
Abstract
Background:
The contracted gallbladder may predispose to a higher rate of biliary or vasculobiliary injury (VBI). It is usually associated with unclear anatomy due to chronic inflammation and fibrosis in the hepatoduodenal ligament region. Laparoscopic ultrasound (LUS) can very effectively delineate anatomical conditions during cholecystectomy. Our study aimed to compare the visual and ultrasonographic navigation around the shrunken gallbladder.
Materials and Methods:
The study group consisted of 612 patients qualified for laparoscopic cholecystectomy. The shrunken gallbladder was diagnosed intraoperatively in 13 patients (2.1%). In 6 patients, the only intraoperative navigation method was a visual evaluation of anatomical conditions, and in 7 patients, the method was LUS.
Results:
The operating time and the length of hospital stay after surgery were significantly lower, the number of conversions was insignificantly lower, and the number of successful visualization of anatomical conditions was significantly higher in the LUS group. We did not observe any bile duct and VBI in patients with the shrunken gallbladder.
Conclusions:
The combination of the fundus-first and subtotal cholecystectomy with LUS navigation might be an effective proposal when coming across the shrunken gallbladder.
Introduction
Laparoscopic cholecystectomy may be challenging. Sometimes chronic cholecystitis can lead to a small contracted gallbladder, which indicates surgery. 1 The shrunken gallbladder characteristics are pericholecystic fibrosis, loss of elasticity, and thickening of the wall. It is also usually associated with obscured anatomy in the hepatocystic triangle, elevation of the hepatoduodenal ligament with fibrosis, and obliteration of the cystic duct and the cystic artery, and adhesions to the surrounding organs. Chronic inflammation may predispose to the common bile duct (CBD) stones formation.2,3
Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) defined pitfalls in cholecystectomy. 4 One of them is chronic inflammation with dense scarring, a contracted gallbladder on ultrasound, and preoperative endoscopic retrograde cholangiopancreatography (ERCP), which is predictive for distorted anatomy and severe adhesions in the hepatocystic triangle. 4 The problem of safe management of the shrunken gallbladder is rather seldom addressed in the literature. The same is true for laparoscopic ultrasound (LUS), which is underutilized during laparoscopic cholecystectomy. 5
Materials and Methods
The study group consisted of 612 patients operated on between January 2014 and October 2020 in one department of surgery. The study's inclusion criterion was the cholecystolithiasis and symptoms of chronic cholecystitis with confirmed gallstones on abdominal ultrasound. The exclusion criteria were the pre- or postoperatively diagnosed cancer of the gallbladder (2 patients were excluded) and acute preoperative cholecystitis. The radiologist's preoperative abdominal ultrasound included the diagnosis of a smaller or contracted gallbladder without any specific information about the anatomical relationships in the hepatocystic triangle in 11 patients, and the shrunken gallbladder was diagnosed intraoperatively in 13 patients (2.1%). In 6 patients (4 women and 2 men), the only intraoperative navigation method was a visual evaluation of anatomical conditions (visual navigation in the operating field [VIS] group), and in 7 patients (4 women and 3 men), the method was LUS (LUS group).
Written informed consent was obtained from all patients before surgery. All procedures followed the ethical standards of the 1964 Declaration of Helsinki and its later amendments. The study was approved by the Ethical Committee of the Wroclaw Medical University (approval no. BW-24/2020).
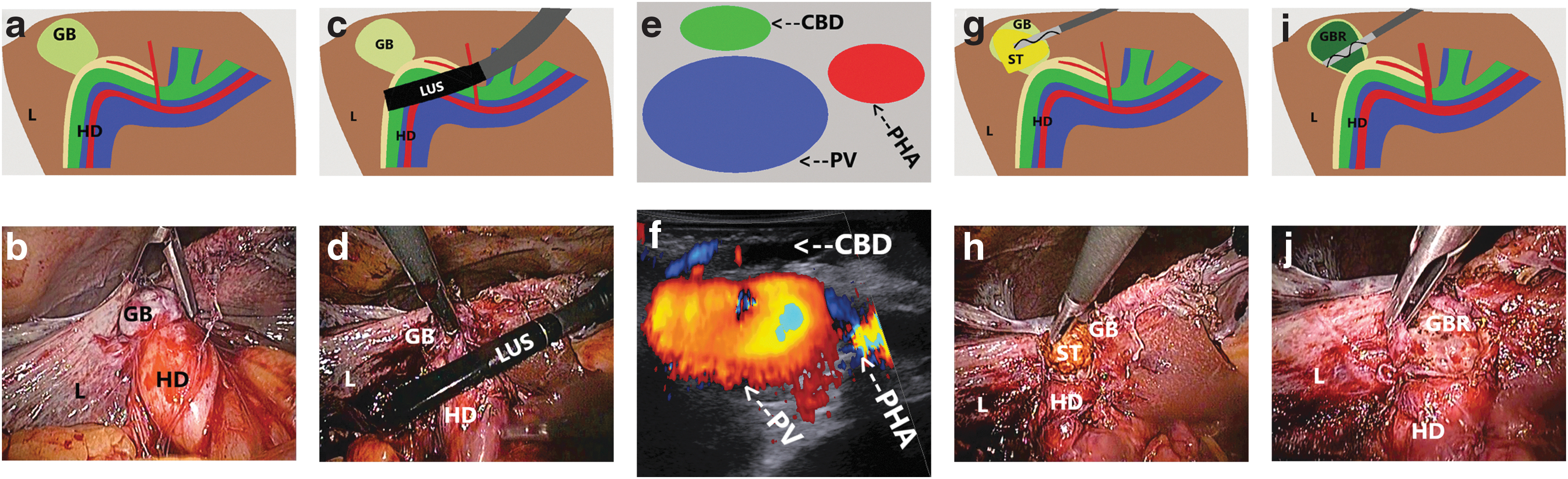
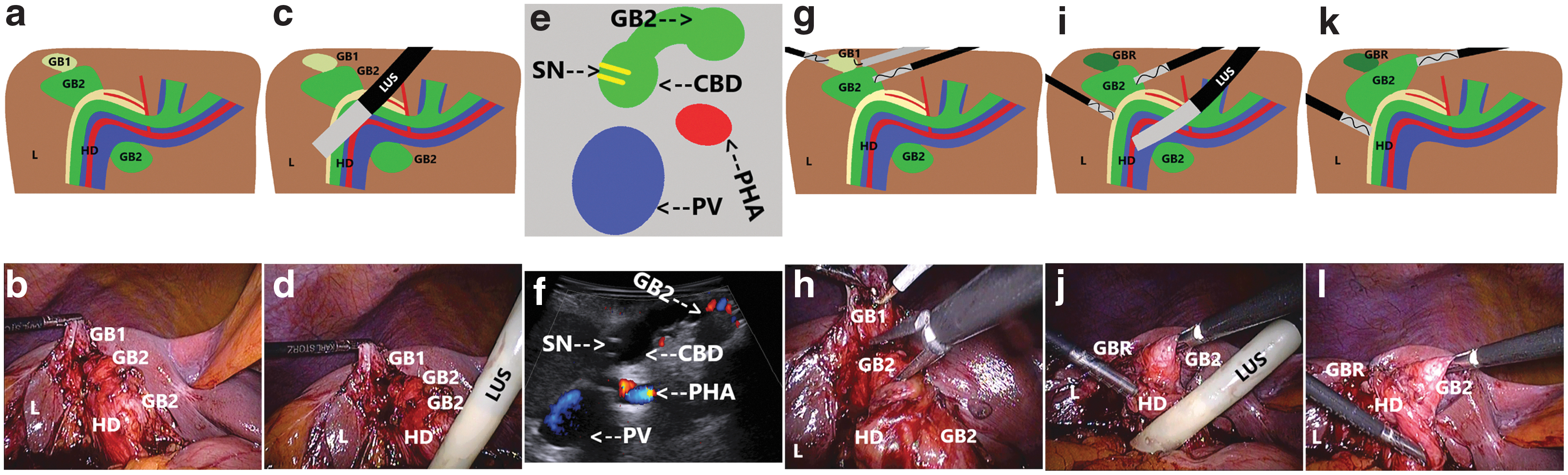
Cholecystectomies were performed on an elective basis by 5 surgeons experienced in laparoscopic cholecystectomy (>120 cholecystectomies). LUS was performed by 2 surgeons experienced in this technique (>70 examinations). For LUS, the laparoscopic probe Toshiba PEF-704 LA (frequency 7.0–10 MHz) and the diagnostic ultrasound system Toshiba NemioMX SSA-590A, all manufactured in Japan, or laparoscopic probe BK Medical 9066-RF and the diagnostic ultrasound system BK Medical 5000 (frequency 4.0–12 MHz), all manufactured in Denmark, were used. The LUS probe was inserted through the epigastric 10 mm trocar. The anatomical conditions throughout the procedure defined LUS with color Doppler function (Figs. 1e, f and 2e, f). In patients with preoperative endoscopic bile duct stenting during ERCP due to choledocholithiasis and narrowing of the bile duct, the stents were well visible on ultrasound that helped to identify CBD (Fig. 2e, f).
Surgical treatment of the single-chamber contracted gallbladder.
Surgical treatment of the double-chamber contracted gallbladder.
The technique of laparoscopic cholecystectomy with LUS navigation was a combination of a fundus-first and subtotal cholecystectomy. In patients with the single-chamber shrunken gallbladder, it consisted only of stones and most gallbladder wall removal over the safety line defined with LUS. The fluid in the contracted gallbladder was colorless. The internal orifice inside the shrunken gallbladder and the cystic duct in LUS were not visible, indicating the connection between the gallbladder and CBD was absent (Fig. 1a–j) (Supplementary Video S1). We did not observe any biliary fistulas during the postoperative period.
In patients with the double-chamber gallbladder, the shrunken gallbladder was treated the same way. The second functioning chamber (containing stones and the bile, connected with the CBD) was dissected laparoscopically under LUS control (Fig. 2a–l) (Supplementary Video S2). Still, in every case, due to undissectable fibrous tissue and the lack of a safe plane of preparation near the CBD, the operation was converted, and open cholecystectomy was performed.
Statistical Analysis
Descriptive statistics were used to describe the basic features of the data in the study. Statistical analysis included the Mann–Whitney U test for continuous variables and the Fisher's exact test for binary variables. The level of statistical significance was set at 95% (P < .05).
Results
The operating time and the length of hospital stay after surgery were significantly lower, and the number of successful visualization of anatomical conditions was significantly higher in the LUS group. The number of conversions was lower, and the number of preoperative bile duct stenting was higher in the LUS group but was statistically insignificant. There were no significant differences between the two groups according to age and the number of single- and double-chamber gallbladder visualized (Table 1).
Characteristics of the Study Group According to Age, Operating Time, Time Needed to Obtain LUS, Length of Hospital Stay After Surgery, Number of Single-Chamber and Double-Chamber Gallbladder, CON, BDI, and Number of Preoperative Bile Duct Stenting and Successful VIS and LUS
Statistically significant values (P < .05).
BDI, bile duct injury; CON, conversion; LUS, laparoscopic ultrasound navigation in the operating field; VIS, visual navigation in the operating field.
In the VIS group, all the operations were converted due to unclear anatomy. In the LUS group after confirmation of anatomical conditions, three operations with double-chamber gallbladder were converted due to laparoscopically undissectable inflammatory plane between the second chamber of the gallbladder and the CBD. We did not observe any bile duct injury (BDI) and vasculobiliary injury (VBI) (Table 1).
Discussion
BDI rate has plateaued over the last time and is close to the open cholecystectomy era ranging between 0.15% and 0.36%.6,7 The most common cause of BDI is misidentification of the visualized anatomical structures. Noteworthy is also surgeon skill and anatomical variations in the hepatocystic triangle. 4 When the dissection extends too low or too deep, it can lead to BDI or VBI. The recommended critical view of safety (CVS) in a small contracted gallbladder is impossible to achieve. BDI is more possible as the gallbladder may be closely associated with the hepatic duct in this situation. 4
The shrunken gallbladder is associated with a higher risk of intraoperative complications and the leading cause of conversion due to unclear anatomy, increased risk of bleeding, and problems with anatomical identification and orientation.3,4 In a study by Krähenbühl et al., the shrunken gallbladder was found in 3.05% of patients (the study group consisted of 12,111 patients), and BDI occurred in 2.97% of patients from this group in comparison with 0.30% from the whole study group that was statistically significant. 8 In a group with the contracted gallbladder, Huang et al. found a 12.5% complication rate, 3.1% BDI, and 15.6% conversion rate compared with average gallbladder patients. 3 The authors recommend a fundus-first cholecystectomy as the preferred method for the shrunken gallbladder being associated with lower conversion and complication rate and shorter hospital stay. Still, bail-out procedures are instead an option for more advanced laparoscopic surgeons.3,9
A 10-point intraoperative gallbladder scoring system developed under the World Society of Emergency Surgery leadership gives the contracted shrilled gallbladder 1 point in cholecystitis severity score. 9 A 9-point preoperative risk score to predict elective laparoscopic cholecystectomy's difficulty evaluates a shrunken gallbladder for 1 point. 10
The conversion rate for elective cholecystectomy varies between 3.16% and 7.5%.9,11–13 The shrunken gallbladder is rarely mentioned in the literature as the cause of conversion. Perhaps it is hidden in the group of technical or dissection difficulty and anatomic variations.12,13 All the operations in our study only under visual navigation were converted due to unclear anatomy. In the group with LUS, the conversion rate was 43% with well-defined anatomical conditions that made the open cholecystectomy easier. There are no recommendations if the conversion limits the risk or severity of BDI during difficult laparoscopic cholecystectomy. 7 It does not always provide a better view of the anatomy and may be associated with a higher risk of BDI and VBI. The younger generation of surgeons is not familiar with this technique. 14
In the obliterated hepatocystic triangle, SAGES recommends a fundus-first or a subtotal cholecystectomy with the removal of all stones and placement of a drain after the closure of the stump. Alternatively, the stump may be left open for a controlled fistula. 4 Our operative technique of the shrunken gallbladder is based on the “salvage technique” described by Nassar et al. It is a combination of the fundus-first and subtotal cholecystectomy under LUS navigation based on ensuring an optimal patient outcome: no stones in the gallbladder remnant without bile leak, BDI, and VBI. 2 LUS enabled a secure delineation of anatomy and proper qualification for the indicated surgical technique. Preoperative CBD stenting during ERCP may help orientation and visualize the bile duct, especially when the anatomy is distorted. 15
Anatomical misinterpretation is one of the most common causes of BDI and VBI; thus, successful identification of anatomy around the gallbladder may effectively reduce the number of complications.10,16,17 Methods of navigation include intraoperative cholangiography (IOC), CVS, near-infrared fluorescent cholangiography (NIRF-C), and LUS. 10 IOC is time consuming, involves radiation exposure, and sometimes dangerous dissection to cannulate the cystic duct that itself in case of mistaken anatomy may be the cause of BDI.10,18 To achieve the highest identification of biliary structures, at least a partial dissection during NIRF-C is needed; indocyanine green has to be injected intravenously. It is similar to IOC; only biliary structures are identified. 10 High-quality CVS cannot be achieved in progressive inflammation and fibrosis, and another three options should be chosen.2,10
In contrast, LUS is noninvasive, nonirradiating, visualizes vascular and avascular structures, is safe for both the patient and the operating team, and may be used an infinite number of times whenever needed. The only disadvantage seems to be a flat learning curve.5,10,19,20 According to the multisociety practice guideline on preventing BDI, IOC's potential benefit is early recognition and avoidance of increasing the severity of BDI. Still, no recommendations based on the available data were made. 7 There are also no recommendations on relaying on NIRF-C, which is not a substitute for the right dissection and identification technique. 7 LUS with appropriate experience and training may be used as an alternative to IOC. 7
Photo or video documentation, including LUS reports, may also be necessary for teaching, quality, and litigation purposes.7,21 Future research recommendations include the role of new imaging modalities in high-risk populations and the recognition of key strategies to enhance laparoscopic cholecystectomy safety. 7
Our study's limitation was a relatively small study group with the shrunken gallbladder, but in general, the number of patients with this form of chronic cholecystitis is small. Further studies, including larger groups of patients in more than one surgical center, are needed to confirm our findings and the presented method of dealing with the small contracted gallbladder.
Conclusions
To conclude, visual navigation in the case of the shrunken gallbladder seems to be insufficient. The combination of the fundus-first and subtotal cholecystectomy with LUS navigation enables a proper plane of dissection, decreases the conversion rate, and helps in decision making to perform a safe cholecystectomy when coming across the small contracted gallbladder.
Footnotes
Authors' Contributions
Substantial contributions to the conception or design of the study or the acquisition, analysis, or interpretation of data for the study were done by M.S. and J.R. Drafting the study or revising it critically for important intellectual content was performed by M.S. and J.R. Final approval of the version to be published was obtained by M.S. and J.R. Agreement to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved was by M.S. and J.R.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.