
Abstract
Women face unique and multifaceted challenges throughout their lifespans, shaped by biological, societal, and health care-related factors. These challenges have led to gender disparities in disease burden, access to care, and representation in medical research, underscoring the need to increase targeted investments in women’s health. Historically, research on diseases that disproportionately affect women has been underfunded, hindering progress in closing gender health gaps. In March 2024, the President of the United States signed an Executive Order on Women’s Health Research and Innovation, signaling a new commitment by the federal government to prioritize women’s health research and address these disparities. The Society for Women’s Health Research (SWHR) has consistently led the charge to identify research gaps and advocate for evidence-based initiatives to improve the health and well-being of women. In celebration of its 35th anniversary, SWHR introduces a 2025 Women’s Health Research Agenda, which outlines key priorities in the areas of uterine health, autoimmune disease, and cardiometabolic health. This agenda serves as a strategic roadmap for stakeholders to engage with critical areas of women’s health, fostering collaboration and accelerating research to address the unmet needs of women across the lifespan.
Introduction
Women face unique challenges over the course of their lifespans, including but not limited to biological sex differences that contribute to disease disparities, underrepresentation in medical research (as participants and scientists), gender-related expectations and societal norms, family caregiving and health care decision-making, and discriminatory practice and other access barriers to health care. 1 –3 These challenges present ample opportunities to turn research, health care, and policy attention toward increasing awareness and investment in improving the health of women across their lifespan.
Historically, research on diseases and conditions that predominately affect women has been underfunded, thwarting our ability to close gender health gaps. 4 With less than 11% of the National Institutes of Health (NIH) budget funding research across women’s health topics, there are many opportunities to increase efforts in the study of sex differences and the health of women (Table 1). 5 On March 18, 2024, U.S. President Joe Biden signed an Executive Order on Women’s Health Research and Innovation (EO 14120)—part of the first-ever White House initiative on women’s health research that gave specific directives prompting prioritization and integration of women’s health across federal agency portfolios and budgets. Throughout 2024, Congress supported funding for research in women’s health on a bipartisan basis, as the women’s health community witnessed strong commitments from the Advanced Research Projects Agency for Health, NIH Office of the Director, National Science Foundation, and Department of Defense, among others. As another fiscal year takes shape, it is important to continue efforts to prioritize and integrate women’s health research across the public and private sectors to maintain momentum in the progress that organizations like the Society for Women’s Health Research (SWHR) and other institutions have been working toward for decades.
NIH Categorical Spending, FY2020–FY2024 (Dollars in Millions and Rounded)
Mortality: Figures for mortality data are drawn from the National Vital Statistics System and indicate the number of deaths in which a particular disease or condition was mentioned on a deceased individual’s death certificate.
NIH, National Institutes of Health.
SWHR is dedicated to advancing women’s health through science, policy, and education while promoting research on sex differences to optimize women’s health. Since its establishment in 1990, SWHR has been the leading voice on identifying research gaps and unmet needs in diseases and conditions that disproportionately, differently, or exclusively affect women and convening partners across research, health care, and advocacy communities to action evidence-based initiatives that galvanize change for women’s health and well-being. SWHR is invested in a wide range of topics that span women’s health, including autoimmune diseases, eye health, gynecological health, healthy aging, infectious diseases, liver health, maternal health, pain, sleep, and technology innovations.
As we celebrate our 35th anniversary year, SWHR is pleased to introduce a Women’s Health Research Agenda to highlight persistent areas of need in women’s health and to serve as a roadmap for stakeholders to pinpoint where they might initiate engagement or increase current efforts. The 2025 Agenda will focus on uterine health, autoimmune disease, and cardiometabolic health, with special emphasis on uterine fibroids, lupus, and metabolism in women (Fig. 1). Our recommendations are based on reviews of the state of science in each area, as well as guidance from years of work and ongoing engagement with subject matter experts in our interdisciplinary science and policy networks.
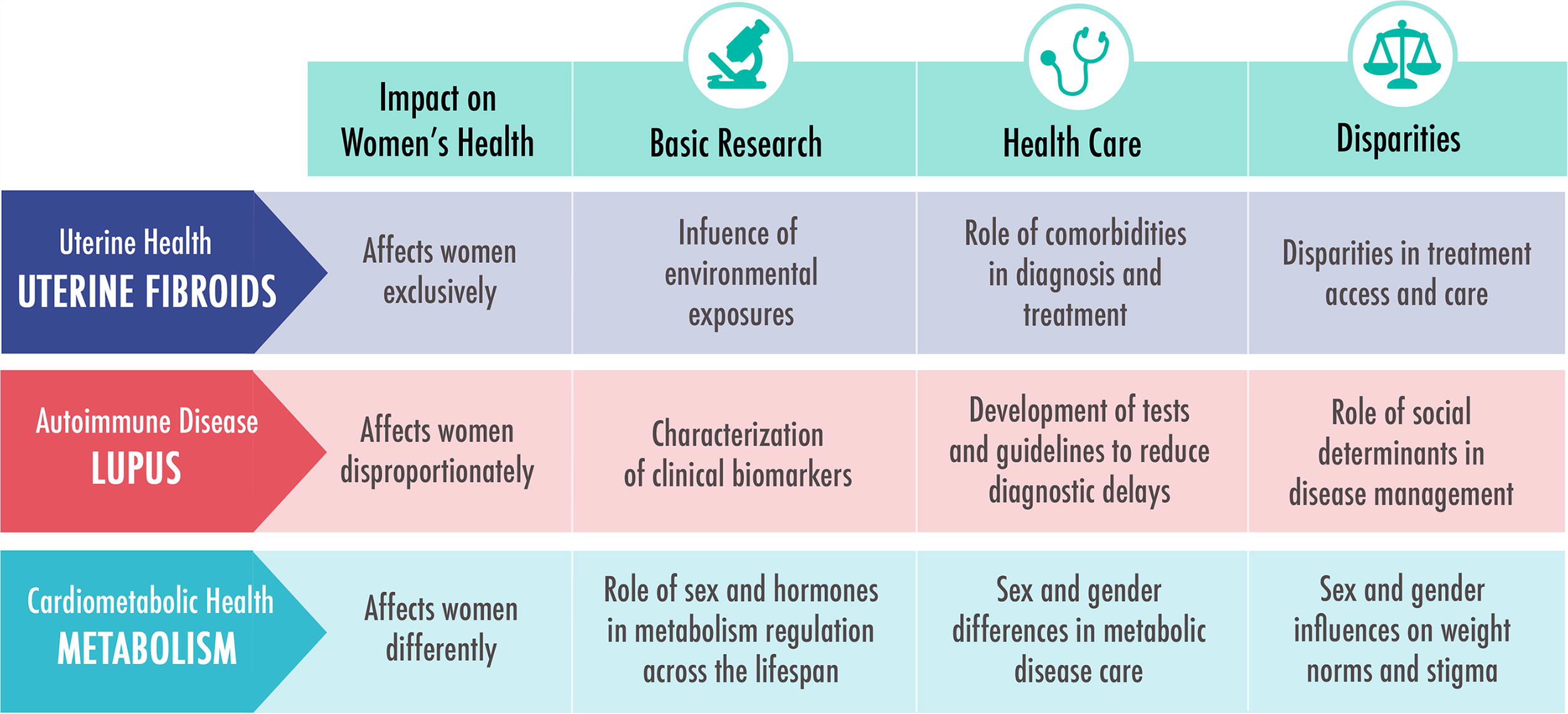
SWHR women’s health research agenda focus areas, 2025–2026. SWHR, Society for Women’s Health Research.
Agenda Overview
Uterine health refers to the overall health of the uterus, including the structural integrity and function of the female reproductive tract, in general, and during menstruation, implantation, gestation, and labor. Many uterine health conditions are characterized by irregular menses, abnormal menstrual bleeding, pelvic and lower back pain, difficulty with urination, or pregnancy challenges. These conditions, such as uterine fibroids, endometriosis, cervical or endometrial cancers, and heavy menstrual bleeding, exclusively affect women (or individuals assigned female at birth).
Uterine fibroids are one of the most common gynecological conditions, affecting an estimated 26 million women, ages 15–50, in the United States. 6,7 Despite their pervasiveness, many women go undiagnosed or may not seek medical care for their symptoms. Furthermore, much remains unknown about the causes of fibroids and the full scope of impact its current treatment options have on fertility. With only 0.03% of the NIH budget funding uterine fibroids research in 2024, our understanding of uterine fibroids will remain limited (Table 1). Increased research investment could accelerate progress toward elucidating the influence of environmental exposures on disease onset and progression, reducing risk and managing treatment of comorbid conditions, and eliminating disparities in the age of onset and symptom severity across different populations of women (Fig. 1).
Autoimmune diseases are chronic and often life-altering conditions that develop when the immune system mistakenly attacks the body’s own healthy organs, tissues, and cells. Autoimmune diseases affect up to 8% of the U.S. population, and studies suggest that the prevalence of autoimmune biomarkers is increasing. The Autoimmune Association has estimated more than $100 billion in annual direct costs associated with autoimmune disease health care in the United States, and globally, cases are continuing to rise by 3–9% each year. 8,9 There are more than 100 classified autoimmune diseases, and 80% of cases are diagnosed in women. Sex differences in autoimmune diseases are widely known, with disproportionate disease prevalence and burden documented in rheumatoid arthritis, multiple sclerosis, thyroid diseases, and lupus. 10
Lupus is characterized by widespread inflammation and symptoms throughout the body that often result in organ tissue damage—most commonly in the joints, skin, brain, lungs, kidneys, and blood vessels. Of the 1.5 million Americans with lupus, 90% are women ages 15–44 years. 11 African American and Hispanic women are 3 to 4 times more likely to develop lupus than White women. 12 Estrogen hormone levels have been known to trigger disease flares and the chronic inflammation and organ dysfunction associated with lupus can result in serious complications and comorbid health conditions. 13 Because there is no cure for lupus, patients depend on early diagnosis and treatment to manage symptoms and slow the progression of disease. Based on gaps in research identified by SWHR, efforts should focus on characterizing clinical biomarkers of lupus, developing tests and guidelines to reduce diagnostic delays, and elucidating social determinants of health disparities in disease management (Fig. 1).
Cardiometabolic health describes the combination of factors that affect the intersection between the body’s cardiovascular and metabolic systems. Shared risk factors for cardiometabolic diseases include high blood pressure, overweight, high cholesterol, and smoking and alcohol use, which can lead to insulin resistance (metabolic syndrome), cardiovascular disease (CVD), obesity, and type 2 diabetes. Disparities in cardiometabolic health have been reported in sex, race, and age. Body fatness and adipose tissue distribution are major contributors to obesity, and differences between men and women have been well-documented in their pathway to developing a metabolic disease throughout the life course. 14 For example, waist circumference and dyslipidemia pose a higher risk for metabolic disease and heart disease in women compared to men. 15 In addition, while men have a higher prevalence of hypertension before age 60, the disparity shifts towards women after age 60. 16
Metabolism is defined as the sum of chemical reactions that occur throughout the body’s cells to provide the body with energy—converting nutrients into energy for cellular processes such as building, repair, and waste removal. Metabolism and metabolic remodeling are critical for cardiovascular health, as CVD is the leading cause of death for both men and women in the United States and globally. Unfortunately, optimal metabolic function (homeostasis) is under constant flux due to genetics, hormones, and environmental exposures, among other factors. Sex differences in energy balance are affected by age and hormone transitions such as puberty, pregnancy, and menopause throughout the lifespan. Moreover, sex and hormones influence energy storage and macromolecule utilization preference; estrogen promotes fat storage and insulin sensitivity in women, and testosterone promotes fat burning and muscle preservation in men. 14
While inherited metabolic diseases are relatively rare, acquired metabolic diseases, such as non-alcoholic fatty liver disease, obesity, and osteoporosis, have become more common in the 21st century. 17 There is no assigned category that tracks NIH research funding for general metabolism; however, there is a significant investment in obesity research (Table 1). It should be noted that this work is not dedicated to the study of women’s health, as only 228 (8.6%) projects—accounting for $92.3 million or 7.8% of the 2023 obesity research dollars—indicated a focus on sex or gender in a relevant key term search of the portfolio’s project titles. Targeted research efforts are needed to further understand the role of sex and hormones in metabolism regulation throughout the health span and different life stages, sex and gender influences on norms and stigma surrounding weight that may affect behavior toward modifiable risk factors, and sex and gender differences in the diagnosis and treatment of overweight and obesity (Fig. 1).
Uterine Fibroids
Although benign, uterine fibroids are the most common tumors in women—present in 70% of White women and over 80% of Black women. 7 Only 25–50% of women will experience symptoms, such as heavy menstrual bleeding, pain, anemia, and infertility, prompting them to seek medical care. Women with symptomatic fibroids can experience significant disease burden and reduced quality of life, even throughout their treatment journey. Consequently, the economic burden of symptomatic fibroids in the United States is estimated at $5.9–34.4 billion in total costs annually. 18 This range reflects underreporting and discrepancies that women experience in navigating accurate and timely diagnoses, accessing treatment options, and managing disease complications and comorbidities. Despite efforts to interpret some of the race-related disparities of fibroid pathology, a study of genetic and molecular differences in tumors in Black and White women was unable to explain the increased prevalence or disease burden in Black women. 19 Moreover, very few studies have focused on Hispanic, Asian, and other women of color, leaving significant gaps in understanding how to treat diverse populations of women living with fibroids. 20 As such, studies to identify modifiable risk factors might provide answers to the increased disease burden in women of color.
Environmental exposures
The exposome is a concept that describes all the environmental exposures a person experiences throughout their life course and how they affect health. Despite being a widely accepted paradigm for studying chronic diseases, the role of environmental risk factors on uterine fibroid incidence and disparities remains understudied. 21 Studies have reported that exposure to endocrine-disrupting chemicals, even in utero, can increase the risk of uterine fibroids, affecting the age of onset and disease severity. 22 Furthermore, disparities in exposure risk associated with local environment and societal pressures have been documented concerning women from different racial and ethnic groups. For example, Black women have higher levels of exposure to phthalates and bisphenol A compared with Hispanic, White, and other groups. Black women also tend to experience an earlier age at onset and more severe symptoms, despite fibroids’ prevalence being common in both White women (70%) and Black women (> 80%). 23 Given these individual knowns, chemical influences on fibroids have still not been adequately investigated to mitigate the disease burden in women, particularly women of color.
Comorbidities
Diagnosing fibroids can be challenging because its typical symptoms of heavy or irregular menstrual bleeding, pelvic and back pain, frequent urination, and infertility overlap with symptoms of other gynecological conditions, such as endometriosis and adenomyosis. Furthermore, these conditions can also co-occur with fibroids. Comorbidity with endometriosis is well-documented, although retrospective study reports range from 12% of fibroids patients having confirmed endometriosis to 57.9% comorbidity and higher. 24 Genetic underpinnings of the two diseases, however, are not as well understood. Recently, genome-wide association studies have identified a set of risk factor alleles for the development of fibroids, which include WNT4 and CDC42 variants on chromosome 1 and SYNE1 and ESR1 variants on chromosome 6. 25,26 A better understanding of the genetic overlap between gynecological diseases might improve our ability to coordinate preventive care and holistic treatments for patients living with comorbidities.
Mental health is an important consideration for patients with chronic health conditions. While literature about evaluating the risk of mental health conditions in fibroids patients is limited, studies have indicated that women diagnosed with fibroids have a higher rate of depression and anxiety, particularly those who experience pain symptoms or had a hysterectomy. 27 Further assessment of this association by demographics, disease manifestation, and treatment journey will be useful in mitigating risk for psychosocial incidents and sequelae.
Disparities in treatment access and utilization
Hysterectomy is considered the only curative treatment for fibroids; fibroids account for more than 40–60% of all hysterectomies. 20 While this invasive surgical procedure presents better short-term outcomes, in the longer term, hysterectomy is associated with an increased risk of CVD, fracture risk, and neurological issues. 28,29 African American women are 2.4 times more likely to undergo a hysterectomy, although studies report that they often prefer less invasive options. 30,31 This high rate of hysterectomy among a population that also has an increased risk of CVD and certain neurological conditions in older age raises concern and a need to identify and offer treatment options with better long-term outcomes. Racial biases continue to shape the way health care providers and patients navigate disease management across different communities, further exacerbating the disparities in women of color.
Age and parity are also factors that drive fibroid treatment option recommendations and utilization. Traditionally, younger women have been recommended fertility-preserving treatment options, whereas women 40s or older are more often offered a hysterectomy, with the nearing of menopause. Clinical conversations with all patients must truly emulate shared decision-making, driven by individual patient experiences and needs, rather than age or racial biases and assumptions. Studying the impact of these biases on patient engagement and collecting comparative data on treatment options and their outcomes can provide the evidence base needed to develop interventions that better predict patient responses to treatments and that minimize psychosocial burden, financial toxicity, and long-term adverse health outcomes.
Lupus
Systemic lupus erythematosus (SLE) affects multiple parts of the body, accounting for 70% of all lupus cases. 32 Other forms of lupus include cutaneous lupus erythematosus, which primarily affects the skin; a temporary drug-induced lupus that can develop from reactions to certain medications; and neonatal lupus, a rare form of lupus that occurs when infants acquire autoantibodies from a mother with SLE. The symptoms of neonatal lupus typically resolve within 6 months after birth and do not reoccur; however, in very rare cases, congenital heart block can be a serious complication that presents in utero. 33,34 Many of the symptoms of lupus, including fatigue, joint pain and swelling, light sensitivity, and skin rash, are similar to other rheumatic diseases, such as rheumatoid arthritis and fibromyalgia. As a result, SLE is often incorrectly or delayed in its diagnosis. Basic and clinical research must address the pressing need to equip health care providers with methods to better recognize indications of lupus and arrive earlier at an accurate diagnosis.
Clinical biomarkers for SLE
Due to the complex pathology and diverse clinical indications of SLE, the use of a single biomarker is insufficient to address the diagnostic challenges of lupus. While the literature reports several novel biomarkers for potential use in diagnosing and monitoring SLE, their use in clinical practice is limited. 35 Validation of the specificity, sensitivity, accuracy, and reproducibility of many of these promising biomarkers is lacking. 36
Traditional markers for lupus include autoantibodies—as their production and the formation of immune complexes are key trademarks of SLE. 35 Antinuclear antibody is the most common test for SLE; however, it only measures immune system activity, not SLE specifically. On the contrary, anti-double stranded DNA is a strong positive indicator of lupus, with high specificity, but low sensitivity. 37 Elucidating molecular mechanisms of disease and leveraging new and traditional disease-specific biomarkers would make strides toward improving the diagnosis of lupus.
Diagnostic tests and guidelines
There is no single diagnostic test for lupus, so diagnosis often relies on a process of elimination and meeting multiple criteria to indicate SLE. The patient journey often includes a clinical examination, medical history, blood and urine tests, biopsies, and/or imaging. Up to 76% of patients with lupus had their early symptoms misdiagnosed. 38 Delays in diagnosis can lead to cardiovascular complications, rheumatic and kidney diseases, and osteoporosis, not to mention patient fatigue in managing daily living and engaging the health care system. 39
The European League Against Rheumatism and the American College of Rheumatology recently launched classification criteria for SLE. 40 While advancing the field in many ways, these strictly clinical criteria provide specificity to better illustrate and predict SLE in patients but have limited diagnostic capability. This conservative list does not offer enough items with the level of sensitivity that is required to permit clinicians to diagnose disease. 41 Studies that can effectively demonstrate connections between different organ manifestations of SLE and validate biomarkers that can link immunological and clinical manifestations could bridge critical gaps in the potential use of classification criteria toward definitive diagnoses of SLE.
Disparities in disease management
With an overwhelming gender disparity in lupus affecting women compared with men, women of color are also more likely to have more severe disease, worse health outcomes, and higher mortality from SLE. Even with generally improved patient outcomes over the decades, race and ethnicity remain independent predictors for worse disease outcomes for SLE. 42 These disparities are perpetuated due to lower socioeconomic status, racial discrimination and negative patient experiences navigating the health care system, and a lack of representation in clinical trials for women from racial and ethnic minority backgrounds. 43 –45 Other determinants of disease that have been noted include environmental factors, such as pollutant exposures that contribute to epigenetic changes which can affect age of onset and disease severity. 46 Research that can not only elucidate these issues but also aim to provide solutions from an individual to a societal level is critical to addressing this need. 47
Maternal morbidity, for which disparities and inequities are well-documented, is another key consideration for lupus, as pregnant women with SLE are more likely to experience adverse pregnancy outcomes and fetal complications. 48 Studies that focus on the perinatal pharmacokinetics of lupus therapeutics would significantly improve health care options for pregnant patients challenged with managing both their autoimmune health and maternal health throughout their reproductive years.
Metabolism
Metabolic regulation across the lifespan
Sex is a biological variable that affects energy balance and body composition. Metabolic adaptation during exercise differs between the sexes, with women preferentially oxidizing lipids compared to men who utilize carbohydrates as the predominant fuel source. 49 In women, both chronological and ovarian aging contribute to substantial changes in fat and skeletal muscle mass, waist circumference, and body fat distribution. 50 Women uniquely have additional risk for metabolic syndrome due to factors such as pregnancy-related weight gain and retention, hormonal contraceptive use, and menopause. 15
Sex hormones play a role in insulin sensitivity. Estrogen, the primary female sex hormone, demonstrates protective effects on insulin sensitivity, favoring women during their reproductive years, whereas insulin resistance is generally more prevalent in men during this life stage. However, after menopause, when estrogen levels decline, the incidence of insulin resistance in women increases and becomes more comparable to that of their male counterparts. 51 The implications of older-age insulin resistance, metabolic decline, and altered body composition pose significant potential health risks for women as they age. While menopause and its estrogen depletion are inevitable life experiences for women, understanding the scope of their effects on the female body is critical to developing preventive care to promote a longer health span for women.
Sociocultural norms and stigma around weight
Societal pressures and gender norms around body image influence health behaviors, food choices, and body satisfaction. For example, females tend to overestimate their muscular size and express heightened concern regarding gluteal shape, while males exhibit a more realistic self-perception, primarily focused on hip width. 52 Furthermore, in many cultures around the world, larger body size has historically been associated with wealth and health, and slimness is an indicator of poverty and weakness. One study of a North African Arab population reported that 65% of men and 57% of women preferred overweight body size in the opposite gender. 53 This is a stark contrast from the Western world idealization of slimness, which has created a stigma around being overweight that adversely affects self-perception, as well as social interactions, employment, and medical care. Varied views on diet, exercise, and body composition within different cultures and populations affect health behaviors and metabolism outcomes among subpopulations of women. Studies to understand these differences must provide the evidence base to reframe how overweight is communicated in a clinical setting and used as a measure of good versus bad health.
Metabolic disease diagnosis and treatment
The prevalence of metabolic syndrome in women increased from 25.0% (1988–1994) to 34.9% (2007–2012) in the United States and is continuing to rise. 54 The largest increases were observed among non-Hispanic White (44%) and Black (41%) women, with only a 2% increase for Mexican American women. The two risk factors with the most significant increase across the study period for women were elevated waist circumference and low high-density lipoprotein cholesterol. To reduce the risk of CVD, clinical management focuses on these and other modifiable factors, such as hypertension and glucose intolerance. Unfortunately, there is a lack of consensus on which factors are most clinically relevant and necessary to diagnose metabolic syndrome.
Women report adverse drug reactions up to two times more often than men, with sex differences in drug metabolism being a key contributor to higher drug toxicity in women. 55 Enzymatic activity can be altered by sex-dependent hormonal factors, such as pregnancy or oral contraceptive use. Such factors influence the dosage and efficacy of therapeutics. When treating type 2 diabetes, for example, males respond better to sulfonylurea than females, who respond better to rosiglitazone. 56 Inclusion of women—including from diverse subpopulations—in clinical studies and stratification of pharmacokinetic data to elucidate sex differences in treatment guidelines are imperative for reducing the burden of adverse drug reactions due to metabolic differences in women and men.
Conclusion
SWHR is committed to raising awareness about the disproportionate impact of a variety of diseases, conditions, and life stages on women’s health, and this research agenda specifically highlights uterine, autoimmune, and cardiometabolic diseases. With our partners across research, health care, and policy, we will work to drive the research and health care communities to improve women’s health outcomes across the lifespan. SWHR will continue to develop resources that address the research gaps, empower women to better navigate their health care, educate society about the unique health needs of women, and promote science-based and patient-centered health care policies and legislation. Starting with uterine fibroids, lupus, and metabolism as focal points for conditions that exclusively, disproportionately, and differently affect women, we call on stakeholders throughout the health care ecosystem to join us and engage in tackling the challenges elevated in this agenda. The study of sex differences and women’s health does not just benefit women; it truly benefits everyone, as we learn more about what makes each person uniquely different and develop inclusive strategies to improve the health of all people.
Footnotes
Authors’ Contributions
I.O.A.: Conceptualization, investigation, writing—original draft, review, and editing, and supervision. S.C.: Conceptualization, investigation, and writing—review and editing. S.G.: Conceptualization and investigation. All authors read and approved the final article.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
No funding was received for this article.