
Abstract
Objective:
To investigate the perceptions of lactation experiences of neurology faculty and the impact of lactation time on academic achievement.
Materials and Methods:
This was a cross-sectional study utilizing a survey administered across 19 academic neurology centers in the United States. Respondents self-identified as having children and answered questions about lactation at work. Demographic information; academic achievement including publications, guest speakerships, awards, leadership roles, and funding; and perception of lactation experience were analyzed.
Results:
Among 162 respondents, 83% took lactation time at work. Thirty-seven percent reported lack of employer support for lactation, 46% were dissatisfied with their lactation experience, 59% did not receive compensation for lactation time, 62% did not have blocked clinical time, 73% reported relative value units were not adjusted to accommodate lactation, and 43% reported lack of access to private lactation space. Women spent on average 9.5 months lactating per child and desired 2.4 further months of lactation. There was no difference in all measures of self-reported academic achievement between women who did and did not take lactation time when measured across all career stages.
Conclusions:
Although a majority of respondents took lactation time at work, perceptions of employer support for lactation were low, and expectations for work productivity were not adjusted to accommodate lactation time. Taking lactation time at work did not decrease self-reported academic achievement. System-level best practices designed to support lactating faculty should be developed to guide academic institutions.
Introduction
Approximately 44% of full-time academic and clinical faculty at U.S. medical schools are women, and since 2021, women comprise more than 50% of graduating medical students. 1 Women physicians and academic faculty enter the workforce during peak childbearing years. Balancing career development with family planning, caregiving, and domestic responsibilities is difficult and a barrier to early satisfaction with work-life integration. 2 –4 Only 14.9% of U.S. medical schools provide faculty birth mothers with 12 or more weeks of fully paid parental leave. 5 When returning from parental leave, lack of time for milk expression and dedicated lactation space are among the most frequently cited negative experiences of physician mothers, including those in academia. 3
Physician mothers perceive widespread discrimination from their employers and colleagues regarding utilization of family leave and lactation time, causing many to prematurely stop lactating. 4,6 –8 The American Academy of Pediatrics and the World Health Organization recommend exclusively feeding human milk through 6 months of life and continued human milk as long as mutually desired by the parent–child dyad. 9,10 Yet, only 28% of U.S. physicians lactated to their personal goal, with 49% reporting they would have lactated longer with better job accommodations. 6 While available data on lactation experiences at academic medical centers are largely limited to clinical faculty, lactation has been identified as a barrier to equity for women in academia in general, and work-life balance and family leave policies are associated with a woman’s intention to remain in academic medicine. 11,12 In one study of employees of a large academic medical center that surveyed clinicians as well as other employees and staff including those in research, 57% found milk expression at work difficult and 38% reported that their job limited them from lactating as long as desired. 13
Lactation rates are also impacted by race and ethnicity, and it is conceivable that perceptions of experiences may differ by race and ethnicity. The overall prevalence of breastfeeding initiation among U.S. women is 84%. 14 Among women identifying as White only, nearly 86% initiated breastfeeding, compared with 75% of those identifying as Black, 78% of those identifying as American Indian or Alaskan Native, and 90% of those identifying as Asian. 14 To our knowledge, there are no studies that assess differences in lactation experiences among academic medical faculty of various racial and ethnic backgrounds.
With a projected physician shortage of 37,000–134,000 by 2034, every effort to retain women faculty is imperative. 15 This is particularly acute in neurology, where the predicted shortage of neurologists is expected to increase from 11% in 2012 to 19% in 2025. 16 Across all career stages, women faculty physicians have a higher rate of attrition from academia than men. 17 Attempts by academic medical centers to address barriers to lactation, such as providing dedicated lactation spaces and compensation for lactation time, do improve perception of the workplace. 18 However, lactation experiences and solutions to challenges may differ among medical specialties given inherent differences in practice. 4,6,18 To better understand possible barriers to satisfaction with work-life integration among neurology faculty, it is necessary to evaluate the culture and perception of lactation support for women in academic neurology. To our knowledge, there is no previous study of lactation experiences specifically among neurology faculty. In addition, while taking lactation time may be perceived to decrease productivity, there are no published data investigating the academic achievements of faculty who take lactation time.
This study investigated the perceptions of lactation experience and the impacts of taking lactation time at work on academic achievements among academic neurology faculty. We hypothesized that individuals who took lactation time would have lower academic achievement compared with women with children who did not take lactation time and that Black, Indigenous, and people of color (BIPOC) women would have worse perceptions of lactation experiences than White women.
Materials and Methods
Study design
This was a cross-sectional study and subanalysis of a larger standardized survey administered across 19 academic neurology centers in the United States as part of the “Women in Neurology Collaborative Study (WINCS).” The WINCS sought to evaluate the impact of gender and race on career advancement for academic neurology faculty. 19 Our current study focuses on lactation experience. Details on survey development and administration are available in a previously published article. 19 Briefly, the centers were recruited from the American Academy of Neurology Women in Neurology section, as well as from personal outreach (by SP) for voluntary participation to represent geographical and size diversity. The participating sites are listed in Supplementary Data S1. Sites represented all four geographic regions and eight of nine geographic divisions recognized by the U.S. Census Bureau. 20 The principal investigator for each site secured Institutional Review Board (IRB) approval with an exemption or waiver of informed consent, as deemed appropriate by the site IRB.
Data collection
The survey was active from February 19, 2021 to April 6, 2022. The survey collected information on demographics; academic achievements including average number of peer-reviewed publications per year in the last 5 years and the total number of first/last authorships, awards, guest speakerships, leadership roles, and funded projects; compensation; perception of gender equity; domestic circumstances; and parental leave (Supplementary Data S1). The lactation information collected included whether the respondent expressed milk at work, the number of months of milk expression per child, the desired duration of further milk expression, and perceptions of lactation experiences using nine Likert scale questions. There is currently no validated instrument to evaluate lactation experience among faculty in academic medicine. Thus, the Likert questions were created by neurology faculty with direct experience of lactation challenges.
Survey participants
Adult and pediatric neurology faculty with advanced degrees (MD, DO, PhD, MD/PhD, MBBS, and MS) were eligible respondents. Survey respondents included in our lactation analysis self-identified as women with children and answered lactation questions about milk expression at work. All respondents who self-identified as women were asked, “Did you breastfeed/pump at work when you had your child(ren)?” with answer options as follows: “Yes, I breastfed/pumped at work,” “No: I did not breastfeed/pump at work,” and “Does not apply.” Respondents who answered “yes” and “no” were included in the analysis. Those who responded “does not apply” and those who did not identify as women were not included in the analysis.
Statistical analysis
Statistical analysis was performed using R version 4.3.2. Means with standard deviations and counts with percentages are reported as appropriate. The survey item used to indicate racial/ethnic identity included the following response selections: American Indian/Alaskan Native, Asian, Black or African American, Native Hawaiian or other Pacific Islander, White, Hispanic/Latino, unknown, not reported, and prefer not to say. More than one option could be selected to allow for the possibility of combinations in which individuals could be classified as multiracial/ethnic. Respondents were classified as BIPOC if they selected either singularly or chose multiple selections of “Black or African American,” “American Indian/Alaskan Native,” “Native Hawaiian or other Pacific Islander,” “Asian,” and/or “Hispanic/Latino.” Analysis of perception of lactation support by race/ethnicity was restricted to BIPOC women versus White women due to small respondent numbers in categories other than “White” (Table 1). Respondents who declined to report race/ethnicity were not included in the analysis.
Demographic and Sample Characteristics of Survey Respondents
Note: Data are presented as mean (SD) or frequency (percentage) as appropriate.
BIPOC, Black, Indigenous, and people of color.
A Likert scale of nine lactation questions was used to determine perception of lactation support (Table 2). Due to small sample size, we collapsed responses “very strongly agree,” “strongly agree,” and “agree” into one response of “agree,” and similarly, “very strongly disagree,” “strongly disagree,” and “disagree” were collapsed to “disagree.” The modified values therefore are “agree,” “disagree,” and “neutral.” Analysis was done using a Chi-square test for perception of lactation between BIPOC women and White women.
Respondent Answers to Questions on Perceptions of Lactation Experiences by Race
RVU, relative value unit.
Scatter plots were used to show the values of the six measures of academic achievement that are continuous variables (number of first/last authorships, average number per year of peer-reviewed publications in the last 5 years, awards, guest speakerships, leadership roles, and funded projects) by respondents’ years in profession (Fig. 1).
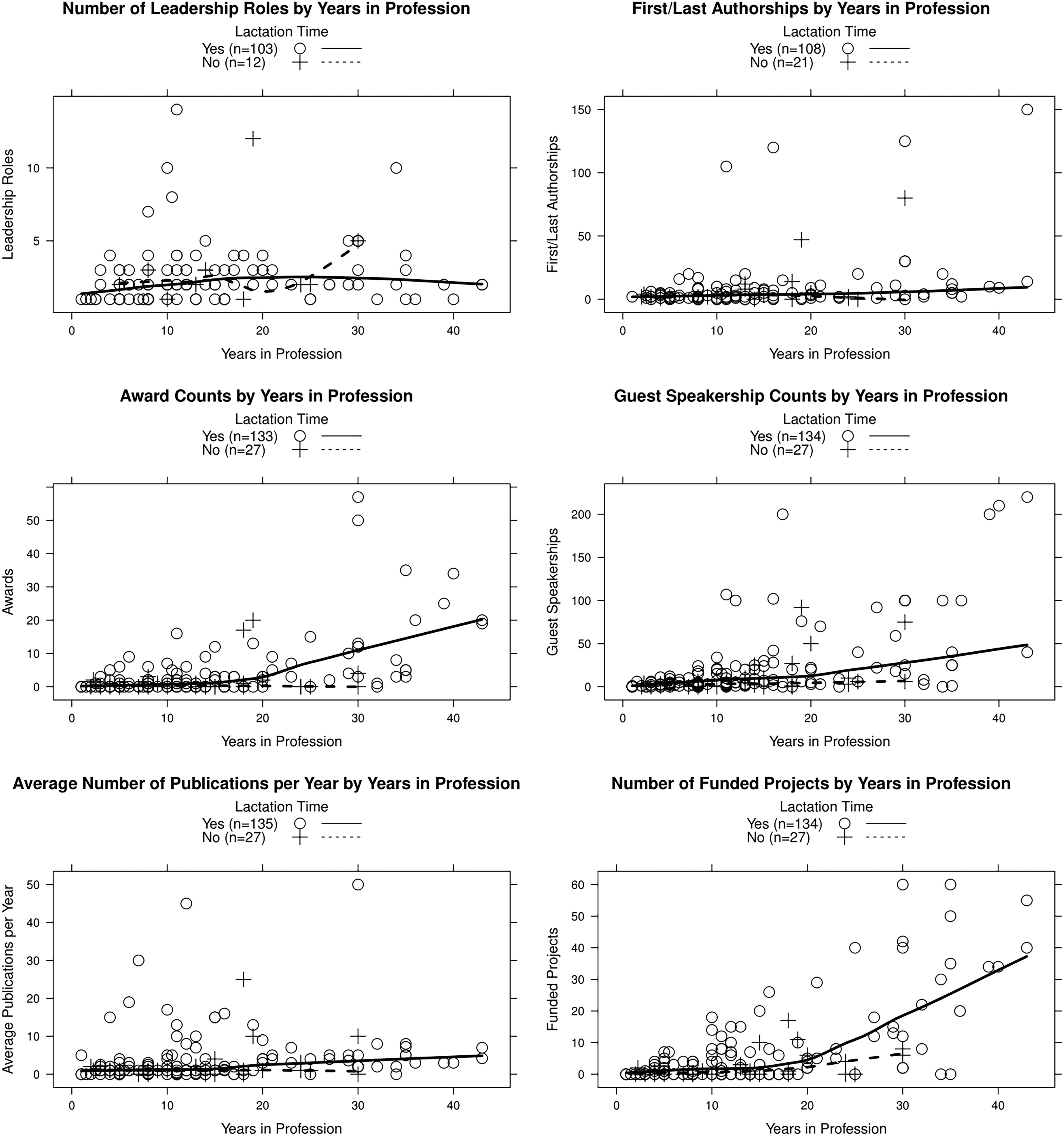
Scatter plots with smooth fitted curves showing surveyed measures by years in profession, grouped by whether or not respondents took lactation time.
Results
Of the 462 respondents who completed the survey, 162 met the inclusion criteria for the current analysis of women with children who answered questions about milk expression at work. Table 1 summarizes the demographic characteristics of this cohort. Overall, 84.5% of respondents had either a medical degree (MD, DO, or MBBS) alone or a combined degree (medical degree plus PhD or MS). Most (88.3%) respondents were in marital or long-term relationships. Respondents had an overall average of 14.2 years of experience within their respective fields, and 48.8% held positions as assistant professors, 27.8% as associate professors, and 17.9% as professors.
Among the 162 respondents, 135 (83.3%) took lactation time at work and 27 (16.7%) did not. Of those taking lactation time, 63.7% identified as White, 33.3% identified as BIPOC, and 3.0% did not respond to the race question. Of those who did not take lactation time, 70.4% identified as White and 29.6% identified as BIPOC.
Perception of lactation experience
Overall, when responding to the statement, “I felt satisfied with the lactation experience as a working mom,” 34.3% agreed, 45.5% disagreed, and 20.1% were neutral. Although 29.8% of respondents reported that they felt supported in their lactation efforts by their employer, 36.5% did not. While 52.9% reported that they felt coworkers supported their lactation efforts, 19.4% did not. Overall, 23.1% of respondents agreed that lactation time was paid, 58.9% disagreed, and 17.9% were neutral. Most (61.9%) did not have blocked clinical time to accommodate lactation efforts, and 73.1% reported that their clinical relative value unit (RVU) expectations were not adjusted for lactation time. The availability of designated private lactation space was mixed, with 47.7% agreeing that they had access to such a space and 42.5% disagreeing. Overall, respondents spent on average 9.5 months lactating per child and desired 2.4 further months of lactation.
Subanalysis comparing the perceptions of lactation experience between White and BIPOC faculty did not show significant differences in the responses to most questions (Table 2). However, BIPOC respondents were less likely to agree that lactation time was compensated than White respondents (11.3% and 30.2%, respectively; p = 0.05). A larger percentage of BIPOC than White individuals disagreed with the statement “I felt supported in my lactation effort by coworkers,” but this was not statistically significant (27.2% versus 13.9%, respectively; p = 0.09). There was no statistically significant difference between White and BIPOC faculty on the months lactating per child (9.08 versus 10.4, p = 0.16) and the number of further desired months (1.79 versus 3.41, p = 0.07).
Academic achievement
Figure 1 depicts six measures of scholarly achievements—average number of peer-reviewed publications per year in the last 5 years and total numbers of first/last authorships, awards, funded projects, leadership positions, and guest speakerships over career duration—displayed by years in profession. When adjusted for years in profession, there was no clear difference in academic achievements between women who took lactation time at work and women who did not. There was a trend toward increased awards, guest speakerships, and funded projects after 20 years in their profession in faculty who took lactation time at work. However, there were only five respondents who did not take lactation time who had been in their profession longer than 20 years, limiting our ability to draw any comparative conclusions for those in the profession longer than 20 years. There was no difference in academic achievement between White and BIPOC respondents who took lactation time. However, all BIPOC respondents had been in their profession <16 years, limiting our ability to make achievement comparisons. Due to survey design, we are unable to evaluate the short-term impact of taking lactation time at work on academic achievement during specific lactation periods for individuals.
In summary, although some respondents found support and accommodations for lactation while at work, the majority reported challenges, particularly in the areas of time, compensation, and access to private spaces. BIPOC faculty were less likely to report that lactation time was compensated compared with White faculty. Across all career stages, there was no difference in academic achievement between those who took lactation time at work and those who did not.
Discussion
This study of women academic neurology faculty and their lactation experiences at work demonstrated low employer support for lactation, frequent lack of private lactation spaces, limited adjustment of clinical productivity goals or salary to accommodate lactation efforts, and low levels of satisfaction with lactation experiences. Similar perceptions and challenges have been observed in previous studies, leading to premature discontinuation of lactation, insufficient milk supply, and health consequences, such as mastitis. 4,6 –8
Although other studies evaluate the perception of lactation experiences of broader physician groups or other medical and surgical specialties, to our knowledge, this is the first study to assess lactation experiences specifically among academic neurology faculty. While many challenges are common across specialties, neurology faculty face unique factors impacting lactation experiences, especially in clinical settings. For instance, neurological evaluations are often longer than in other specialties, which reduces opportunities for milk expression. The shortage of neurologists and access concerns may result in increased pressure to see more patients, resulting in less time for milk expression. In the inpatient setting, neurologists must respond to unpredictable acute care situations, such as status epilepticus or acute stroke, that require immediate evaluation and treatment and limit the ability to schedule lactation time. Finally, the gender gap in neurology academic leadership may further affect efforts to increase lactation support since senior men who most frequently design policies are often not cognizant of the barriers faced by junior women physicians. 21 While women comprise about 21.9% of U.S. clinical science department chairs in all specialties, only 17.4% of neurology department chairs are women. 22 Institutions looking to improve lactation experiences must consider the practice conditions of all lactating faculty to ensure that solutions are available to a variety of concerns.
To our knowledge, this is the first study to assess the effects of taking lactation time at work on academic achievement. Taking lactation time at work does not appear to negatively impact self-reported academic productivity. With this recognition, academic neurology leadership has an opportunity to provide more support to lactating faculty. While our survey did not investigate the impacts of specific policies, other studies have recommended a variety of options to support lactating faculty. Paid parental leave is associated with an increase in lactation initiation and duration, as well as improved physical and mental health for the child and lactating person. 23 In one study of women in academic medicine, work-life integration and fair and transparent family leave policies were associated with a woman’s intent to remain at her institution. 12 However, only 14.9% of U.S. medical schools provide faculty birth mothers with 12 or more weeks of fully paid parental leave. 5 Lactation limits conference and travel ability, thus impacting collaboration, networking, and other opportunities that may increase productivity. 11 To accommodate, employers could reimburse childcare costs during work-related travel and reimburse for shipping expressed milk. 11 The lack of adequate lactation space has been reported in previous studies. 4,6 –8 In our study, 42.5% of respondents reported that they lacked adequate lactation space. Lactation rooms close to clinical and academic worksites equipped with not only a hospital-grade pump, chair, table, sink, refrigerator, and electrical outlet, but also computers and phones allow lactating faculty to continue working during milk expression if able and by choice. To be effective, lactation spaces must also be plentiful enough to be unoccupied when needed. In one study of women working at an academic medical center, 5.6 minutes was the reported average maximal acceptable time to walk to a lactation room, and 83% preferred lactation suites that accommodate multiple simultaneous occupants. 13 Further study is needed to determine if specific lactation policies enhance lactation experiences and faculty retention. Additionally, to inform policies that best support lactating faculty, future research should directly examine the short-term impacts of lactation on academic achievement.
While we did not evaluate the impact of lactation on clinical productivity, taking time for lactation inherently limits short-term clinical productivity. Employers can further support lactation by instituting policies that mitigate a lactating person’s concern over lost clinical productivity. Such policies include work RVU (wRVU) credit for lactation time, lower patient caps for teams with lactating physicians, reimbursement for wearable pumps, telework options, clinical coverage for pumping breaks outside of regularly scheduled breaks, paid parental leave, and onsite childcare. 4,7,11,18,24 While academic and clinical leaders may view compensated lactation time as cost prohibitive, in one study, the average cost to reimburse clinical time blocked for lactation for a mean of 8.9 months was $9125.78. 18 This constitutes a small percentage of clinical faculty reimbursement. While data on the effects of lactation policies are lacking, limited data have shown that lactation policies including wRVU credit for lactation time and providing adequate lactation spaces can improve faculty perceptions of institutional culture support for lactation. 18 Part-time employment options may also improve lactation initiation and duration, though they may not be desired by lactating individuals. 25
The successful implementation of lactation policies requires the creation and dissemination of formal policies that are enthusiastically supported by leadership and address the variety of work conditions faced by employees. 26 Importantly, official lactation policies relieve the burden of advocating for lactation accommodations from the lactating person, which may affect relationships with colleagues and superiors. 26 It is important to intentionally evaluate and amend any policy attempting to neutralize the impacts of gender, including lactation, as these policies can have unintended consequences. 11 For instance, one study of U.S. academic economists found that gender-neutral tenure extension policies decreased tenure rates for women and increased tenure rates for men. 27 Since 2010, federal legislation has required certain employers to provide time and space for milk expression for 1 year after birth for hourly workers, though it excluded salaried employees and likely most academic medicine faculty. 28 The Providing Urgent Maternal Protections for Nursing Mothers Act effective starting April 28, 2023 expanded protections to require most employers to provide milk expression time and space for 1 year after birth to all employees, excluding only certain transportation employees and employers with fewer than 50 employees. 28 The impacts of this law on lactation among both medical faculty and the U.S. population at large remain to be seen. Importantly, these policies protect lactation time only for 1 year after birth, though both the American Academy of Pediatrics and the World Health Organization recognize the benefits of providing human milk for 2 years after birth and beyond. 9,10
Our efforts to assess how experiences may differ among White versus BIPOC women are also unique. Although rates of breastfeeding initiation are significantly lower among women identifying as Black and American Indian or Alaskan Native as compared with women identifying as White, to our knowledge, there are no studies evaluating how lactation experiences differ among White versus BIPOC academic medical faculty. It is conceivable that these racial differences persist among academic faculty and that perceptions of lactation experiences may differ among those with differing racial identities. Due to the small numbers of BIPOC respondents in our study, subanalysis evaluating lactation experiences by race was limited. However, BIPOC women were less likely to agree that lactation time was compensated than White women (11.3% and 30.2%, respectively; p = 0.05). This suggests that lactation experiences may differ among races, and further investigation of faculty lactation experiences should analyze racial and ethnic differences.
Our findings and their impacts should be interpreted considering the following limitations. The survey did not inquire about the timing or frequency of respondents’ lactation, and academic achievement was assessed only once, covering their entire career. Therefore, we cannot determine if there were differences in academic achievements during specific lactation periods for individuals. Nevertheless, across all career stages, there was no disparity in academic achievement between those who took lactation time and those who did not. Since we did not assess the recency of respondents’ lactation experiences, their perceptions may not reflect current policies at their institution. While achievements were not significantly affected by taking lactation time, we did not assess for exhaustion or burnout associated with maintaining productivity while lactating, which may impact faculty satisfaction and retention. Our study also cannot assess those who left their academic position due to childbirth or lactation. We surveyed respondents at 19 institutions, representing a small percentage of academic neurology departments. However, these institutions did reflect regional diversity and offer a broader view than studies that focus on single-center experiences. As a survey, our study is subject to both selection and recall bias. Respondents who were more interested in the topic may have been more likely to participate, and long-term recall can lead to inaccurate responses. Respondents self-reported their academic achievements, which may further introduce bias. Additionally, we did not obtain detailed measures of academic achievements such as the scope of leadership positions, journal impact factors, or award prestige. We also did not measure lactation impacts on clinical productivity and reimbursement, which may be more concerning to clinical faculty and institutions than academic achievement. Our survey only assessed experiences of faculty, excluding the experiences of trainees and students who may have an even harder time procuring protected lactation time, space, and resources. Most respondents held medical degrees. However, research and clinical faculty may face different lactation barriers and have varying departmental expectations, compensation, and promotion criteria. Furthermore, our results may not accurately reflect experiences among nonacademic neurologists or of lactation across the gender spectrum, including nonbinary individuals. Finally, due to limited respondent numbers, those identifying as an underrepresented race and/or ethnicity were grouped together as “BIPOC” for statistical analysis. However, combining multiple races and ethnicities into a single group prevents a full understanding of the impacts race and ethnicity may have on lactation experiences.
Conclusions
In this retrospective survey of academic neurology faculty and their lactation experiences at work, respondents expressed low perceptions of employer support for lactation, frequent lack of private lactation spaces, limited adjustment of clinical productivity goals or salary to accommodate lactation efforts, and low levels of satisfaction with lactation experiences. Lactation time at work did not affect self-reported academic achievement across all career stages, though the short-term impacts of lactation on academic achievement warrant further investigation. There are concrete steps that institutions can take to improve lactation experiences, and further research is needed to establish best practices to support lactating neurology faculty. Future studies should assess the impact lactation policies have on faculty recruitment, retention, and burnout. Our study suggests that lactation experiences may differ between White and BIPOC individuals, though the sample size was small and the findings were not consistently significant. The intersectionality of race and ethnicity on lactation experiences should be included in future research in this area.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Virginia J. Howard, Professor of Epidemiology in the School of Public Health at the University of Alabama at Birmingham, for her contributions to initial survey design. We also acknowledge Dr. Laurie Gutmann, Department of Neurology, Indiana University and Dr. Sneha Mantri, Department of Neurology, Duke University for their contributions in investigation.
Authors’ Contributions
S.D.: Investigation, formal analysis, resources, writing (original draft and reviewing and editing), project administration, and visualization; J.M.: Formal analysis, writing (original draft and reviewing and editing), and visualization; C.Z.: Writing (original draft and reviewing and editing), data curation, and visualization; P.G.: Conceptualization, methodology, investigation, and writing (reviewing and editing); C.Z.: Investigation and writing (reviewing and editing); H.A.: Investigation, resources, and writing (reviewing and editing); S.S.: Investigation, formal analysis, and writing (original draft and reviewing and editing); S.D.: Writing (original draft and reviewing and editing); A.H.: Writing (reviewing and editing), data curation, and visualization; A.Y.: Writing (reviewing and editing) and data curation; C.N.: Conceptualization, methodology, investigation, validation, writing (reviewing and editing), supervision, resources, and project administration; P.S.: Investigation and writing (reviewing and editing); K.R.: Investigation and writing (reviewing and editing); M.A.: Investigation and writing (reviewing and editing); D.K.: Investigation and writing (reviewing and editing); N.A.: Investigation and writing (reviewing and editing); N.F.: Investigation and writing (reviewing and editing); S.N.: Investigation and writing (reviewing and editing); K.Z.: Investigation and writing (review and editing); S.D.J.: Writing (reviewing and editing); N.B.: Investigation and writing (reviewing and editing); N.F.-S.: Investigation and writing (reviewing and editing); L.T.: Investigation and writing (reviewing and editing); J.Y.-C.: Investigation and writing (reviewing and editing); D.B.: Investigation, formal analysis, writing (original draft and reviewing and editing), and resources; J.A.: Investigation and writing (reviewing and editing); A.W.: Conceptualization, methodology, and writing (reviewing and editing); J.S.: Conceptualization, methodology, and writing (reviewing and editing); S.A.-L.: Conceptualization, methodology, investigation, resources, and writing (original draft and reviewing and editing); S.P.: Conceptualization, methodology, investigation, validation, data curation, formal analysis, writing (original draft and reviewing and editing), supervision, resources, and project administration.
Author Disclosure Statement
S.I.P. has received honoraria for lectureship from Hofstra University, served as expert witness and legal consultant, is on the Epilepsy Foundation of Minnesota Board of Directors, is funded by drug trials for Xenon and UCB Pharma, chairs the American Epilepsy Society Digital Advisory Committee, and serves on the University of Minnesota Center for Women and Medicine group and the American Neurological Association Ideas Task Force. P.G. received support from the Palatucci Advocacy Leadership Forum Grant by the American Academy of Neurology. N.A. received honoraria for Facilitating Anti-racism discussions at Brown University. D.H.K. has received royalties from Springer, honoraria from the PRI-MED conference, and meeting/travel support from the American Academy of Neurology for the Undergraduate Education Subcommittee. S.S. has received support from Biogen and Verasci. H.B.A. receives compensation from the American Academy of Neurology for her position as Deputy Editor of the Neurology Minute podcast and is funded by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH; Grant #KL2TR001421) and has received lecture honoraria from the American Epilepsy Society. N.F. has received grant funding from the Patient-Centered Outcomes Research Institute and NIH. K.Z. has received grant funding from Eisai (investigator-initiated study grant) and has participated on the SK Life Sciences Advisory Board. N.B. has received funding from SUNY Upstate Patient Advocacy Fund for a study not related to this article. L.T. received author royalties from UpToDate, payment/consulting fees for medical-legal consultation, and honoraria and support for conference fees for neurology/toxicology lectures and participates on a Data Safety and Monitoring Board at Indiana University for studies involving ethanol infusion. J.K.S. has received support from the Binational Scientific Foundation Grant for Culinary Medicine, textbook royalties from Textbook Essentials of PM&R and Easy EMG, is an advisor for Simplified a company dedicated to lactation consulting, and is a Third Culture Capital venture partner. J.B.A. is funded by grants from the U.S. Department of Defense (W81XWH-17–1-0619), the Evelyn F. McKnight Brain Institute (PI), LivaNova Inc, and NIH (R01HD102723 [PI]) for studies unrelated to the current study, has received lecture honoraria from the Cleveland Clinic, travel funds from the International League Against Epilepsy, has received consultant fees from LivaNova Inc, participates on a Data Safety and Monitoring Board at the University of Alabama at Birmingham/University of Colorado Anschutz Medical Campus, serves on the American Epilepsy Society Scientific Program Committee, and serves as an associate editor for Epilepsy and Behavior Reports. All other authors report no interests to declare.
Funding Information
This project was not funded.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.