
Abstract
Abstract
Aim:
This study aims to analyze the efficacy and safety of the combination of laparoscope and preoperative (PODL) or intraoperative (IODL) duodenoscope in the treatment of cholecystolithiasis with choledocholithiasis.
Materials and Methods:
From January 2015 to February 2017, 51 patients with cholecystolithiasis and choledocholithiasis, who were treated with the PODL (n = 29) or IODL (n = 22), were reviewed retrospectively. The efficacy and safety were evaluated and compared between these two groups.
Results:
The success rates were 100% in IODL group and 96.6% in PODL group. There was no statistical significance in the difference of stone clearance rate and residual stone rate between two groups (P > .05). There were no significant differences in complications, like aspiration, gastrointestinal perforation, and acute cholangitis between two groups (P > .05). IODL significantly decreased numeric rating scale (NRS) scoring, reduced surgery cost and shortened hospitalization time compared to that of PODL group (P < .05). No cholangitis, reoccurrence of stones or biliary obstruction occurred in all 51 patients.
Conclusion:
In this retrospective study, IODL was found superior to PODL. And the IODL can significantly decrease NRS scoring, reduce surgery cost and shorten hospitalization time.
Introduction
Cholelithiasis, which is considered as a common disease in the clinic, is caused by several factors like metabolic abnormalities and lifestyle habits and it usually consists of cholesterol and pigments.1,2 According to the site of lithiasis, cholelithiasis is mainly divided into cholecystolithiasis, hepatolithiasis, and extrahepatic bile duct stones. Cholelithiasis is known as one of the most prevalent surgical ailments that clinical surgeons encounter during clinical practice; about 10%–15% of adults suffer from cholelithiasis in the United States.3,4 The morbidity of cholangiolithiasis is mainly associated with age and could reach 30% for elderly patients who are older than 60 years.5,6 When cholelithiasis combines with serious infections, the condition of patients may worsen to acute obstructive suppurative cholangitis, which is characterized by higher mortality. 7
Until now many strategies, including traditional open surgery, laparoscopic operation, and robotic surgery, have been applied for the treatment of cholecystolithiasis with choledocholithiasis. 8 The key point for treating cholecystolithiasis with choledocholithiasis is the complete removal of bile duct stones. However, each strategy has its advantages and disadvantages and none of the methods could provide a satisfactory effect. The laparoscopic cholecystectomy (LC) has been considered as the golden standard for cholecystolithiasis in clinical practice; however, there were still many controversies over the treatment of choledocholithiasis.9,10 Nowadays, open common bile duct exploration, laparoscopic common bile duct exploration, choledochoscopic common bile duct exploration, and endoscopic retrograde cholangiopancreatography (ERCP) (including endoscopic sphincterotomy [EST], endoscopic papillary balloon dilation [EPBD], and endoscopic nasobiliary drainage [ENBD]) are widely adopted in the treatment of choledocholithiasis. Usually, a multiple-method combination is adopted since a single method cannot completely clear the lithiasis. 11
In recent years, the combination of laparoscope and duodenoscope has become the most important strategy for cholelithiasis. 12 This strategy not only meets the requirement of minimal-invasive surgical approaches of natural cavities of the human body, but also improves the prognosis of patients. According to the timing of duodenoscope, this treatment strategy could be divided into three types, including preoperative, intraoperative, and postoperative duodenoscope. 13 The preoperative duodenoscope strategy is widely adopted by surgeons around the world for its convenience and definite efficacy. However, intraoperative duodenoscope could only be completed in the hybrid operating room that is equipped with advanced medical imaging devices by experienced endoscopists and surgeons. 14
Therefore, this retrospective study aims to analyze the operative effects, postoperative complications, economic indexes of operation, and short term follow-up of the patients with cholecystolithiasis and choledocholithiasis who were treated with preoperative or intraoperative combination strategies.
Materials and Methods
Patients and grouping
From January 2015 to February 2017, 51 patients with cholecystolithiasis and choledocholithiasis were treated with preoperative or intraoperative combination strategies in the First Affiliated Hospital of Dalian Medical University. All of the patients were divided into preoperative ERCP/EST/EPBD/ENBD+LC group (laparoscope and preoperative duodenoscope [PODL] group) and intraoperative ERCP/EST/EPBD/ENBD+LC group (intraoperative duodenoscope [IODL] group). This study was approved by the Ethical Committee of First Affiliated Hospital of Dalian Medical University, Dalian, China.
Inclusive and exclusive criteria
Inclusive criteria: (1) Recurrence of right upper abdominal pain with or without jaundice. (2) Cholecystolithiasis and choledocholithiasis were diagnosed by at least two of imaging examinations including ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI). (3) The diameter of choledocholithiasis was less than 20 mm.
Exclusive criteria: (1) Patients who were younger than 18 years or older than 80 years. (2) The maximum diameter of the extrahepatic bile duct stone was more than 20 mm. (3) Patients with recurrence of choledocholithiasis, Mirizzi syndrome, or hepatolithiasis. (4) Patients combining with biliary tract tumors or other tumors. (5) Patients who were not suitable for LC or duodenoscope.
Operation methods
In this study, the preoperative preparation was performed according to the previous study. 15 The LC operation was performed in accordance with previously published literature.4,8 ERCP operation was also performed according to the description of Li et al. 16
Main outcome measures
Operative indicators: (1) Operative duration: total time of ERCP and LC. (2) Intraoperative bleeding: the total amount of bleeding of ERCP plus LC. (3) Stone clearance rate. (4) Residual stone rate.
Postoperative complications: (1) ERCP associated complications: aspiration pneumonia, post-ERCP pancreatitis (PEP), gastrointestinal perforation, and acute cholangitis. (2) LC associated complications: biliary leakage and bile duct injury. (3) Other complications: bleeding, infection, cerebrovascular accidents, and death.
Other indicators: (1) Pain scoring (numeric rating scale [NRS]): for PODL group, NRS score was the average of post-ERCP and post-LC (Fig. 1). (2) Surgery cost: total cost of duodenoscope and LC. (3) Hospitalization time.

The graph for the numeric rating scale system for pain scoring.
Statistical analysis
All of the data were analyzed by SPSS software 20.0 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.). The quantitative data were recorded as mean ± standard deviation and analyzed by using Student's t-test for analysis between two groups. Meanwhile, Tukey's post hoc test was used to validate analysis of variance (ANOVA) for comparing measurement data between groups. The categorical variables (recorded as percentage) were analyzed by the chi-square test. All the data were obtained through at least six independent tests or experiments. Statistical significance was defined as P < .05.
Results
Comparison of the basic materials in two groups
To confirm the accuracy of the statistical results, the basic materials were compared between the two groups. The results showed that there were no significant differences for age, alanine aminotransferase, total bilirubin, alkaline phosphatase, γ-glutamyl transferase, Child-Pugh grading of liver function, maximum diameter of gallbladder stones, maximum diameter of choledocholithiasis, and maximum diameter of common bile duct between the two groups (Table 1, P > .05). Therefore, the data in the two groups were comparable.
Comparison of the Clinical Materials Between Two Groups
γ-GT, γ-glutamyl transferase; ALP, alkaline phosphatase; ALT, alanine aminotransferase; ERCP, endoscopic retrograde cholangiopancreatography; LC, laparoscopic cholecystectomy; TB, total bilirubin.
Operation in two groups
For all of the 51 patients, the total operation success rate was 98.0% and detailed grouping of surgical procedures was shown in Figure 2.
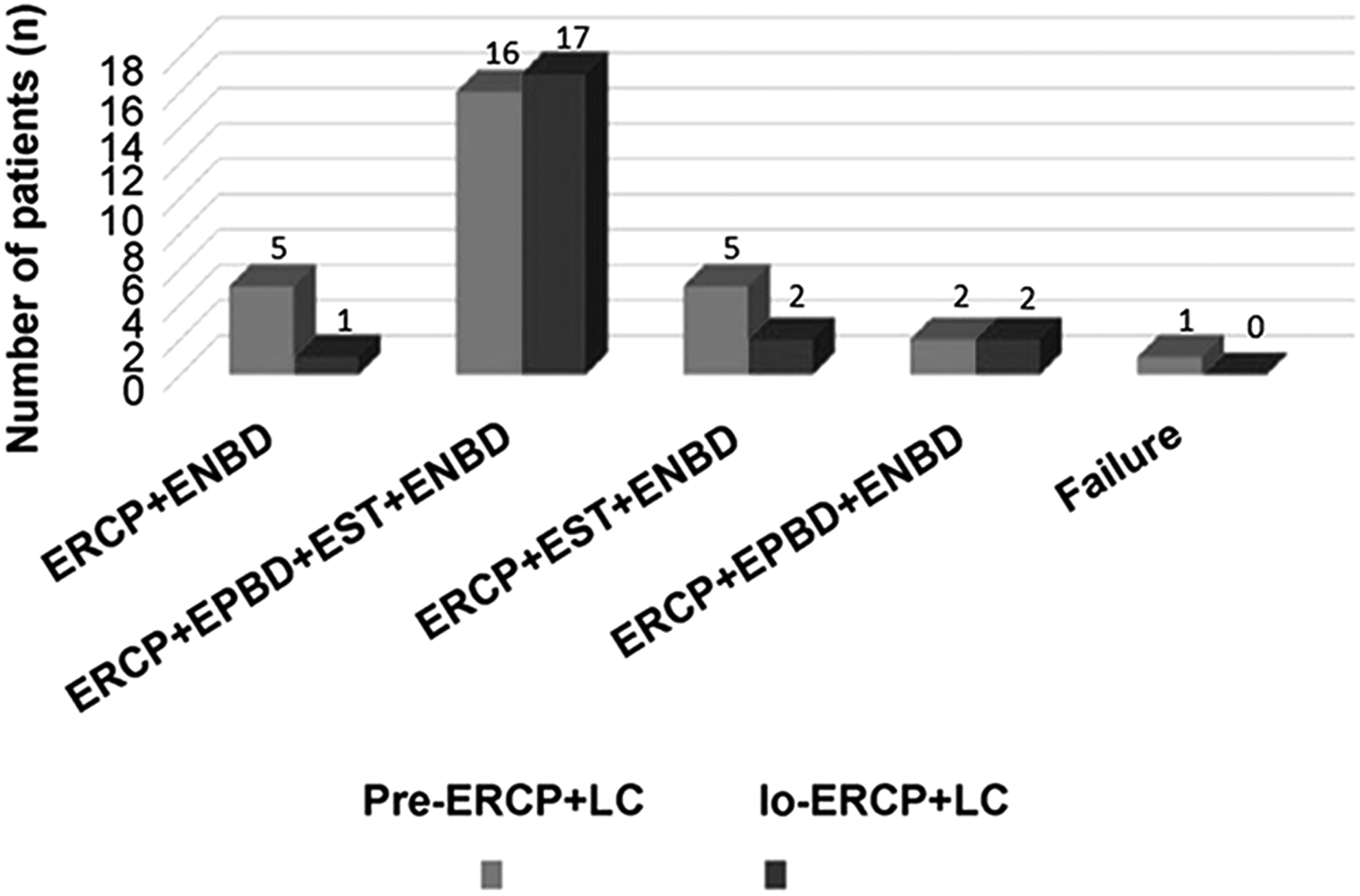
Completion for the operation in two groups. ENBD, endoscopic nasobiliary drainage; EPBD, endoscopic papillary balloon dilation; ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy.
Analysis of operative indicators between two groups
Fifty patients were successfully cleaned out of all stones and 1 patient had residual stones after the operation. The total removal rate of extrahepatic bile duct stone was 98.0% and the residual stone rate is 1.9% (Table 2). There were no significant differences for removal stone rate and residual stone rate between two groups (P > .05).
Comparison of the Operation Index of Patients Between Two Groups
ERCP, endoscopic retrograde cholangiopancreatography; LC, laparoscopic cholecystectomy.
Analysis of postoperative complications
There was no complication associated with laparoscopic or endoscopic surgery, including aspiration, gastrointestinal perforation, acute cholangitis, bile leakage, and bile duct injury, in patients of both groups (Table 3). Meanwhile, PEP and hyperpancreatemia occurred in two groups, and there was no significant difference in the incidence rate (P > .05).
Comparison of the Complications After the Operation Between Two Groups
ERCP, endoscopic retrograde cholangiopancreatography; LC, laparoscopic cholecystectomy; PEP, post-ERCP pancreatitis.
Io-ERCP+LC strategy decreased NRS scoring, reduced surgery cost, and shortened hospitalization time
NRS scoring, surgery cost, and hospitalization time were compared between these two groups (Table 4). And according to these results, efficacy of Io-ERCP+LC strategy was more in those indicators.
Comparison of the Other Indicators After Operation Between Two Groups
ERCP, endoscopic retrograde cholangiopancreatography; LC, laparoscopic cholecystectomy; NRS, numeric rating scale.
Short term follow-up
We followed up the patients 1 week, 1 month, 3 months, and 6 months after operation and the reoccurrence of stones was excluded by using ultrasound examination and CT. The results indicated that all of 51 patients in two groups exhibited no reoccurrence of stones, no appearance of cholangitis, biliary obstruction, and death cases.
Discussion
The LC is the standard treating strategy for cholecystolithiasis. 17 However, when cholecystolithiasis is combined with the common bile duct stones, the conventional treating strategy is open choledocholithotomy, cholecystectomy, and drainage with T-tube. 18 In recent years, with the development of minimally invasive methods, the combination of laparoscopy and duodenoscopy has been proven to be effective for treating gallbladder stones with common bile duct stones. 19 Therefore, the clinical efficacy of the combination of laparoscope and preoperative or intraoperative duodenoscope in the treatment of cholecystolithiasis with choledocholithiasis was analyzed in this study.
Our results showed that there was no significant difference in operation time, intraoperative bleeding, total removal rate of stone, and residual stone rate between the two groups. For the pre-ERCP+LC group, pharynx anesthesia, analgesia, and sedative were conducted to prevent the discomfort symptoms during operation and to enhance tolerance of patients, however, there were still a few patients who were not tolerant during the operation. For the Io-ERCP+LC group, performing the LC before the duodenoscope use under general anesthesia could avoid the tolerance problems of patients and enhance the success rate and efficacy of the double-endoscopes therapy.
For the postoperative complications, the total complication incidence rate was 24.1% in Pre-ERCP+LC group, and 36.4% in Io-ERCP+LC group, which indicates no significant differences (P > .05). No aspiration, gastrointestinal perforation, acute cholangitis, bile leakage, or bile duct injury appeared in both two groups. However, some patients had PEP and hyperpancreatemia after operation in these two groups without significant differences for the incidence rate (P > .05). This result suggests that conducting LC and intraoperative ERCP/EST/EPBD/ENBD in a single session is safe. Alexakis et al. 20 reported that total complication incidence rates of PODL group and IODL group are 16.1% and 19.9%. These rates are lower compared to our findings, which may be associated with the application of indometacin for prevention. The occurrence of PEP is associated with the mechanical damage of duodenal papilla and pancreatic duct caused by the surgery. 21 Therefore, for the prevention of PEP, the practiced surgical techniques and ENBD treatment are necessary factors for patients. Moreover, the complications in two groups may also correlate with the limited number of patients and operative capability of ERCP.
NRS is a common measurement tool that is selected in numerous pain investigations. 22 The NRS, a horizontal-line composed of 11 marks (from 0 to 10), has been extensively applied in patients with the enhanced levels of acute pain or chronic pain. In this study, the NRS scores in Io-ERCP+LC group was significantly lower compared to that of Pre-ERCP+LC group (P < .05). This result suggests that IODL could effectively reduce the pain associated with general anesthesia during the process of operation compared to PODL. Moreover, the surgery cost was also significantly reduced and hospitalization time was shortened in Io-ERCP+LC group compared to pre-ERCP+LC group, which were consistent with the previous study. 23
Although this study received some interesting results, there were still a few limitations. First, the sample size of patients is relatively small in this study. Second, the follow-up time is relatively short and the long-term complications have not been observed. Third, the recurrence rate of bile duct stones and acute cholangitis have not been evaluated and discussed in this study.
In conclusion, the combination of the laparoscope and intraoperative or preoperative duodenoscope is an effective method in treating cholecystolithiasis with choledocholithiasis. These two methods are proven to be safe and feasible and a short period of follow-up shows no reappearance of any complications. IODL has a better result in postoperative pain, surgery cost, and hospitalization time; more important, an increase in patient satisfaction and tolerance of therapy. However, to get more reliable results, more randomized clinical trials with high methodological quality are required.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the National Natural Science Fund of China (Grant No. 81303110), Basic research project of Education Department of Liaoning Province Key Laboratory (Grant No.LZ2015028), and Major projects of clinical diagnosis and treatment in key departments of Liaoning Provincial Health Planning Commission (Grant No. LNCCC-A03-2015).