After PSM
CER, conventional endoscopic resection; EFTR, endoscopic full-thickness resection; ESD, endoscopic submucosal dissection; ESE, endoscopic submucosal excavation; GIST, gastrointestinal stromal tumor; PSM, propensity score matching; SMT, submucosal tumor; STAER, snare traction-assisted endoscopic resection.
Bold values indicate that their p-values are less than 0.05, which is statistically significant.
Treatment outcomes before and after PSM
Before PSM, the STAER group had a shorter dissection time (P = .003), fasting time (P = .001), and postoperative hospital stays (P < 0.001). However, no significant difference was found in the results of technique success rate, en bloc resection rate, tumor area, dissection speed, and complications (Table 2).
Endoscopic Treatment Outcomes of Patients with Gastric SMT ≥ 2 cm Before and After PSM
CER, conventional endoscopic resection; PSM, propensity score matching; SMT, submucosal tumor; STAER, snare traction-assisted endoscopic resection.
After PSM, the STAER group revealed a shorter dissection time (76.00 vs. 76.50 minutes, P = .003), fasting time (3.00 vs. 5.00, P = .004), and postoperative hospital stays (5.50 vs. 7.00, P = 0.003), and higher dissection speed (6.60 vs. 5.20, P = .040). However, there were no significant differences between the two groups in technique success rate, en bloc resection rate, tumor area, and complications.
Subgroup analysis of dissection speed
In the subgroup analyses, the differences of dissection speed were significantly related to tumor length, tumor location, and treatment method (Table 3). For lesions with a length diameter between 2 and 5 cm, the dissection speed was significantly higher in the STAER group than that in the CER group (5.88 vs. 4.91, P = .030). For lesions located in the antrum, the dissection speed was also significantly higher in the STAER group (12.21 vs. 5.52, P = .011). Compared with patients who underwent ESD or ESE, the dissection speed of lesions performed by EFTR was also higher in the STAER group than that in the CER group (6.24 vs. 5.48, P = .034).
Subgroups Analysis of Dissection Speed
CER, conventional endoscopic resection; EFTR, endoscopic full-thickness resection; ESD, endoscopic submucosal dissection; EP, ectopic pancreas; ESE, endoscopic submucosal excavation; GIST, gastrointestinal stromal tumor; STAER, snare traction-assisted endoscopic resection.
Discussion
ER shows an advanced therapeutic technique aiming to provide minimal invasiveness and favorable outcomes in patients with gastric SMTs. However, variations in size and location of the gastric SMTs affect the difficulty of performing ER. Thus, several traction techniques have been developed to overcome these difficulties.12–14 ER with snare traction could potentially reduce the dissection time and dissection difficulty.15,16 And this method didn’t require any additional equipment (only a snare for traction), there was no increase in the total cost of endoscopic accessories for the operation because the snare was used regularly in the ER procedure.
Hu et al. showed snare traction–assisted method is an effective method for ER of upper gastrointestinal SMTs. 16 Our studies concluded similar results. In this study, the dissection time and dissection speed of the STAER group were shorter and faster than that of the CER group, respectively. The technique success rate and en bloc resection rate of both groups are quite satisfactory, which are consistent with previous studies.16,17 There was no difference in complication data between the two groups, which may be owing to the fact that endoscopists involved in this study were experienced in the ER technique.
Although several studies have proved the superiority of traction ER compared with conventional ER,17,18 there were still few studies explored under what conditions could traction method show the greatest effect. Having established that the main advantage of snare traction was a faster dissection speed, we next carried out subgroup analyses to investigate the effect of characteristics related to the tumor. The subgroup analysis of this study revealed that STAER improved the dissection speed in lesions length between 2 and 5 cm, located in the antrum, and lesions was performed by EFTR. In terms of lesion length, we believe that this could be explained by the fact that lesion lengths larger 5 cm were thought to be more challenging for the endoscopists, as the technical difficulty of the operation increases with the size of the tumor. Generally, the location of tumors was an important factor affecting the dissection time of gastric ER. The tumors in the lower third of the stomach were less difficult than the tumors in the upper and middle third. 19 However, this study showed dissection speed was no difference in gastric fundus between the two groups. We supposed the small sample may be a reasonable explanation. Moreover, our study identified EFTR with snare traction could improve the procedure efficiency which was similar to the other studies.
During the endoscopic procedure, traction was used to reduce the difficulties. Previous studies show various traction methods and novel devices have been used to improve the safety and efficiency in ER, including dental floss, S-O clip, or magnetic method.20,21 However, they either require additional maneuvers or costly adjunct devices, which are not available in some hospitals. In this study, snare traction showed unique advantages as follows: (1) cheap, convenience, and practicability; (2) real-time adjustment of the pulling and pushing force; (3) preventing tumors falling into the abdominal cavity during EFTR; (4) traction assistance is often effective at the beginning of ER procedure, but the traction tension gradually reduces during the operation. 22 However, snare traction could change the fixed position flexibly and easily.
This study also has some limitations. First, this was a retrospective study. A PSM analysis was performed to minimize the selection bias. Second, this was a single-center study with a limited sample, which only reflected our center’s experiences. Thus, further multicenter large-sample studies are warranted. Third, the cardia is a special anatomical location with a narrow lumen and frequent contraction. The difficulty increased significantly; therefore, tumors in the cardia were excluded from this study.
In conclusion, ER with snare traction is an alternative choice for the resection of gastric SMTs. Further perspective multicenter large sample studies and cost-effectiveness analyses are required for a more comprehensive assessment of snare traction.
Footnotes
Authors’ Contributions
D.L. and Y.S.: Concept of the study; Y.Z., S.Z., and J.L.: Data collection; Y.Z. and S.Z.: Data analysis; Y.Z. and S.Z.: Statistical analysis. Y.Z., S.Z., and D.L.: Manuscript preparation.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.