
Abstract
Abstract
Introduction:
Compared with open surgery, laparoscopic groin hernia repair has been shown to significantly reduce postoperative pain. However, chronic pain remains a problem with the laparoscopic approach, affecting approximately 10% of patients. The purpose of this study was to evaluate clinical outcomes following the use of Parietex ProGrip™ (Covidien, Dublin, Ireland) self-gripping mesh during laparoscopic totally extraperitoneal groin hernia repair.
Materials and Methods:
Data were collected prospectively from 145 male and 15 female patients with 235 inguinal hernias. All patients underwent repair by the laparoscopic totally extraperitoneal approach using Parietex ProGrip mesh. During follow-up ranging from 5 to 24 months, complications, pain score, patient satisfaction, and recurrence were analyzed.
Results:
All patients were discharged on the day of surgery or the next morning. There were no immediate complications or returns to the operating room. Delayed postoperative complications included minor bruising to the genital region (3 cases), hematoma/seroma (1 case), and wound infection (1 case). The mean follow-up was 15 months, at which time there were no reports of hernia recurrence and 99% of patients were satisfied with their hernia repair. One patient (0.63%) reported severe pain (numeric rating scale score of >7), and 4 patients (2.5%) reported intermittent mild pain on exertion.
Conclusions:
The results of this study suggest that the use of a self-gripping mesh during the laparoscopic totally extraperitoneal approach is a promising and effective technique for repairing both primary and recurrent inguinal hernias.
Introduction
G
The Royal College of Surgeons of England recently reviewed the current evidence and now recommends a laparoscopic approach for the following: bilateral hernias; recurrent hernias (if the primary repair was open); any groin hernia in a woman; and hernias in men who are young and active or who have pain as a predominant symptom of their hernia. 2 Although using a laparoscopic approach has been shown to significantly reduce the risk of persistent postoperative pain and numbness, about 10% of patients still experience these symptoms. 1 Using tacks or staples to secure the mesh or repair the peritoneal window during a TAPP repair may contribute to the development of these symptoms.
To address these risks, the peritoneal window can be sutured, or a TEP approach can be used. Various approaches have been tried to avoid the use of tacks to secure the mesh. Some surgeons advocate using no fixation; however, a meta-analysis of the published literature did not demonstrate that this technique reduces the occurrence of postoperative pain, 3 possibly due to the wider dissection required to place a larger mesh. Glue fixation is another alternative, and a meta-analysis of a small number of studies comparing this with tacker fixation concluded a reduction in postoperative pain. However, glue is more expensive than tackers and therefore not a viable option for many surgical departments. 4
In an effort to reduce postoperative discomfort, reduce costs, and maintain a low recurrence rate, we have used Parietex ProGrip™ (Covidien, Dublin, Ireland), a self-gripping mesh, during TEP repairs. This lightweight monofilament polyester mesh is self-gripping and semi-reabsorbable. It consists of two components: a hydrophilic, monofilament polyester, which provides rapid and effective tissue in-growth, and an absorbable polylactic acid (PLA) gripping system. The monofilament composition and the large pore size of the mesh are thought to reduce foreign body reaction and to aid in optimal tissue integration. The gripping system consists of a series of very small PLA grips giving the mesh self-adhesive properties. The grips are biodegradable, and when the tissue grows into the mesh, the grips break down, leading to a reduction in the overall tension and chronic strain of the foreign body.
The mesh has historically been used in open repairs, producing results comparable to a traditional Lichtenstein repair 5 with a low pain and recurrence profile at least in the short term. Early studies evaluating the use of this mesh during laparoscopic TAPP repairs have shown the mesh to be safe with a lower postoperative pain when compared with tacker fixation.6,7
In November 2011, we began selectively using the TEP technique with self-gripping mesh. Our initial results are presented in this article.
Materials and Methods
Patient population
Data were collected prospectively for consecutive patients undergoing elective laparoscopic inguinal hernia repair in our unit (two clinical centers in Sydney, NSW, Australia) between November 2011 and July 2013. All patients undergoing laparoscopic inguinal hernia repair at our clinical centers were treated using Parietex ProGrip, as per our standard of care. Patients who also had previously undergone open inguinal hernia repairs presenting with recurrence were included in the study. Patients with previous laparoscopic inguinal hernia surgery, who had undergone hernia repair as part of an emergency procedure, or who had incarcerated hernias were excluded from the study (Table 1).
Data collection
Data were collected as part of a prospective database. Preoperative data included patient demographics (age and gender), unilateral versus bilateral hernias, primary repair or surgery for recurrent hernia, body mass index, and level of premorbid physical activity. Perioperative data included operating time and length of stay. Postoperative data collected included postoperative complications, hernia recurrence, pain score on a numeric rating scale (NRS) (from 0 to 10), 8 and patient satisfaction. Hernia recurrence was defined as the clinical or radiological presence of a hernia in the postoperative period.
The study included a telephone follow-up clinic using a questionnaire-based proforma that assessed complications, pain, recurrence, and patient satisfaction. All authors collaborated on the design of the questionnaire. Telephone follow-ups were conducted by the authors (J.O., V.C., K.H., and W.H.). J.O. made 125 telephone calls, and the remaining authors made a total of 35 calls. The surgeon (K.L.) did not perform any telephone follow-ups. A follow-up visit was scheduled for any patient complaining of a recurrence or severe pain in order to conduct a physical and radiological examination as required.
The study was conducted in accordance with approval from the appropriate human research and ethics committee (HREC reference number 12/167 LNR/12/POWH/32).
Surgical technique
All patients underwent a standard TEP approach with two 5-mm ports and balloon-assisted dissection through a 12-mm camera port. Careful dissection was performed in the usual fashion in order to prepare the preperitoneal space adequately (Fig. 1). Prior to introduction into the pre-peritoneal cavity, the 15- × 15-cm mesh was trimmed to 12 × 15 cm and rolled from both the superior and inferior margins inward toward the middle. The inferior edge was rolled tightly, whereas the superior edge was rolled loosely. The rolled mesh was then marked transversely with a surgical pen along both rolled edges and longitudinally two-thirds along the intended medial border to aid orientation once inside the preperitoneal space. The longitudinal mark signified where the mesh should be positioned over the deep inguinal ring to allow sufficient medial coverage. The mesh was then introduced through the 12-mm port and positioned over the deep inguinal ring over the previously marked point, with the medial edge overlapping the public tubercle toward the midline (Fig. 2). The inferior border of the mesh was unrolled, first laterally, then medially, to ensure that it followed the contour of the groin and pelvis and to allow easier unrolling of the superior edge of the mesh (Fig. 3). Once the mesh was positioned satisfactorily with coverage of all defects, the preperitoneal space was deflated under vision (Fig. 4). Initial placement was crucial, as there is little ability to reposition once the mesh has been unrolled. For large direct groin hernia defects the complete 15- × 15-cm piece of mesh was used with sufficient medial coverage to obviate the need for fixation.
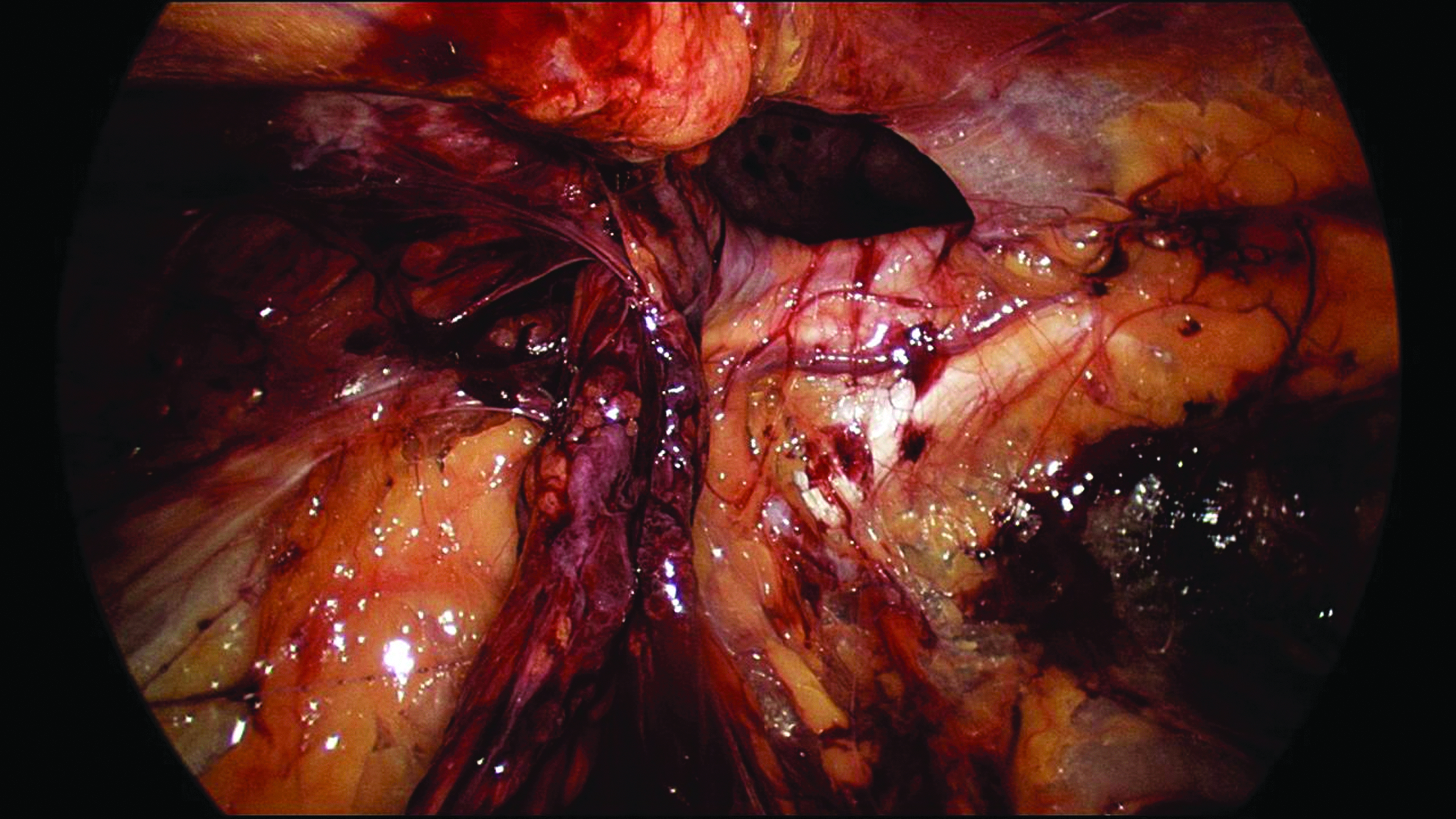
Dissection of the preperitoneal space.
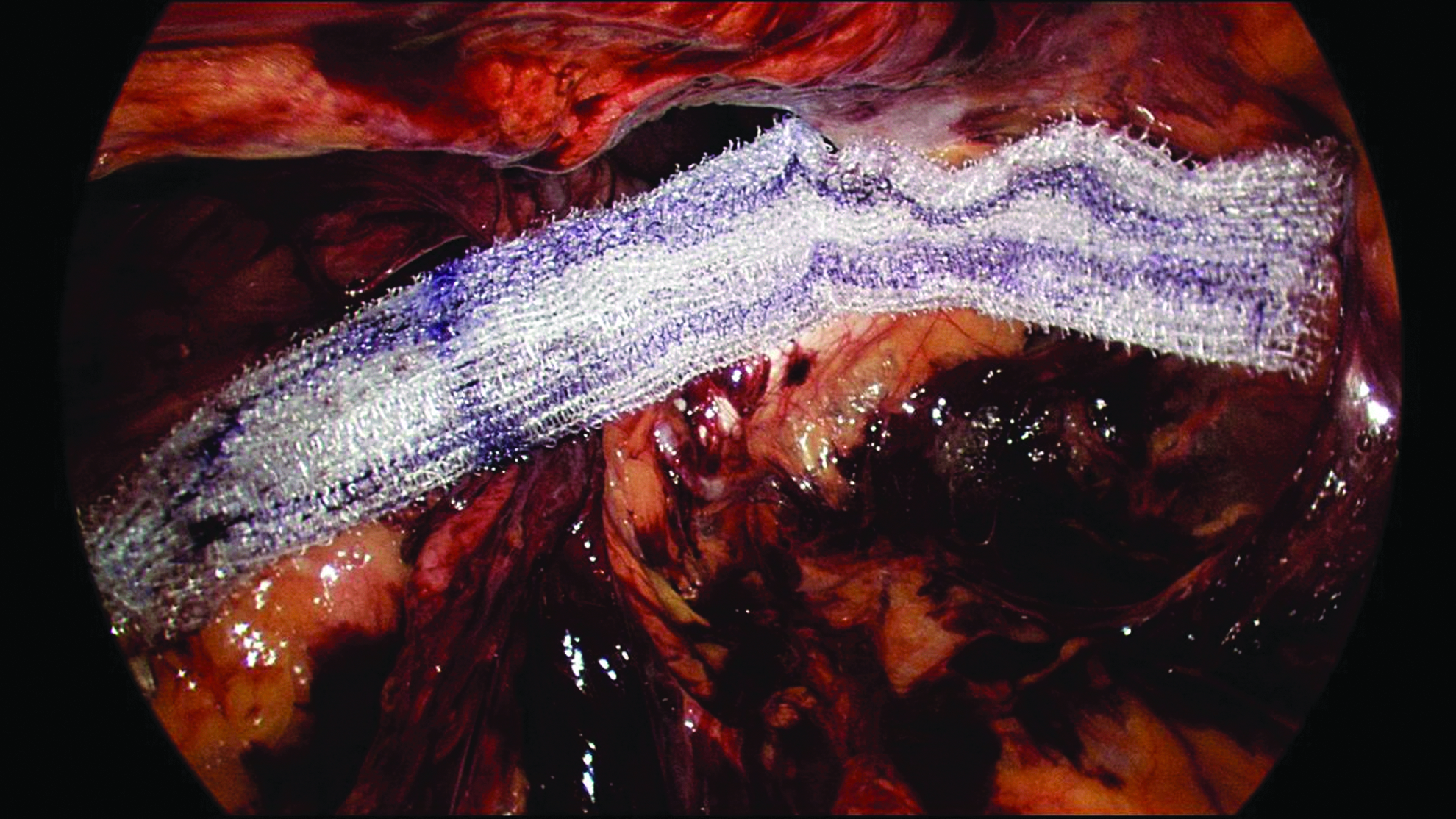
Positioning of the mesh over the deep inguinal ring.
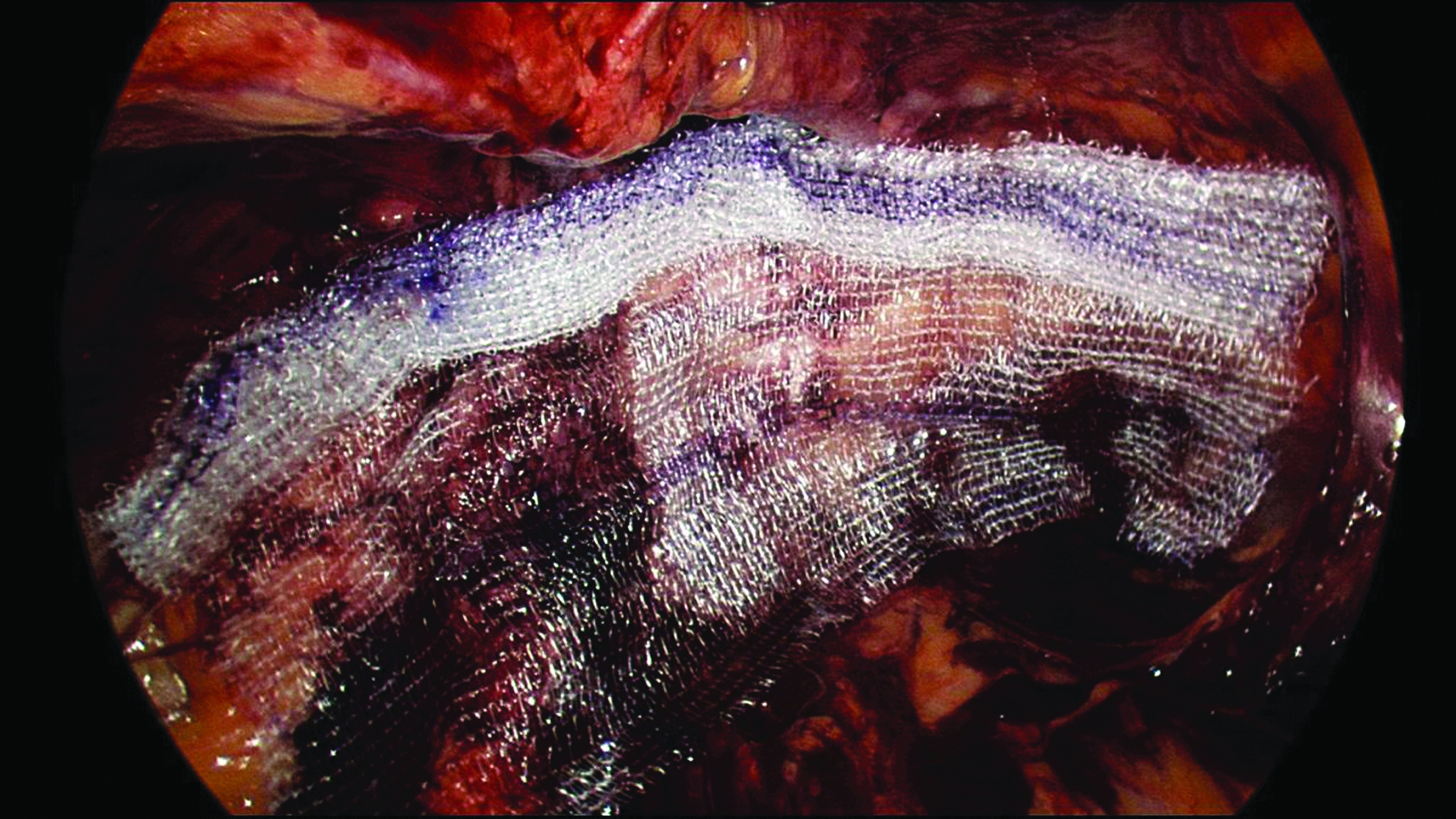
Unrolling of the mesh following the contour of the groin and pelvis.
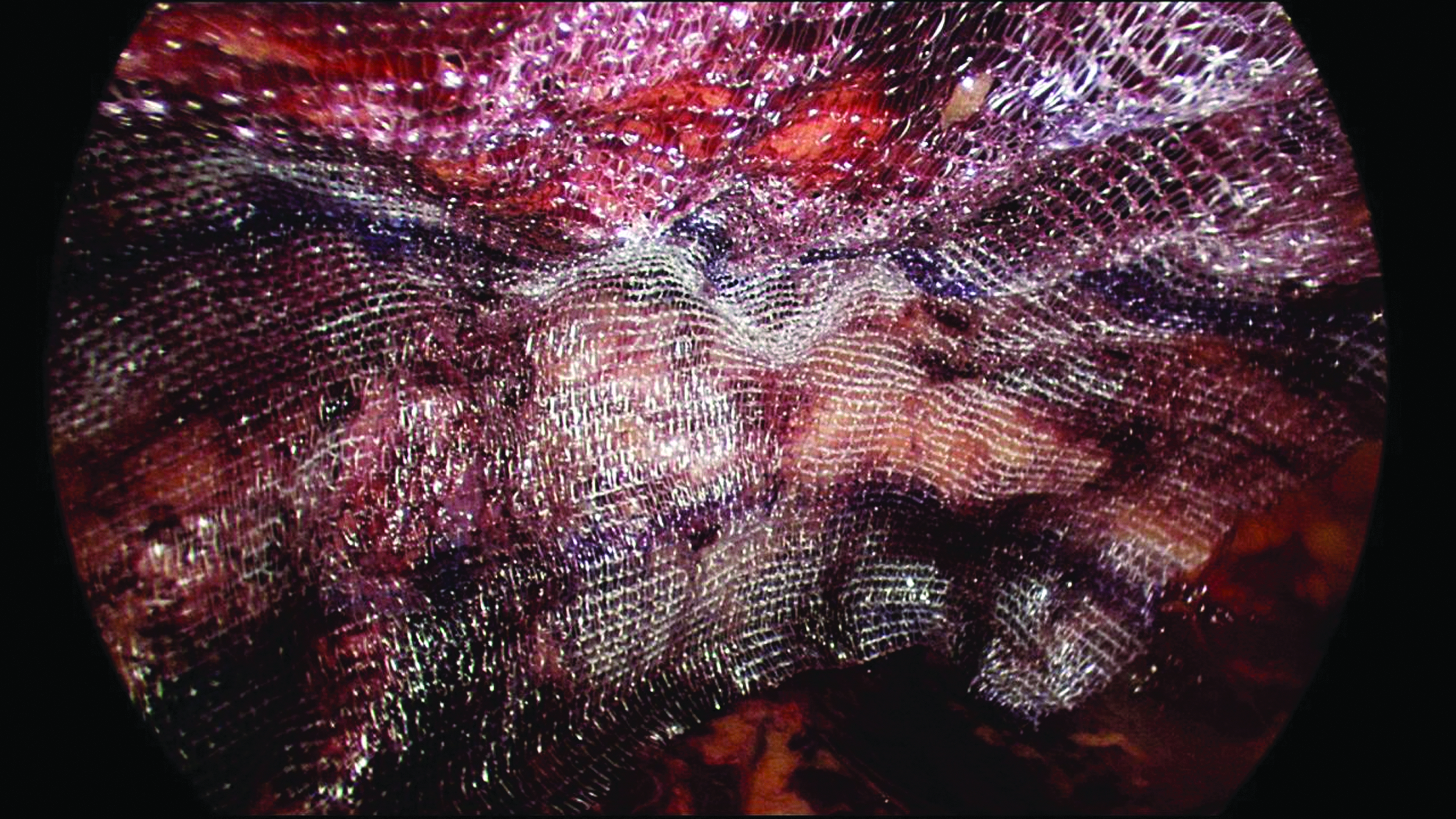
Deflation of the preperitoneal space following satisfactory positioning of the mesh.
Statistical analysis
Data were described as frequency (percentage) for categorical variables and mean (standard deviation) for continuous variables. As there were no hernia recurrences, no statistical test was performed to compare patients with and without hernia recurrence at follow-up. Continuous variables were compared according to gender using the Mann–Whitney test, and qualitative variables were compared using Fisher's exact test. Statistical analysis was performed and analyzed by biostatisticians.
Results
Patient demographics and hernia data
One hundred sixty patients underwent 235 laparoscopic TEP hernia repairs using Parietex ProGrip mesh in the study period. All procedures were performed by or under the direct supervision of the lead surgeon (K.L.). All patients had at least 3 months of follow-up. The demographics and operative data are summarized in Table 2.
Data are mean ± standard deviation values (range) or number (%) as indicated.
Most patients had a sedentary job or lifestyle or were retired or unemployed, and they performed little or no exertion on a daily basis. Hours of physical activity outside of work varied, with the most common activities being walking, golf, and other exercise.
Surgical data
The mean operative time was 32.5 ± 18.6 minutes. Bilateral inguinal hernia repair resulted in longer operating time regardless of hernia type. There was a considerable reduction in operative time following the first 50 hernia repairs, consistent with the learning curve resulting from the use of a new mesh technique.
Mean length of hospital stay was 11.04 ± 6 hours and had no relation to gender, side, type of hernia, or surgeon experience. The majority of patients went home on the day of surgery (53%), whereas the remaining were discharged on the first postoperative day (47%) mainly due to patient preference in a private hospital setting.
Postoperative complications
Immediate and delayed postoperative complications were uncommon and are summarized in Table 3. The mean follow-up was 15 months (range, 5–24 months). Results from the telephone follow-up survey demonstrated that 96.8% of patients reported no or low pain. Mild intermittent pain (NRS 1–3) was experienced by 2.5% of patients, and 0.63% (1 patient) complained of severe pain. The patient who complained of severe pain (NRS score of 7) was one of our first patients and reported this at his 3-month follow-up appointment. The patient noted intermittent pain that affected the umbilical region when bending and sitting but was not present at rest. The pain had resolved by 24 months.
No life-threatening or serious adverse events such as hemorrhage or return to the operating room were reported.
Hernia recurrence
Of the 160 patients who were contacted and who completed the survey, 1 patient was asked to attend a physical examination to determine the presence of hernia recurrence. Following careful clinical examination and radiological assessment with dynamic ultrasound of the inguinal region, no evidence of recurrence was found. A hematoma/seroma was diagnosed and treated conservatively.
Patient satisfaction
Overall, 99.3% of patients were satisfied with their hernia operation and would recommend this operative technique to friends or relatives with an inguinal hernia. There were no statistically significant differences in satisfaction based on the side of surgery, gender, or the presence or absence of postoperative complications.
Discussion
Several mesh fixation techniques have been proposed over the past few years for laparoscopic groin hernia repair, ranging from permanent and absorbable tacks, to biological and nonbiological glues, to no fixation. Each method has advantages and disadvantages in several measured outcomes. The use of self-gripping mesh in the open repair of groin hernias is now accepted as a viable approach 5 with satisfactory results achieved with regard to pain and recurrence rates in the short term.9 The success with its use in open surgery has led to its application in the treatment of groin hernias using a laparoscopic TAPP approach as described by Birk et al. 6 and Fumagalli Romario et al. 7
In this article we present our initial results with the laparoscopic TEP approach for repair of groin hernias using a self-gripping mesh. The majority of patients in our study were males, and a majority of repairs were unilateral (although bilateral repairs did constitute nearly half of the cases). Operative times and length of stay were competitive compared with the TAPP approach and improved as increasing numbers of cases were performed. Immediate and delayed postoperative complications were uncommon, and no hernia recurrences were recorded at 12 months of follow-up. Overall, the vast majority of patients were satisfied with the surgery, and all patients would recommend the procedure to family and friends. The patient-reported postoperative pain scores compared very favorably with the published literature,6,7 which may indicate that the use of a self-gripping mesh is associated with reduced postoperative pain. Our results suggest that laparoscopic TEP groin hernia repair with self-gripping mesh is a safe and promising technique.
A thorough understanding of preperitoneal anatomy is crucial in the initial placement of self-gripping mesh in a TEP approach, due to the fairly permanent nature of the fixation once it is in contact with tissue. The mesh adheres when placed in contact with connective tissue and is difficult to reposition. The key to the successful use of this mesh is accurate placement of the mesh along the line of the ilioinguinal tract followed by gently rolling the mesh out inferiorly and superiorly as described in our surgical technique. The additional benefit of using Parietex ProGrip over standard nongripping mesh and a tacking device such as ProTack™ (Covidien) is a reduced cost in consumables. Although the self-gripping mesh is slightly more expensive than standard mesh, there is an overall reduction in cost of around AUD $379/€260/US $356 (AUD $323 in a bilateral case). Due to the need for precise initial placement it may be inadvisable for a surgeon with little laparoscopic experience to use this mesh unless supervised by a surgeon with suitable experience. Several of our cases were performed by surgeons-in-training under the supervision of the lead surgeon.
Despite the many advantages of using self-gripping mesh, there were some limitations. The mesh was not ideal for use if the dissected space was relatively small, as it made unrolling the mesh more difficult. Additionally, the mesh was not ideal if the dissection was very difficult, or if there was a significant breach of the peritoneum. Breaches of the peritoneum rarely occurred when a gentle dissection technique was used, and small holes were repaired with surgical clips when they occurred.
In future studies comparison of the self-gripping mesh with standard mesh with fixation may allow a more accurate evaluation of the advantages of the technique described in this article for the laparoscopic repair of groin hernias. Longer clinical follow-up and examination of specific types and sizes of hernia defects may determine if the self-gripping mesh is superior to fixation across the range of groin hernias a surgeon may encounter.
Conclusions
To our knowledge this is the first report that has evaluated the use of Parietex ProGrip mesh in laparoscopic groin hernia repair using the TEP approach and is the largest series using self-gripping mesh in laparoscopic groin hernia repair. The results of this study suggest that, in experienced hands, groin hernia surgery performed with the TEP approach using self-gripping mesh is feasible and efficacious for both unilateral and bilateral repairs, resulting in minimal chronic pain or hernia recurrence. We believe that this is a significant advance in the laparoscopic approach to groin hernia surgery, providing a viable, alternative use of self-gripping mesh. However, longer-term randomized data are required to better assess the benefits of this approach compared with the other techniques available.
Footnotes
Acknowledgments
Editorial support was provided by Theresa K. Griffin, DC, Covidien.
Disclosure Statement
Nonmonetary provision of editorial support was provided by a Covidien employed medical writer. No competing financial interests exist.
This article was drafted by J.O. and reviewed critically by all authors. The decision to write and submit the article was made by the authors.