
Abstract
Objective:
To estimate the prevalence of diagnosed vasomotor symptoms (VMS) due to menopause among US women aged 40–64 years and assess sociodemographic differences in VMS prevalence and risk of discontinuing VMS-related treatment.
Materials and Methods:
This retrospective study evaluated merged data from IQVIA’s PharMetrics Plus medical claims and consumer attributes databases for 2017–2020. VMS diagnosis was identified using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis codes. Continuous enrollment was required ≥6 months before and 12 months after diagnosis date. Treatment discontinuation was measured for VMS-related treatments initiated at diagnosis or during the 12 months after diagnosis. Treatment duration was measured from diagnosis to the first day of a ≥90-day treatment gap. A Cox proportional hazards model was used to determine factors associated with risk of treatment discontinuation.
Results:
Among 7,386,206 eligible women, the 4-year prevalence of diagnosed VMS in 2017–2020 was 79.1 per 1,000 and was highest among non-Hispanic White women (82.5 per 1,000), followed by Hispanic (77.3), Black (71.6), and Asian women (64.5). Rates were higher among women living in urban areas and those with higher education and income. Among women newly diagnosed with VMS (n = 226,262), median treatment duration was 297 days. Black, Asian, and Hispanic women had higher risks of discontinuing treatment than non-Hispanic White women. Lower income was also associated with higher risk of discontinuation than higher income.
Conclusion:
Lower prevalence of diagnosed VMS and higher risk of treatment discontinuation were observed among racial/ethnic minorities and women with less education and income, suggesting possible underdiagnosis and unmet needs.

Introduction
Vasomotor symptoms ([VMS]; i.e., hot flashes and night sweats) are generally considered the hallmark symptoms of menopause. 1 It is estimated that up to 80% of women experience VMS at some point during the menopausal transition, with symptoms peaking in the late perimenopausal and early postmenopausal years. 2 However, the prevalence of VMS due to menopause has been shown to vary widely depending on factors such as method of symptom ascertainment, geographic region, and sample size, as reported in a 2010 systematic review. 3 Many women report experiencing moderate to severe VMS, with significant adverse effects on quality of life. 4,5 Symptoms are often associated with sleep disturbances, fatigue, and impaired concentration that can negatively impact ability to work and carry out daily activities. 1,4,6,7 Further, frequent VMS have been found to persist for a median of 7.4 years, with the longest duration among African American women and the shortest among Chinese women. 8
While VMS affect most women of menopausal age, research has elucidated some differences in symptom reporting across various sociodemographic characteristics. The Study of Women’s Health Across the Nation (SWAN) has followed approximately 3,000 midlife women in the United States since the mid-1990s and found that African American women report higher rates of VMS. 2,9 Other factors found to be associated with higher rates of reported VMS include less than a college education, current smoking, higher body mass index, and symptoms of depression and anxiety. 1,2,10 The underlying mechanisms of these associations are not well understood, and other potential socioeconomic determinants of VMS remain unexplored.
Hormone therapy is considered the cornerstone of VMS management and has been shown to be effective in reducing the severity and frequency of symptoms. 11,12 For women who cannot use hormone therapy or choose not to, multiple nonhormonal options are available, such as fezolinetant, low-dose paroxetine, gabapentin, and various selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs). 12 Some previous research has identified sociodemographic differences in the receipt of treatment for VMS. The US-based Menopause Epidemiology Study found that 61% of White women reported seeking health care for menopausal symptoms compared with just 53% of Black women. 13 Similarly, 52% of White women reported using hormone therapy to treat menopausal symptoms compared with 35% of Black women and 45% of Hispanic women. 13 Despite these large differences in the use of hormone therapy, little is known about the patterns and correlations to hormone therapy and nonhormonal VMS-related treatment use among women during menopause.
To our knowledge, no analysis of health care claims data has examined the prevalence and sociodemographic correlates of diagnosed VMS among women of menopausal age. A better understanding of the diagnostic and treatment disparities in such a dataset may have important implications in the provision of equitable care, especially considering that many women report not seeking treatment for menopause-related concerns. 6 Further, among women who do seek and receive treatment for VMS, it is unclear whether disparities exist in treatment persistence. Using a large commercial claims database, this study sought to quantify sociodemographic differences in the prevalence of diagnosed VMS and in the risk of discontinuing VMS-related treatment.
Materials and Methods
Study design and setting
These retrospective, noninterventional, and database analyses included data from commercially insured women in the United States.
Data sources
We used linked data from IQVIA PharMetrics Plus and consumer attributes (Cx) databases. PharMetrics Plus comprises adjudicated claims for more than 150 million commercially insured individuals across the US and includes all medical and pharmacy claims data. The data represent a variety of employer, payer, and provider types from diverse geographic regions, with patients in every 3-digit zip code and every Metropolitan Statistical Area of the United States.
Participants identified in the PharMetrics Plus database were linked to the Cx database, which is multisourced and based on compiled self-reported information. The Cx database includes key individual sociodemographic information, such as race, ethnicity, education level, income, and urbanicity. To construct the linked dataset, we created an encryption algorithm using patient-level information to deidentify patients. The deidentified patient IDs then underwent a deterministic process to match patients across databases.
Identification of sample
To assess the prevalence of diagnosed VMS, we used January 1 to December 31 as the sample selection period for each year during an overall study period spanning July 1, 2016, through December 31, 2021 (Fig. 1). Women aged 40–64 years were included if they had linked PharMetrics Plus and Cx data available between January 1 and December 31 of that calendar year. Those with coverage by Medicare Risk, Medicare Cost, or State Children’s Health Insurance program were excluded, as they may have supplemental coverage from these sources outside of their commercial networks. Hence, the PharMetrics Plus database would not capture all of their medical claims.

Study design for assessing prevalence of diagnosed VMS. VMS, vasomotor symptoms.
We selected a separate study period to measure VMS-related treatment use (Fig. 2). Women newly diagnosed with VMS aged 40–64 years with linked PharMetrics Plus/Cx data were identified during the selection period spanning April 1, 2016, to December 31, 2020. The index date was the earliest date of first VMS diagnosis. Any woman with a diagnosis of VMS during a look back period from the index date to database start date (January 1, 2013) was excluded. Baseline demographics and clinical characteristics were assessed during a 6-month preindex period, and outcomes were assessed during a 12-month postindex period. Women were also required to have continuous health plan enrollment for at least 6 months before and 12 months after the index date. Those with invalid or missing health plan enrollment dates were excluded.

Study design for measuring VMS-related treatment utilization among women newly diagnosed with VMS. VMS, vasomotor symptoms.
Women with a diagnosis of VMS were identified via International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis codes. Because no ICD-10-CM codes are specific to VMS, several codes were used to discern a diagnosis. The detailed definition of a VMS diagnosis claim included any medical claim with ICD-10-CM codes that satisfied either of the following conditions: (1) Natural or surgical menopausal/female climacteric states (ICD-10-CM, N95.1) OR (2) Flushing (ICD-10-CM, R23.2) or hyperhidrosis (ICD-10-CM, R61) and ≥1 claim with an ICD-10-CM code associated with natural menopause or a procedure/diagnosis code for surgical menopause (ICD-10-CM, E28.310, E28.319, E28.39, E89.40, E89.41, or Z78.0) on the same date or in the prior 12 months.
Statistical analysis
Prevalence assessment
We computed prevalence of diagnosed VMS for each of the calendar years 2017, 2018, 2019, and 2020 and the 4-year period prevalence of combined years 2017–2020. Prevalence estimates were calculated by dividing the total number of women with a VMS diagnosis by the total number of women with study eligibility during the calendar year of interest. To adjust estimates to reflect a national commercially insured US population, a base projection methodology was used. Sample weights were applied to a subset of persons in the database to correct for underrepresentation or overrepresentation of any age group, based on distributions reported in national census data. This projection method has been used previously with data in IQVIA’s PharMetrics Plus and open-source claims databases. 14 –16 Subsequently, a multivariable logistic regression model was used to determine factors associated with the odds of a VMS diagnosis for the latest nonCOVID year (i.e., 2019). Collinearity among sociodemographic covariates was evaluated prior to model development, and covariates without multicollinearity (including age group, region of residence, health plan type, race/ethnicity, income level, and area of residence) were included in the final model. A stepwise approach for variable selection was also used, with a p-value of <0.10 required for retention in the model. Patients with missing values for any covariate were excluded from the model, and a p-value of <0.05 was considered statistically significant.
VMS-Related treatment discontinuation
Postindex VMS-related treatment use and discontinuation were assessed among women with a VMS diagnosis. VMS-related medications were characterized as hormone therapies (estrogen alone, estrogen + progesterone, selective estrogen receptor modulators [SERMs], and conjugated estrogens) and nonhormonal therapies (SSRIs, SNRIs, paroxetine, gabapentin, and clonidine). Subsequently, VMS-related treatment discontinuation was measured from the date of first VMS diagnosis (index date) to a gap of at least 90 days for which neither a VMS diagnosis nor VMS-related medication was present in any claim. The first day of the gap was considered the end of the treatment duration. VMS-related treatment discontinuation was computed only for treatments that were newly initiated during the postindex period (i.e., after VMS diagnosis).
To determine factors associated with the risk of discontinuation of VMS-related treatment among women newly diagnosed with VMS, a Cox proportional hazards model was used and proportional hazards assumptions were assessed for each covariate. Age group, region of residence, race/ethnicity, income level, index year, and the presence of baseline VMS-related comorbidities were included in the model. VMS-related comorbidities (including sleep disturbances, anxiety, and depression) were defined based on the presence of relevant diagnostic or procedure codes during the 12-month postindex period. Codes used to define the VMS-related comorbidities are shown in Supplementary Table S1. Interactions between covariates were not assessed.
Collinearity among covariates was evaluated prior to model development, and covariates without multicollinearity were included in the final model. Education category was ultimately removed from the model due to moderate multicollinearity with income (r = 0.39). A stepwise approach for variable selection was also used, with a p-value of <0.10 required for retention in the model. Patients with missing values for any covariate were excluded from the model. A p-value of <0.05 was considered statistically significant.
Results
Sample selection and characteristics
The final sample for the prevalence estimation included 4,995,994 women with linked PharMetrics Plus/Cx data in 2017, 4,857,778 women in 2018, 4,785,670 in 2019, and 4,678,688 women in 2020 (Table 1 and Supplementary Fig. S1). In total, 7,386,206 unique women (mean [SD] age: 54.6 [5.6] years) were included in estimating VMS prevalence rates between the years 2017–2020.
Projected 4-Year Period Prevalence Rates of VMS per 1,000 Women, by Age Group and Year
Projected 4-year period prevalence (2017–2020) per 1,000 women with VMS (unique patients were counted only once in overall number of eligible women).
VMS, vasomotor symptoms.
The final sample of women newly diagnosed with VMS included 226,262 women (Supplementary Fig. S2). Most (83.0%) were in the age group 45–60 years. Nearly three quarters (71.7%) were non-Hispanic White, about half (49.2%) resided in the southern region of the US, and the majority (74.5%) had a preferred provider organization (PPO) health plan (Table 2). After the VMS diagnosis date (index date), 16.8% used hormone therapy, 13.9% used nonhormonal therapy, and 71.8% used neither. Additional clinical characteristics are shown in Supplementary Table S2.
Demographic Characteristics of Women Newly Diagnosed With VMS, 2017–2020
VMS, vasomotor symptoms.
Prevalence estimates
The estimated 4-year period prevalence of diagnosed VMS for combined years 2017–2020 was 79.1 per 1,000 women, with the annual prevalence highest in 2019 (41.1 per 1,000) and lowest in 2020 (37.9 per 1,000). The 4-year period prevalence rates were highest among women aged 51–54 years (133.2 per 1,000) and lowest among women aged 40–44 years (21.5 per 1,000) (Table 1).
Disparities in VMS prevalence emerged across various sociodemographic characteristics (Table 2). Four-year period prevalence rates were highest among women living in the South (97.5 per 1,000) and West (96.2 per 1,000) of the United States and lowest in the Midwest (62.5 per 1,000) and Northeast (55.8 per 1,000). Additionally, women living in urban areas had higher 4-year period prevalence rates of VMS (80.6 per 1,000) than those living in rural areas (69.9 per 1,000). Non-Hispanic White women had the highest 4-year period prevalence rates of diagnosed VMS (82.5 per 1,000), followed by Hispanic women (77.3 per 1,000), women of other race/ethnicity (77.1 per 1,000), non-Hispanic Black women (71.6 per 1,000), and non-Hispanic Asian women (64.5 per 1,000). Four-year period prevalence rates of diagnosed VMS were also generally higher among women with higher levels of education and income. Women who had completed graduate school had the highest prevalence rates (92.9 per 1,000), while those who had not completed high school had the lowest (73.2 per 1,000). Similarly, women reporting at least $250,000 in annual income had the highest 4-year period prevalence rates (105.3 per 1,000), while those reporting $20,000–$34,999 in annual income had the lowest (63.5 per 100,000). Additionally, 4-year period prevalence rates were higher among women with PPO (84.3 per 1,000) and consumer-directed health plan (CDHP) insurance (75.2 per 1,000) and lowest among those with health maintenance organization (HMO; 64.0 per 1,000) and indemnity insurance (55.8 per 1,000).
Odds of a VMS diagnosis
Women aged at least 45 years had higher odds of receiving a VMS diagnosis than those aged 40–44 years, with those aged 51–54 years having more than five times the odds of diagnosed VMS (adjusted odds ratio [OR] [95% confidence interval (CI)]: 5.31 [5.19–5.43]; p < 0.001). The odds of receiving a VMS diagnosis were 31% lower for non-Hispanic Asian women (adjusted OR [95% CI]: 0.69 [0.67–0.71]; p < 0.001), 18% lower for non-Hispanic Black women (0.82 [0.81–0.84]; p < 0.001), and 13% lower for Hispanic women (0.87 [0.85–0.89]; p < 0.001) than for non-Hispanic White women. Further, compared with women with annual incomes less than $35,000, those with incomes of at least $35,000 had elevated odds of a VMS diagnosis, with ORs increasing with each higher income category. The odds of receiving a VMS diagnosis were also 18% lower for women with indemnity insurance (adjusted OR [95% CI]: 0.82 [0.76–0.88]; p < 0.001) and 25% lower for those with HMO insurance (OR [95% CI]: 0.75 [0.74–0.76]; p < 0.001) compared with those with PPO insurance. Finally, women residing in urban areas had slightly higher odds of being diagnosed with VMS compared with those in rural areas (adjusted OR [95% CI]: 1.18 [1.13–1.23]; p < 0.001) (Fig. 3).

Odds ratios of diagnosed VMS by sociodemographic characteristics in 2019. aIncome level refers to annual household income. CDHP, consumer-directed health plan; CI, confidence interval; HMO, health maintenance organization; POS, point-of-service; PPO, preferred provider organization; ref, reference level; VMS, vasomotor symptoms.
Treatment use and discontinuation
Across the entire sample of women newly diagnosed with VMS, the median duration of VMS-related treatment use (measured to the first day in a ≥90-day treatment gap) in the postindex period was 297 days (mean [SD]: 237.9 [130.3]). Non-Hispanic White women had the longest treatment duration (median: 309 days; mean [SD]: 241.7 [129.8] days), while non-Hispanic Black and Hispanic women had the shortest durations (246 days; 222.8 [132.4] days) and (242 days; 220.5 [131.1] days), respectively. Women living in rural areas had longer treatment durations (median: 317 days; mean [SD]: 241.2 [132.1] days) than those in urban areas (298 days; 238.1 [130.4] days). Further, women with higher annual household income levels generally had longer VMS-related treatment durations than those with lower income levels (Fig. 4).

Median durationa of VMS-related treatment utilization among women newly diagnosed with VMS by
In the Cox proportional hazards model, women aged 61–64 years had the highest adjusted risk of discontinuing VMS-related treatment (adjusted HR [95% CI]: 1.22 [1.16–1.29]; p < 0.0001). Further, non-Hispanic Black, non-Hispanic Asian, and Hispanic women all had higher adjusted risks of discontinuing treatment compared with non-Hispanic White women. The adjusted risk of treatment discontinuation was similar across income levels and regions of residence (Fig. 5).
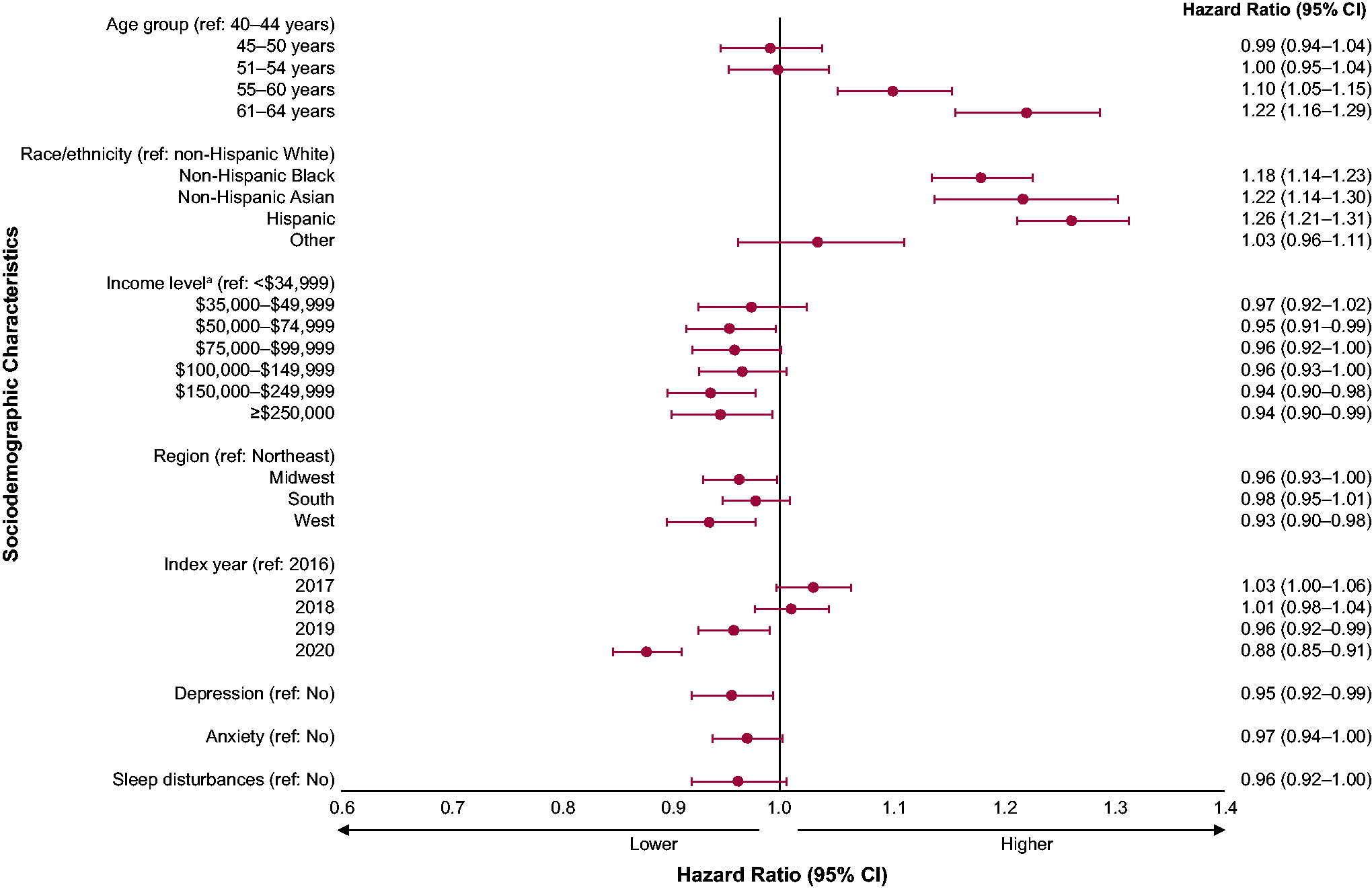
Adjusted hazard ratios for discontinuation of VMS-related treatment. aIncome level refers to annual household income. CI, confidence interval; ref, reference level; VMS, vasomotor symptoms.
Discussion
VMS are frequently experienced by women during the menopausal transition. 2 While previous research has elucidated the self-reported prevalence of VMS among women of menopausal age, 2,10 to our knowledge this study represents the first assessment of VMS prevalence using claims data. In a large, national commercial claims dataset linked to consumer data, we found that the 4-year period prevalence of diagnosed VMS in the years 2017–2020 was approximately 79 per 1,000 women aged 40–64 years. Prevalence was highest among women aged 51–54 years and lowest among those aged 40–44 years. Annual prevalence was similar across years, with the highest prevalence in 2019 (41.1 per 1,000) and the lowest in 2020 (37.9 per 1,000). We hypothesize that the lower prevalence in 2020 is an effect of a decrease in health care service use overall due to the COVID-19 pandemic. 17
Previous research has found that up to 80% of women report experiencing VMS during the menopausal transition—a considerably higher proportion than the 4-year period prevalence of diagnosed VMS of 133.2 per 1,000 (13.3%) among women aged 51–54 years in the current study. However, many women who experience VMS during the menopausal transition may not seek medical care for symptoms and therefore are not included in medical claims analyses or other studies of health system–based data. Indeed, using electronic health record data from the UK, Kiran et al. (2022) estimated that 21.1% of UK women aged 40–65 years have VMS. 18 Todorova et al. (2023) surveyed more than 12,000 postmenopausal women in seven countries and found that 15.6% reported experiencing moderate to severe VMS, a value more in line with this study’s findings. 19 Of these women, 60.1% sought advice from a medical specialist. Available data suggest that while most women may experience VMS, only a subset would characterize their symptoms as moderate to severe and seek medical care.
Our study using medical claims data highlights the sociodemographic differences in VMS prevalence that differ from those of previous research. We found that non-Hispanic White women had the highest prevalence of diagnosed VMS and significantly higher odds of receiving a VMS diagnosis than Black and Hispanic women. In contrast, analysis of data from the SWAN study has shown that significantly more Black women report VMS than those of other races/ethnicities. 2 Evidence has also shown that Black women may have more persistent VMS; the SWAN study found that median duration of symptoms was 10.1 years for Black women compared with the overall median of 7.4 years. 8 These contrasting findings point to a potential racial/ethnic disparity in the receipt of menopause-related health care. However, consistent with previous research showing reduced frequencies of VMS among Asian women, 6,10 we found that Asian women had the lowest prevalence rates of diagnosed VMS. Some evidence does suggest that reporting VMS may be influenced by cultural perceptions. 20
In the current study, women with higher levels of education and income had higher prevalence rates and significantly higher odds of receiving a VMS diagnosis. Previous research, however, has found that women with lower educational attainment report higher incidence rates of VMS. 2,21 Our data also show that women living in urban areas had higher VMS prevalence rates than those living in rural areas. Taken together, our findings and those of previous research suggest that although women in some subgroups (i.e., Black women, Hispanic women, and women with lower educational attainment) may be more likely to experience VMS, they also may be less likely to pursue or have access to consistent medical care and treatment for menopause-related concerns. Further, women with PPO or CDHP insurance plans in this study had higher prevalence rates of diagnosed VMS than those with HMO or indemnity plans, indicating a potential detection bias by insurance type. More research is needed to investigate sociodemographic disparities in the diagnosis and treatment of VMS, especially considering that much of the evidence on the menopausal transition relies on data collected in the 1990s and early 2000s. 2,5,10,21
Even though numerous therapies are available to alleviate VMS, 12 we found that nearly three quarters of women with a VMS diagnosis were taking neither hormone nor nonhormonal prescription therapies. This finding illustrates potential unmet need in the receipt of menopause-related health care and is consistent with previous work. A US-based commercial claims database analysis found that 79.5% of women with VMS had no evidence of treatment in their claims data. 22 However, claims data are unlikely to capture any nonprescription treatments for VMS, which evidence shows are frequently used. Reporting on over 1,000 US women aged 40–60 years with menopausal complaints documented in their electronic health records, DePree et al. (2023) found that 62.4% had documented use of nonprescription treatment for VMS. 23 Many women also report hesitancy to use hormone therapy owing to concerns about side effects and long-term risks. 6 Indeed, a 2022 survey study reported that more than half of physicians do not prescribe hormone therapy because of patient concerns with long-term risks. 24 Moreover, some potential contraindications for hormone therapy, such as history of breast cancer, prevent women from receiving hormone therapy. 11 Previous research has shown that White women report higher rates of hormone therapy use than Black and Hispanic women, 13,25 and our data also show that Black, Asian, and Hispanic women with VMS all had a higher risk of discontinuing VMS-related treatment than their non-Hispanic White counterparts. The mechanisms of racial, ethnic, and other sociodemographic disparities in receiving care for VMS are not fully understood.
Several limitations should be considered when interpreting findings presented here. We identified demographic factors associated with the 4-year period prevalence of VMS; however, we did not measure the association of such characteristics with incident (i.e., new) cases of VMS. Thus, our findings could indicate a relationship between these factors and the duration rather than occurrence of VMS. PharMetrics Plus is a large medical claims database covering of all US Metropolitan Statistical Areas and including largely commercially or self-insured individuals. Thus, findings should be interpreted considering these inherent selection biases, as uninsured women and women with public insurance (e.g., Medicaid, Medicare) could not be evaluated. As previously noted, women with PPO or CDHP insurance plans in this study had higher prevalence rates of diagnosed VMS than those with HMO or indemnity plans, suggesting possible detection bias by insurance type. Black women were also underrepresented in this study compared with the general US population of women: while approximately 13% of all US women aged 18–64 years are Black, Black women comprised 6.8% of women diagnosed with VMS in this study. 26 Similarly, the US Department of Agriculture estimates that 13.8% of the US population resides in rural areas; in this study, 1.4% of women with diagnosed VMS were living in areas considered rural. 27
Although we linked claims data with consumer data to analyze key sociodemographic characteristics, other factors related to VMS, such as smoking status, body mass index, and menopausal transition stage, could not be explored. Residual confounding from these factors may account for some of the sociodemographic differences observed in this study. It should also be noted that some SERMs, which were included as VMS-related treatments, may exacerbate VMS. However, some SERMs (e.g., Duavee, a combination of bazedoxifene and estrogen) have been shown to improve VMS. 28 Including all SERMs as VMS-related treatment may have produced an effect such that some women included in the study experienced exacerbation of VMS, and further research assessing VMS-related treatment outcomes should consider evaluating individual SERMs separately. However, considering that VMS are generally underdiagnosed, and that many affected women remain untreated, we sought to capture a broad range of treatments that may have been used by providers to treat VMS.
Finally, the use of claims data to identify a VMS diagnosis has limitations, as no ICD-10-CM codes are specific to VMS. Thus, to identify women diagnosed with VMS, we developed an algorithm to identify patients using a combination of codes that required meeting either of two conditions. It is possible that this classification method overestimated VMS prevalence by capturing some women who were menopausal during the study period but not actively experiencing VMS. However, we believe our method was robust given that up to 80% of women of menopausal age report experiencing VMS. 2 The approach used in this study has also been applied previously by Shiozawa et al. (2024) to identify women diagnosed with VMS in commercial claims data. 22
Conclusion
Using US commercial claims data linked with consumer data, this study identified sociodemographic differences in the prevalence of diagnosed VMS and in the risk of VMS-related treatment discontinuation among women of menopausal age. Data show a lower prevalence of diagnosed VMS and a higher risk of treatment discontinuation among racial/ethnic minorities and among women with lower levels of education and income. These findings point to potential underdiagnosis of VMS, suggesting that women in vulnerable populations have unmet needs in menopause-related health care. More research is needed to understand these potential disparities and how they may be ameliorated.
Footnotes
Acknowledgments
Medical writing and editorial support were provided by Kelly Birch, MPH, Tulika Bhushan Bahukhandi, RPh, MS, and LeeAnn Braun, MPH, MEd, of Echelon Brand Communications, LLC, an OPEN Health company, and funded by
Authors’ Contributions
G.R.-D.: Investigation; data curation; writing (original draft); and writing (review and editing); supervision. M.A.: Conceptualization; methodology; software; formal analysis; investigation, writing (original draft); writing (review and editing); supervision; and project administration. A.S.: Conceptualization; methodology; software; formal analysis; investigation; writing (original draft); writing (review and editing); supervision; and project administration. R.D.: Formal analysis; investigation; writing (original draft); writing (review and editing); supervision; and project administration. C.Y.: Investigation; writing (original draft); writing (review and editing); supervision; and project administration. J.Y.: Investigation; writing (original draft); writing (review and editing); supervision; and project administration. S.M.: Investigation; writing (original draft); writing (review and editing); supervision; and project administration.
Author Disclosure Statement
G.R.-D.: Received study funding and medical writing/editing support from
Data Availability Statement
Researchers may request access to anonymized participant-level data, survey-level data, and protocols from Astellas-sponsored clinical trials at www.clinicalstudydatarequest.com. For the Astellas criteria on data sharing see: ![]() .
.
Funding Information
The study was sponsored by Astellas Pharma Inc.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.