
Abstract
Background:
Bar stabilization during minimally invasive pectus excavatum repair (MIRPE) is critical to avoid dislodgement. Multiple techniques are described including stabilizers, wires, and sutures. This retrospective study compared bar movement and outcomes between existing techniques and ZipFix™, a biocompatible cable tie.
Methods:
Patients ≤20 years of age who underwent MIRPE with ZipFix between January 2021 and September 2022 were compared with historical controls who underwent repair by same surgeons between January 2018 and December 2020 using stabilizers or polydioxanone suture (PDS). Demographics, clinical details, and outcomes were compared using Kruskal–Wallis and chi-square tests.
Results:
Of the 116 patients who underwent repair, 45 had bars secured with ZipFix (39%) and 71 (61%) were historical controls (35 stabilizer, 36 PDS). Median (interquartile range) age was 15 (14–16) years and Haller index was 3.9 (3.6–4.5). Nine (8%) patients required two bars. Haller index and use of second bar were comparable between stabilization techniques (P > .05). In total, 49 patients (40%) reported any pain at 1 month and this was similar between stabilization techniques (P = .45). Median bar movement was greater for bars secured with PDS than with ZipFix or stabilizers at 1 month (5.5 versus 2.3 versus 3.3°, P = .010) and last follow-up (6.5 versus 2.1 versus 3.6°, P < .001). One patient whose bar was secured with PDS required revision for dislodgement.
Conclusion:
Pectus bar stabilization with ZipFix is a safe alternative to metal stabilizers and both techniques are superior to suture stabilization alone. The use of ZipFix may be preferred given its lower cost and ease of use.
Introduction
Pectus excavatum is the most common congenital chest deformity in children.1,2 Minimally invasive repair using the Nuss procedure under thoracoscopic vision is the procedure of choice.3–5 The Nuss procedure involves placing a flat curved metal bar under the sternum, anterior to the pericardium. The convexity of the Nuss bar elevates the sternum and provides internal bracing until the growth and ossification of the chest wall are complete. The bar is secured to the ribcage using wires, sutures, or lateral metal stabilizers.5–7 A novel bar fixation method with ZipFix® (DePuy Synthes, West Chester, PA), a biocompatible cable tie, has recently been described in the literature.8,9 Bar fixation techniques are critical to avoid bar dislodgement and recurrence of deformity.
Fixation with wires provides excellent bar stability; however, the risk of breakage and subsequent lung trauma have replaced its use with pericostal sutures.10–13 Absorbable pericostal sutures, particularly monofilament polydioxanone sutures (PDSs), are widely used, with ∼2% requiring revision surgery for bar dislodgement.12,14 The use of lateral metal stabilizers has reduced this rate to 1%, preferred particularly for those patients with a higher risk of bar displacement, such as those with higher age at repair, rigid chest walls, or severe deformities.5,6
However, pain and deformity at the site of the stabilizer are frequent complaints that often go unreported. ZipFix is FDA approved for sternal closure after cardiac surgeries.9,15,16 Its use for Nuss bar stabilization was first reported by Tam et al. with no significant bar dislodgement. 8 Although the incidence of bar dislodgements requiring revision surgery has reduced with the above techniques, bar migration remains an important concern and the optimal bar fixation technique is unknown.
This study primarily aimed to compare bar movement among the commonly used bar fixation techniques at our institution, namely, PDSs, stabilizers, and ZipFix. In addition, secondary outcomes such as infections and reoperations, including other complications, were studied.
Methods
Cohort
A retrospective cohort study was conducted after approval by the institutional review board. Patients ≤20 years of age who underwent minimally invasive pectus excavatum repair (MIRPE) using Nuss procedure with ZipFix from January 2021 to September 2022 were compared with historical controls who underwent repair by the same surgeons between January 2018 and December 2020 using stabilizers or PDSs (i.e., ZipFix versus stabilizers versus PDS). Patients who underwent revision after primary pectus repair elsewhere were excluded.
Data collection
Data collected included demographics, Haller index, presence of scoliosis, operative details (type of analgesic technique, bar fixation method, and number of bars), clinical outcomes (length of stay, complications, and reoperations), bar position (at discharge, 1-month, and last follow-up), and total follow-up time.
Analysis plan
Statistical analyses were performed using IBM SPSS Statistical Software Version 28.0 (IBM Corp., Armonk, NY). Continuous variables were compared using analysis of variance and Kruskal–Wallis tests. Categorical variables were compared using chi-square tests. P values <.05 were considered statistically significant. Data are presented as mean, median, and numbers with percentages.
Surgical technique
All patients underwent MIRPE by the same group of surgeons. Sternal elevation was not performed. Patients received either bilateral percutaneous paravertebral blocks by anesthesia or, more recently, intraoperative bilateral thoracoscopic intercostal nerve cryoablation with intercostal nerve blocks for postoperative analgesia. Once in place, the bar was secured to the adjacent ribs and intercostal muscles at both ends — using absorbable sutures at one end and ZipFix at the other end in the ZipFix group, using PDSs at both ends in the PDS group, and using absorbable sutures at one end and stabilizers at one or both ends in the stabilizer group.
Placement of ZipFix
The ZipFix implant comes with a large, blunt, and noncutting insertion needle that can be safely passed through the intercostal muscles. Once the bar was positioned, the closest appropriate rib was identified for fixation (Supplementary Video S1). The ZipFix needle was inserted cephalad to the selected rib near the eye of the Nuss bar. An exit thoracostomy was created caudal to the rib. A needle driver was positioned through the exit site to grasp the needle intrathoracically under thoracoscopic vision. The back of the needle was pushed, and the tip was grasped and pulled out with the needle driver. This maneuver simplified the placement of the ZipFix tie around the rib. Once the needle was out, it was removed using a cable cutter, and the tie was assembled as a standard cable tie. The manufacturer's tension applicator was used to tighten and cut the excess tie. Since the fixation of one end with ZipFix and the other end with sutures seemed to provide sufficient bar stability, a second ZipFix tie has not been used at the opposite end. Intercostal muscle is frequently secured to the eye of the bar on the side of the ZipFix in an effort to reduce the risk of the tie from sliding off the end of the bar.
Measurement of the bar position and bar movement
The position of the bar was measured with respect to the vertebral column as an angle between the lines along the upper border of the bar and the anterior vertebral ligament (i.e., along the anterior vertebral line) on lateral chest X-ray (CXR) (Fig. 1). The angles were measured at discharge, at 1 month, and on the last available lateral CXR with the bar. The difference between the angles (i.e., at 1-month follow-up minus discharge, and on the last CXR minus discharge) was calculated as the degree of bar movement, Delta. For those with two bars, the lower bar was labeled as Bar 1 and the upper bar as Bar 2.
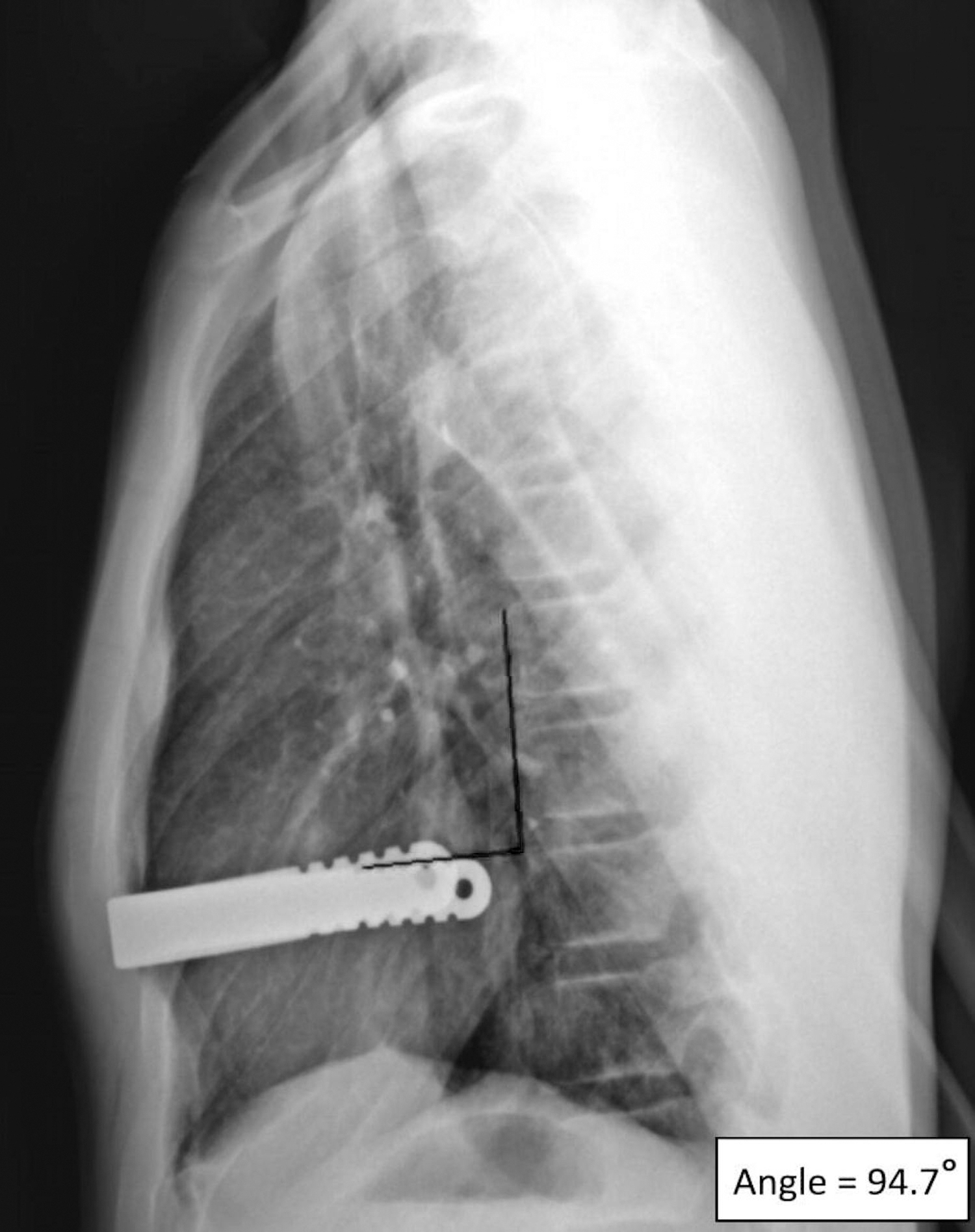
Bar angle measurement. The angle is measured between the lines drawn along the upper border of the bar and the anterior vertebral line (i.e., along the anterior vertebral ligament.
Results
Cohort characteristics
Of the 116 who met the inclusion criteria, 45 (39%) patients had bars secured with ZipFix, 35 (30%) with stabilizers (30 had unilateral and 5 had bilateral stabilizers), and 36 (31%) patients with PDS (Table 1). The median (interquartile range) age was 15 (14–16) years and Haller index was 3.9 (3.6–4.5). Nine (8%) patients required two bars. Twenty-two (19%) patients had scoliosis. The median 1-month follow-up time was 35 (29–44) days, and the median total follow-up time was 210 (53–399) days.
Patient Characteristics with ZipFix Versus polydioxanone Suture Versus Stabilizers
Chi-square test.
Kruskal–Wallis test.
INB, intercostal nerve blocks; INC, intercostal nerve cryoablation;
Stabilization techniques
Outcomes were compared between the three stabilization techniques—ZipFix versus PDS versus stabilizers (Table 2). Gender, Haller index, the use of second bar, and the presence of scoliosis were comparable among the three groups (P > .05). Although there was a statistical difference in age, it was not clinically significant (median [years]—15 versus 14 versus 15, P = .02). The median bar movement was greater for bars secured with PDS than with ZipFix or stabilizers at 1 month (5.5° versus 2.3° versus 3.3°, P = .01) and at the last follow-up (6.5° versus 2.1° versus 3.6°, P = .015).
Degree of Bar Movement with ZipFix Versus polydioxanone Suture Versus Stabilizers
Kruskal–Wallis test.
CXR, chest X-ray; dc, discharge;
Secondary outcomes
Forty-nine patients (40%) reported pain at 1-month follow-up, and this was similar among the stabilization techniques (P = .45). Six patients (5%) had intervention-requiring complications (Table 3). Three of these patients had bar fixation with PDS and the other 3 had ZipFix. Pneumonia and bar infection were seen in a patient with ZipFix; however, the infection was on the contralateral side of ZipFix placement. One patient whose bar was secured with PDS required revision surgery for bar dislodgment (bar movement was 15° at 1-month follow-up and 20° at 2 months follow-up when the revision was considered).
Intervention-Requiring Complications
Discussion
Nuss bar stabilization is fundamental for the effective correction of pectus excavatum. Bar dislodgement can lead to chest pain, recurrence of deformity, and the need for reoperation. Several bar fixation techniques are used at various institutes and include wires, sutures, lateral metal stabilizers, and the novel biocompatible cable tie, ZipFix. This study compared the outcomes among the three bar stabilization techniques (PDS, stabilizers, and ZipFix) used in pediatric patients at our institution. Greater bar movement was noted with PDS than with ZipFix or stabilizers. None with ZipFix or stabilizers required revision surgery.
ZipFix is a biocompatible poly ether–ether–ketone cable tie. 9 It is widely used for sternal closure after sternotomies for cardiac surgeries.9,15,16 Its material inertness, flexibility, smooth blunt ends, resistance to breakage, and high tensile strength make it suitable for securing the Nuss bar to the adjacent rib.8,9 However, it cannot be seen on radiographs due to its radiolucency.
Since 2021, ZipFix has been used as the primary bar stabilizing technique at our institution across all pediatric age groups and severities of deformity. Although Tam et al. secured both ends of the bar with ZipFix in most of their patients, in our study, we secured one end of the bar with a single ZipFix and the other end with absorbable sutures. 8 The side of ZipFix placement was at the discretion of the surgeon. Unilateral ZipFix use without fixation of the other end can lead to bar movement, as was seen in the initial cases of Tam et al. Although our study found no difference in the bar movement between ZipFix and stabilizers, it is worth noting that ZipFix is 1/10th the price of a metal stabilizer. 8 Single unilateral ZipFix with pericostal sutures at the opposite end can be a cost-effective alternative.
Complications encountered in this study were consistent with previous studies.4,6,10,12,13 Postoperative complications, particularly involving the bar, can be concerning. Bar infections, however, are often managed conservatively without the need for bar removal.17,18 It is likely that the bar infection observed in one of our patients with ZipFix was due to postoperative pneumonia and not due to ZipFix, as the infection occurred on the contralateral side of ZipFix placement. Compared with wires, the use of ZipFix for sternal closure has been shown to improve sternal stability and reduce pain with no increased risk of wound infections.15,16 The incidence of infections was reduced in one of the studies. 19
Similar to previous studies, this study also experienced bar displacement requiring revision surgery with PDS use.10,12 Bar migration has been classified as superior, inferior, lateral movement or sliding, rotation, and flipping.20,21 However, variations in patient position during radiographs can be misinterpreted as bar movement (pseudomigration). 20 Careful evaluation of the bar position with respect to the vertebral column, ribs, or sternum on both anteroposterior and lateral chest radiographs is important. 20 This study chose to measure bar position with respect to the vertebral column due to better visibility of the spine compared with the sternum and ribs on most chest radiographs.
Neither Tam et al. nor this study had any event of ZipFix fracture as was seen with wires. The soft blunt ends of the ZipFix decrease the risk of lung trauma and subsequent pneumothorax.8,9 Tam et al. observed alleviation of pain after replacing the stabilizer with ZipFix in a patient requiring revision surgery for persistent pain. 8 It is hypothesized that the flexible nature of ZipFix tends to exert less bending force on the ribs, thereby causing relatively less pain compared with the nonyielding metal stabilizers. 8
Furthermore, the cable tie principle of the ZipFix makes it easier to use and decreases the time to implant. The use of the manufacturer's tension applicator is recommended to secure the pericostal ZipFix at appropriate tension and to prevent excessive tightening and damage to the intercostal neurovascular bundle. 8 The tissue hyporeactivity of the ZipFix makes it readily identifiable and simple to cut with a wire cutter during removal.8,9
This study was limited by its small size and retrospective nature. However, given the rarity of bar displacements with the current stabilization techniques, conducting a prospective study to further evaluate bar dislodgements can be challenging. Furthermore, a standard method to measure bar movement is lacking. This study used a simple method to measure bar movement with respect to the vertebral column, which is different from previous studies.22,23
Conclusion
Pectus bar stabilization with ZipFix is a safer alternative to metal stabilizers in pediatric patients regardless of the age at repair or the severity of the deformity. Although both techniques are superior to suture stabilization alone, the use of ZipFix may be preferred given its lower cost and ease of use.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.