
Abstract
Introduction:
Standard-of-care gastroesophageal reflux disease (GERD) procedures are associated with adverse events (AEs) (i.e., dysphagia, gas-bloating). RefluxStop has been developed to circumvent these outcomes. This study presents the results of 28 patients managed with RefluxStop in Germany.
Methods:
Between July 2021 and November 2023, 28 patients with GERD underwent RefluxStop surgery, a novel laparoscopic antireflux procedure. Retrospective chart analysis with patient-informed consent was conducted to determine clinical outcomes, such as GERD Health-Related Quality of Life (GERD-HRQL) score, proton pump inhibitors (PPI) use, symptomatology, patient satisfaction, and perioperative AEs.
Results:
Baseline characteristics (n = 28): age 47 ± 13.1 years; 67.9% female; body mass index (BMI) 27.3 ± 4.1 kg/m2; 93% PPI use for 5.6 ± 2.7 years; and hiatal hernia in 100% of cases of mean (standard deviation [SD]) size 3.4 (0.8) cm, whereof 35.7% were large hiatal hernia (4–6 cm). At a mean (SD) follow-up of 14.1 (4.7) months, patients experienced 88.6% improvement in median (IQR) total GERD-HRQL score from a baseline of 35 (7.7) to 4 (4.2) at follow-up (P < .05). Preoperative dysphagia (35.7%) resolved completely in all patients (P < .001). The mean (SD) GERD-HRQL heartburn subdomain decreased by 90.6% from a baseline of 18.1 (6.1) to 1.7 (1.2) at follow-up and all patients (100%) had scores <5. Similarly, the mean (SD) regurgitation subdomain decreased from a baseline of 13.2 (4.7) to 2 (1.6) at follow-up and all patients (100%) had scores <5. Patient satisfaction was achieved in 96.4% of patients with no PPI use required in 93% of patients (P < .001); only one patient required PPIs for persistent GERD symptoms. No cases of reoperation or esophageal dilatation were performed. Minor intraoperative AEs occurred in seven patients (i.e., neck emphysema).
Conclusion:
RefluxStop provides excellent safety and effectiveness outcomes for GERD treatment. Dysphagia completely resolved (0%) with 88.6% improvement in median GERD-HRQL score and satisfaction achieved in 96.4% of patients. These promising results reproduced the outcomes noted in the RefluxStop CE trial in real-world settings.
Introduction
Typical symptoms of gastroesophageal reflux disease (GERD) include heartburn and regurgitation, with chronic cough, hoarseness, noncardiac chest pain, globus, throat irritation, and sleep disturbance representing atypical symptoms. 1 As a result, reflux disease significantly impairs quality of life. 2 The pathophysiology of GERD involves failure of the antireflux barrier (ARB) which, as delineated by the American Foregut Society in 2022, 3 is constituted by the lower esophageal sphincter (LES), the crus muscles of the diaphragm, and the gastroesophageal flap valve. ARB failure may be appreciated by low basal pressure of the LES and transient LES relaxations, particularly with LES herniation into the chest cavity, resulting in retrograde flow of gastric contents to the proximal alimentary tract (i.e., esophagus, oral cavity). 1
Reflux disease is the most common gastrointestinal disorder worldwide and the age-standardized prevalence with symptoms every day in Germany is approximately 7.3%, 4 with 25%, 14%, and 4% of German adults experiencing mild, moderate, and severe reflux symptoms, respectively. 5 The prevalence of reflux disease in the German population increases with age as demonstrated by 25% of those aged 60–69 years experiencing moderate or severe symptoms. 5 Understandably, the societal costs of GERD in Germany are substantial, particularly when considering that 73%, 61%, and 2% of patients had taken reflux medication, had visited a doctor, or had been hospitalized for GERD in the previous 12 months, respectively. 6 Furthermore, 6% of employed Germans report absenteeism due to reflux disease. 6 As such, an estimated €688 million per year in Germany is lost in gross domestic product due to GERD-associated inability to work, 7 which does not include the direct costs of disease. Approximately 61% of German patients report reduced productivity from reflux symptoms even though 89.5% of these individuals are managed by medical therapy. 7 Optimization of GERD management is likely to provide benefits beyond the patient perspective extending to broader society through improved productivity and diminished burden on the healthcare system.
The management options for GERD include lifestyle modifications, medical therapy predominantly based on proton pump inhibitors (PPIs), and antireflux surgery in selected cases. Lifestyle modifications include dietary modification, restriction of alcohol, avoidance of spicy foods, obesity management, and mitigation of nocturnal symptoms by head elevation. 8 PPI therapy may improve reflux symptoms but carries a substantial rate of irresponsiveness (40%) in some estimates. 9 This is potentially attributable to PPI medication solely reducing the acidity of gastric refluxate without an impact on the frequency of reflux episodes and underlying anatomical and mechanical causes of GERD (i.e., LES basal pressure and transient LES relaxations). 9 For patients experiencing inadequate response with, intolerance to, or not wishing to continue lifelong medical therapy, antireflux surgery is an alternative modality of management. Conventional antireflux procedures include Nissen fundoplication (360°) and partial fundoplication variations; however, they are associated with a significant burden of postoperative adverse events (AEs), such as dysphagia and gas-bloating syndrome, because of distal esophagus encirclement as a mechanism of action. 10 Esophageal encirclement likely overcorrects for the low basal LES pressure as a cause of GERD, as demonstrated by higher LES pressures on manometry in patients with dysphagia, particularly in those with preoperative dysphagia. 11 New technologies have emerged to maintain at least similar or superior efficacy results while minimizing unwanted AEs.
RefluxStop is an implantable device that has emerged in the surgical treatment landscape of GERD. 12 The operative procedure aims to reinstate the ARB through systematic and extensive mediastinal dissection of the esophagus, repair of the diaphragmatic hiatus with hiatal hernia reduction (if necessary), recreation of the gastroesophageal flap valve by esophagogastroplication, and stabilization of newly reconstructed structures in the abdomen with device implantation in the gastric fundus (Fig. 1). The purpose of this study is to present clinical outcomes of 28 chronic GERD patients managed with RefluxStop surgery in Germany.
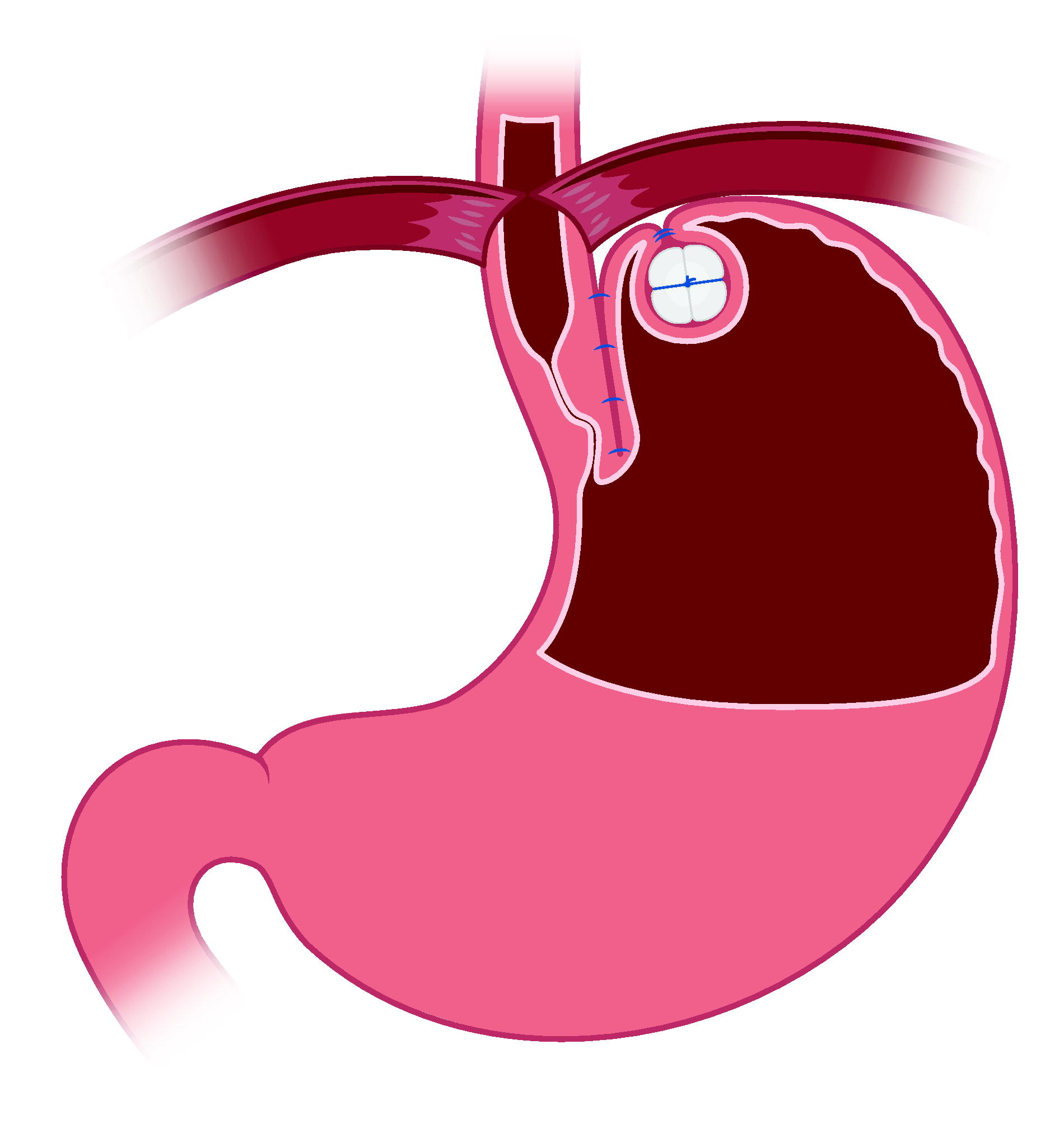
Reconstruction of the ARB with RefluxStop surgery. After diaphragmatic crural repair with hernia reduction (if necessary), esophagogastroplication reinstitutes an acute angle of His to recreate the gastroesophageal flap valve and device implantation in the gastric fundus anchors the LES intraabdominally to sustain basal pressure.* ARB, antireflux barrier; LES, lower esophageal sphincter. *This is an Implantica-provided figure of the RefluxStop device.
Materials and Methods
Study design
Between July 2021 and November 2023, 28 patients with chronic GERD were surgically treated with the RefluxStop device at a single German institution. Based on patient-informed consent, a retrospective chart review was performed to determine clinical outcomes. Inclusion criteria included:
Age ≥18 years. Patients suffering from typical (i.e., heartburn and regurgitation) or atypical (i.e., dysphagia, chest pain, water brash, globus sensation, odynophagia, and extraesophageal symptoms such as chronic cough, hoarseness, and wheezing) symptoms. Proven GERD diagnosis—all patients had endoscopically confirmed GERD (i.e., histologically demonstrated reflux esophagitis). In selected cases, esophageal manometry and barium swallow imaging studies were also conducted. History of inadequate symptom control with antireflux treatment.
Patients were excluded from the study if age <18 years or if they did not provide informed consent for study participation.
Surgical procedure
RefluxStop surgery manages GERD by restoration of the ARB and provides regional stability of reconstructed anatomy. With laparoscopic access, diaphragmatic crural repair with hiatal hernia reduction (if necessary) is performed. Then, free dissection of the esophagus superiorly into the mediastinum is pursued to achieve an additional 4–5 cm of abdominal esophageal length, followed by dissection and mobilization of the fundus to create a tension-free “floppy fundus.” Fat is removed to better appreciate the angle of His and mobilize the LES inferiorly into the abdominal cavity. Sufficient dissection of the esophagus superiorly is critical to ensure an appropriate intraabdominal length of the esophagus to maintain the LES well below the diaphragmatic hiatus. An acute angle of His is reinstituted via limited (90°–120°) esophagogastroplication to create the gastroesophageal flap valve. Finally, using the dedicated deployment tool, the RefluxStop implant is placed in a superiorly oriented fundic pouch with loose suturing to maintain the device in its fully invaginated position. It is essential to place the implant as superiorly as possible to ensure the LES maintains sufficient distance from the diaphragm during respiration.
Data extraction and analysis
Retrospective chart analysis provided clinical data to be collected in an electronic database. The primary effectiveness outcome was a change in total GERD Health-Related Quality of Life (GERD-HRQL) score (i.e., pre- and postoperative) which was obtained via a questionnaire (total range: 0–75) with higher scores indicating more severe symptoms. 13 Subdomain scores between baseline and follow-up were compared both by absolute scores and by the proportions of patients experiencing domain-specific symptoms (i.e., heartburn, regurgitation, and dysphagia). Secondary effectiveness outcomes included GERD symptomatology, the proportion of patients requiring PPI therapy, and patient satisfaction. Safety outcomes consisted of perioperative AEs, including procedure- and device-related AEs.
Statistical analysis
For descriptive analyses, continuous data were summarized by minimum, maximum, median, quartiles (Q1, Q3), mean, and standard deviation (SD); categorical parameters were summarized using counts and percentages. The distribution of continuous data was inspected by histograms, bar graphs, box plots, and scatter plots.
Continuous data were tested for normal distribution via the Shapiro–Wilk test. For comparison of baseline and follow-up values, normally distributed data were compared via the student’s t-test and non-normally distributed data via the Wilcoxon-signed-rank test. For quantitative variables, differences between counts were tested using Pearson’s chi-squared test or Fisher’s exact test if expected counts for any cell were <5.
Unless stated otherwise, patients with missing data for an analyzed parameter were excluded from the retrospective analysis, with the remaining patients set as 100%. Differences were considered significant if the P value was below .05.
Statistical analysis and generation of tables, patient data listings, and figures were performed using R version 4.2.2 under the Microsoft Windows operating system at the computer facilities of the assigned CRO, DBM, Germany. The following R packages were used for analysis: car, cowplot, DescTools, flextable, ggalluvial, knitr, lubridate, markdown, readxl, rmarkdown, reshape2, and tidyverse.
Results
Baseline characteristics
Twenty-eight patients with GERD were managed with RefluxStop surgery via a minimally invasive technique with a mean (SD) follow-up at 14.1 (4.7) months. Baseline patient characteristics are delineated in Table 1.
Patient Characteristics (n = 28) and Baseline Parameters
BMI, body mass index; GERD-HRQL, Gastroesophageal Reflux Disease Health-Related Quality of Life; LA, Los Angeles; PPI, proton pump inhibitor; SD, standard deviation.
Effectiveness outcomes
GERD-HRQL score
The median (Q1, Q3) total GERD-HRQL score improved by 88.6% from a baseline of 35 (31.5, 39.2) to 4 (3, 7.2) at follow-up, as depicted in Figure 2 (P < .05). Dysphagia GERD-HRQL subdomain score >2 and odynophagia subdomain score >2 were not present in any patient (n = 0) at follow-up compared to baseline values of 35.7% (n = 10) and 14.3% (n = 4), respectively (see Table 2). Heartburn GERD-HRQL subdomain, combining six heartburn questions with a possible score of 30, was reduced to a mean (SD) score of 1.7 (1.2) from 18.1 (6.1) at baseline and no patient (n = 0) had a heartburn score >5 at follow-up compared with 100% (n = 28) at baseline (Table 2). The median (Q1, Q3) heartburn subdomain decreased from 18 (13, 22.5) preoperatively to 2 (1, 3) at follow-up (P < .05) (Fig. 3A). Similar results were observed for regurgitation which also consists of six questions with a possible score of 30. The mean (SD) regurgitation score decreased from 13.2 (4.7) at baseline to 2 (1.6) at follow-up and no patient (n = 0) had a score >5 at follow-up compared to 100% (n = 28) at baseline. The median (Q1, Q3) regurgitation subdomain decreased from 12.5 (10, 15) preoperatively to 2 (0.5, 3) at follow-up (P < .05) (Fig. 3B).
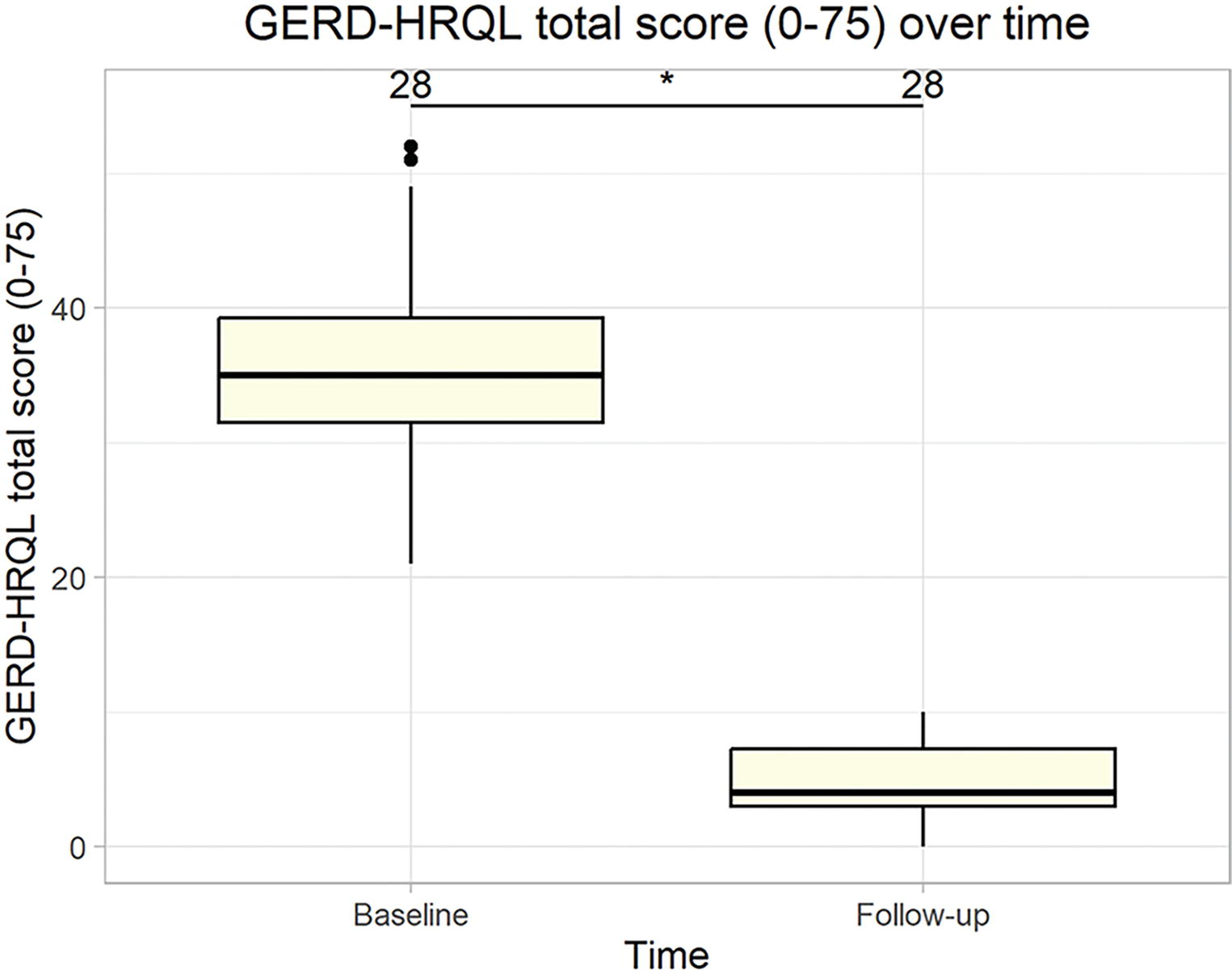
Median total GERD-HRQL score (0–75) over time which improved by 88.6% from baseline (P < .05). The mean (SD) follow-up time was 14.1 (4.7) months. GERD-HRQL, Gastroesophageal Reflux Disease Health-Related Quality of Life; SD, standard deviation.
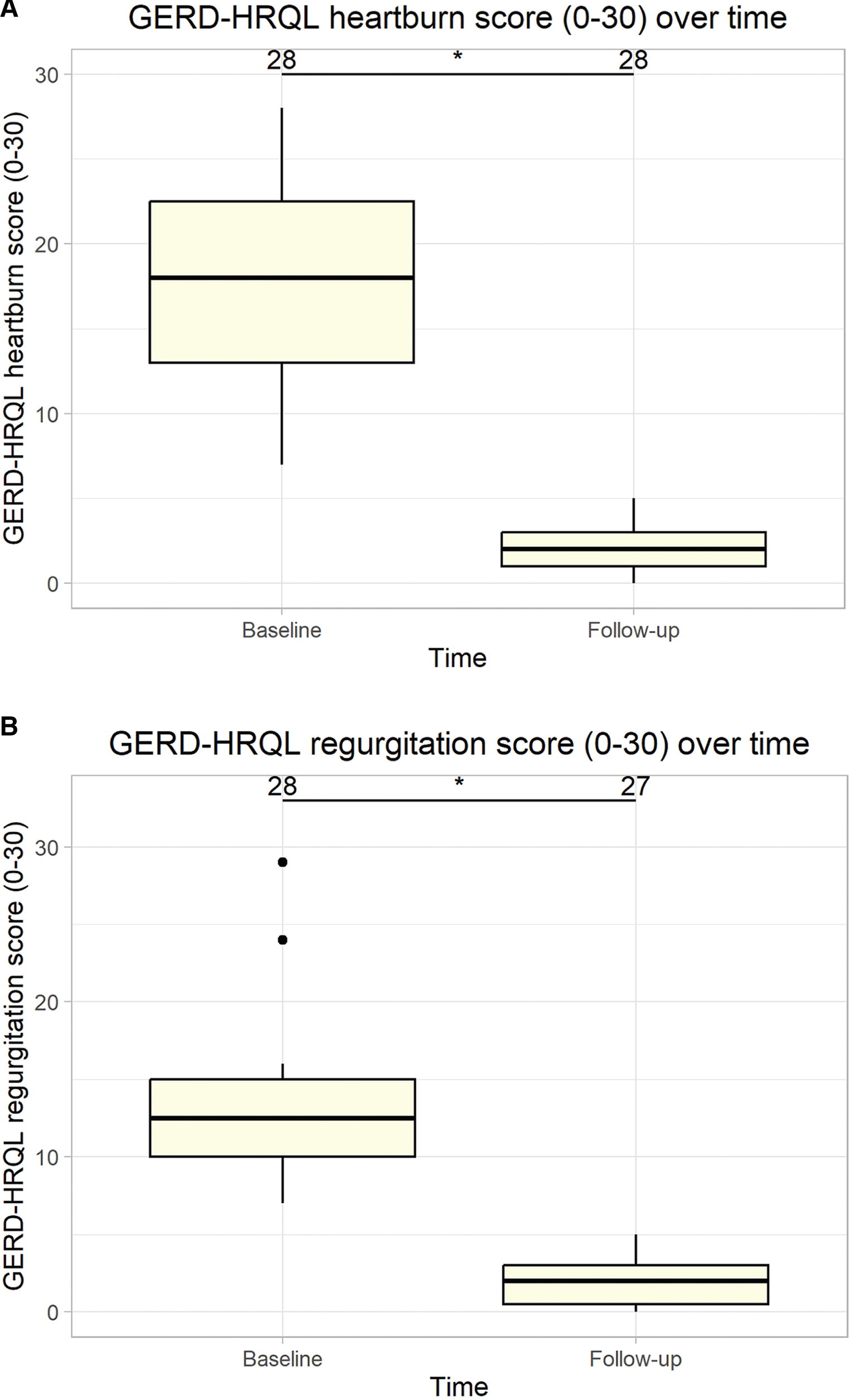
GERD-HRQL score subdomains: heartburn and regurgitation.*
Reflux Symptoms at Baseline Compared to Follow-Up (n = 28)
The proportion of patients with heartburn (P < .001), regurgitation (P < .001), dysphagia (P = .002), and odynophagia (P = .111) at follow-up was significantly different from baseline.
Subdomain consists of six questions from the GERD-HRQL questionnaire with a possible score of 30.
GERD-HRQL, Gastroesophageal Reflux Disease Health-Related Quality of Life; SD, standard deviation.
Symptomatology
In terms of binary description of reflux symptoms, all cases of preoperative heartburn (n = 28), regurgitation (n = 28), and dysphagia (n = 10) completely resolved (n = 0) at follow-up. Before surgical intervention, all (100%) patients were dissatisfied with their disease state according to the questionnaire. Postoperatively, 96.4% (n = 27) of patients were satisfied with GERD treatment with the RefluxStop procedure.
Reliance on PPI therapy
At baseline, 93% (n = 26) of patients took PPI therapy to manage symptoms at a mean (SD) dose of 55.4 (21) mg per day with a range of 20–80 mg per day. After RefluxStop surgery, only two (n = 2) patients required regular daily PPI therapy; one (n = 1) patient had gastritis, and one (n = 1) patient had persistent but improved reflux symptoms. The mean (SD) PPI dose at follow-up was 1.8 (5.5) mg/day with a range of 0–20 mg/day.
Safety outcomes
No cases of reoperation or readmission for intervention, such as esophageal dilatation for postoperative dysphagia, were performed. Minor and quickly resolvable intraoperative AEs (i.e., neck emphysema, eye emphysema, and pleural opening) occurred in seven patients. However, none of the intraoperative AEs were RefluxStop-specific.
Discussion
The results of this study indicate that RefluxStop surgery is a safe and effective treatment option for patients with chronic GERD at least in short-term follow-up. This was demonstrated by favorable outcomes pertaining to symptom resolution, quality of life, patient satisfaction, and reliance on PPI therapy without significant manifestation of safety concerns. More specifically, patients experienced 88.6% improvement in median GERD-HRQL score with complete resolution of preoperative dysphagia (35.7% at baseline to 0% at follow-up). No cases of new-onset dysphagia occurred following RefluxStop surgery, a cumbersome postoperative sequela that is common in Nissen fundoplication cases. According to Spence et al., dysphagia was reported in 48.7% of patients at 1-year follow-up after Nissen fundoplication, 14 whereas Mickevičius et al. reported dysphagia in 24% of patients 15 at 1 year. The favorable outcome of RefluxStop surgery pertaining to this complication is likely due to the avoidance of encircling and applying pressure on the esophagus. With Nissen fundoplication, dysphagia most commonly arises from the wrapping of the fundus around the distal esophagus. 16 Patients were satisfied (96.4%; n = 27) with the RefluxStop procedure and only two (n = 2) patients demonstrated PPI usage at follow-up. One (n = 1) of the two cases requiring PPI therapy at follow-up was for persistent but improved reflux symptoms; the other case was indicated for gastritis. Although minor AEs occurred intraoperatively during this study, none of these events were of any concern or considered procedure-specific or device-related, bolstering the safety outcomes of the RefluxStop procedure.
In Germany, GERD is a common disorder with an expensive management process that presents numerous obstacles for the healthcare system. 5 Moderate and severe symptoms, a predictor of PPI failure when baseline evaluation shows higher GERD Questionnaire scores, 17 most commonly occur in German patients aged 50–69 years. 5 Despite one in four adults experiencing these more severe symptoms, 5 less than 1% of patients with GERD are managed with antireflux surgery in Germany annually. 18 Thus, surgical treatment options may be an essential treatment alternative for this large subset of reflux sufferers. This presents one avenue of optimizing GERD treatment in Germany to improve the patient experience and reduce the burden of disease on the healthcare system and economy, particularly when considering antireflux surgery is significantly superior to medical therapy for complicated cases of reflux disease. 19
Surgical treatment options for reflux disease in Germany include fundoplication techniques and magnetic sphincter augmentation (MSA).20,21 Although both modalities are effective, a significant burden of unmet needs persists in relation to the postoperative manifestations of fundoplication and MSA. Nissen fundoplication is regarded as standard of care according to guidelines worldwide. The literature on Nissen fundoplication provides the following examples of high-quality studies: Koch et al., 22 Draaisma et al., 23 Spence et al., 14 and Yang et al. 24 all reporting rates of approximately 10% or more for reoperation at 1-year follow-up. Moreover, Håkansson et al. 25 and Nijjar et al. 26 reported rates of 17% and 12.5% for PPI use at 1-year follow-up, respectively. The addition of reoperation and PPI use considerations provides an indicative understanding of treatment success and is overall substantially unfavorable compared to the RefluxStop data presented in this report; however, direct comparative studies are preferred and more definitive.
Although MSA is positioned to have fewer unwanted effects than fundoplication due to the claimed lower incidence of gas-bloating syndrome and a sustained ability to belch or vomit, early postoperative dysphagia occurs in a substantial proportion of patients (i.e., 43%–83%). 27 This postoperative dysphagia persists in the longer term in approximately 19% of patients treated with MSA, of which 30%–43% require subsequent esophageal dilatation.28,29 Moreover, MSA is associated with tissue erosion at the site of device placement as well as device migration.28,29 No such events occurred with RefluxStop in this study, however, direct comparison with head-to-head study is required to juxtapose the safety and effectiveness of this emerging technology with fundoplication techniques and MSA.
Strengths and Limitations
A strength of the present study is the lack of interoperator variance influencing the results, as patients were operated on by one surgeon. Operative technique is subject to differences between surgeons as with any type of antireflux surgery. Another strength of the study is the inclusion of a large proportion of difficult-to-treat patients (i.e., large hiatal hernia in 35.7% of size 4–6 cm). The results from this ongoing cohort, in conjunction with other studies assessing RefluxStop with the inclusion of such patients, have supported the broader indication of the RefluxStop device in real-world settings. Moreover, this analysis provided a detailed evaluation of quality-of-life improvements following RefluxStop surgery with subdomains (i.e., heartburn, regurgitation, dysphagia, and odynophagia) of the GERD-HRQL score outlined.
Notable limitations of this study are the small sample size (n = 28) and short follow-up (i.e., mean 14.1 months); however, evaluation of this cohort is ongoing, and additional patients are treated with RefluxStop surgery for ad hoc inclusion. Furthermore, RefluxStop was not compared to other available treatment options in Germany (i.e., Nissen fundoplication and MSA) in this study and only indirect comparisons are possible with these results. Additional randomized studies are required to provide direct comparisons between RefluxStop and fundoplication to effectively delineate the role of RefluxStop surgery in Germany.
Conclusion
Based on this analysis, RefluxStop surgery results in excellent clinical outcomes in the management of chronic GERD. Moreover, all patients were completely relieved of their dysphagia, where more than one-third had dysphagia preoperatively, and no new-onset dysphagia occurred. Treatment with this emerging technology improves reflux disease symptomatology and quality of life significantly. Both the lack of PPI usage for reflux symptoms and patient satisfaction in over 96% of subjects are clearly superior to the results previously achieved at this clinic for the same follow-up period with standard-of-care treatment options. Additional studies should be conducted to delineate the broader role of this implantable device.
Footnotes
Author’s Contributions
Conceptualization: M.E., Statistical Analysis: M.E., Writing the manuscript: M.E.
Data Availability
Anonymized data can be provided upon request.
Ethics
Ethics approval was not required since there were no changes in the institutional standard of care. All patients provided informed consent to undergo surgery as per standard clinical practice and for the use of anonymized health-related data that were included in the analysis.
Author Disclosure Statement
M.E. has a consultancy agreement with Johnson & Johnson that is not related to this article.
Funding Information
M.E. receives travel support and conference honoraria from Implantica (Zug, Switzerland). Article processing charges for this article are supported by Implantica (Zug, Switzerland).