
Abstract
Objective:
To assess the impact of historical redlining on the risk of pregnancy complications and adverse birth outcomes in Massachusetts (MA) from 1995 to 2015.
Methods:
In total, 288,787 pregnant people from the MA Birth Registry had information on parental characteristics, pregnancy factors, and redlining data at parental residences at the time of delivery. Historic redlining data were based on MA Home Owners’ Loan Corporation (HOLC) security maps, with grades assigned (A “best,” B “still desirable,” C “definitely declining,” and D “hazardous”). We used covariate-adjusted binomial regression models to examine associations between HOLC grade and each chronic condition and pregnancy/birth outcome.
Results:
Living in HOLC grades B through D compared with A was associated with an increased risk of entering pregnancy with chronic conditions and adverse pregnancy/birth outcomes. The strongest associations were seen with pregestational diabetes (adjusted risk ratio [RR] Grade D: 1.7, 95% confidence interval [CI]: 1.3, 2.4) and chronic hypertension (adjusted RR Grade D: 1.5, 95% CI: 1.1, 1.9).
Conclusions:
Historical redlining policies from the 1930s were associated with adverse pregnancy outcomes and chronic conditions; associations were strongest for chronic conditions in pregnancy.
Introduction
The United States (U.S.) has among the most striking disparities in pregnancy complications and adverse birth outcomes among developed countries. Despite race being a social and not biological construct, non-Hispanic Black and Indigenous pregnant people are 2 times as likely to experience a hypertensive disorder of pregnancy and 50% more likely to have a preterm birth. 1,2 Both non-Hispanic Black and Asian pregnant people are 2 times more likely to deliver a low birth weight infant. 1 Even before pregnancy, non-Hispanic Black individuals are 2.5 times more likely to enter pregnancy with chronic hypertension 3 and over 70% more likely to enter pregnancy with diabetes; 4 both are conditions that impact pregnancy outcomes and the long-term health of both pregnant people and their children. Drivers of these persistent and increasing disparities have been well-documented and include decreased access to health-promoting resources (medical care, healthy foods, physical activity), discrimination in health care services, and increased psychosocial stress. 5 –8 Although there has been a focus on individual-level drivers that may contribute to the observed disparities in health outcomes, it is important to consider upstream risk factors when identifying solutions to persistent disparities present at the population level. 9 Structural racism has received critical attention as a dominant upstream risk factor of health disparities, 10 –12 and as such, a growing number of studies have evaluated the association between structural racism and adverse health outcomes, including pregnancy outcomes. 13 –15
Dating back to the 1930s, historic residential redlining was a legalized form of structural racism that involved systematically limiting lending to and homeownership by people of color and immigrants, ultimately reducing the opportunity to build wealth and perpetuating material and social deprivation of these populations. 16 –18 The Home Owners Loan Corporation (HOLC) produced ranks for neighborhoods on classifying their suitability for refinancing which became known as historic residential redlining grades. Communities comprised of lower-income, non-White, and/or immigrant populations were assigned a grade of D or “hazardous,” whereas predominantly White and U.S. born communities were generally assigned a grade of A or “best.” These communities graded as D were represented by red areas on HOLC security maps, giving rise to the word redlining. 17 Although banned in the 1960s, studies show that historic redlining is linked to a variety of adverse health outcomes in the present day, including birth outcomes, such as preterm birth and low birth weight. 13 –15 For example, in a New York City-based study conducted between 2013 and 2017, the odds of preterm birth were 1.6 times higher among people living in grade D communities compared with those living in grade A communities. 13
Although studies have examined the association between historic redlining and birth outcomes, few studies, to our knowledge, have also evaluated the associations of historic redlining with chronic (i.e., chronic hypertension and pregestational diabetes) and acute conditions of pregnancy (i.e., gestational diabetes and hypertensive disorders of pregnancy). These conditions may impact birth outcomes, as well as parental and child health later in life. To address this gap, we examined the associations between historic redlining and chronic conditions affecting pregnant people, pregnancy complications, and birth outcomes in almost 300,000 pregnancies in Massachusetts (MA) from 1995 to 2015. The findings from this study may elucidate some of the structural drivers of persistent pregnancy health disparities that could benefit from risk reduction efforts aimed at targeting the lasting effects of these historic policies.
Methods
Study population
We analyzed all singleton live births included in the Massachusetts Birth Registry (MABR) that occurred from January 1, 1995, through December 31, 2015, from the Department of Public Health’s Registry of Vital Records and Statistics. This dataset included information on sociodemographic factors, including race/ethnicity, education, maternal age, Medicaid status, and marital status. In addition, the records included existing medical conditions, as well as pregnancy and birth outcomes.
Data were available for 1,199,288 live births between 1995 and 2015. We excluded individuals without data on parental residence at birth (n = 25,181) and those without data on birth outcomes (n = 38,495). Next, we excluded individuals with gestational age <22 weeks (n = 1,004) and >42 weeks (n = 8,668) and birth weights <1st percentile (< 1,417 grams, n = 11,561) and > 99th percentile (> 4,593 grams, n = 10,569). We also excluded multiple births (2 or more fetuses, n = 46,073). Lastly, we excluded individuals who did not live in historically graded communities (n = 768,950), as done in previously published studies. 13 However, in Table 1, we present the descriptive statistics of the births among parental residences in HOLC-graded and nongraded communities. The total analytic sample for the multivariate analyses was 288,787 live births. Supplementary Figure S1 details the exclusions.
Descriptive Statistics of Births in Massachusetts from 1995 to 2015
Historical residential redlining
Historical residential redlining was assessed through 1938 HOLC security maps that assigned grades (A–D) based on existing neighborhood home values, environmental hazards, and racial composition. 17 Neighborhoods considered “best” (Grade A—green) comprised of higher socioeconomic status (SES) or “upper class” non-Hispanic White families, “still desirable” (Grade B—blue) comprised of “middle class” non-Hispanic White families, “definitely declining” (Grade C—yellow) comprised of lower-SES or “lower class” non-Hispanic White families, and “hazardous” (Grade D—red) comprised of lower SES and non-Hispanic Black, Hispanic, Asian, Jewish, and immigrant families. We obtained shapefiles of Massachusetts (MA) HOLC Security Maps from the University of Richmond’s Mapping Inequality Project. 17 We superimposed geocoded parental addresses at the time of birth onto historical HOLC security maps to assign each birth a HOLC grade. We assigned births where the parental address at the time of birth was not encompassed in HOLC-graded regions as “Not Classified,” as done in previous research. 13 Figure 1 provides an example of historic redlining for the Greater Boston Area.
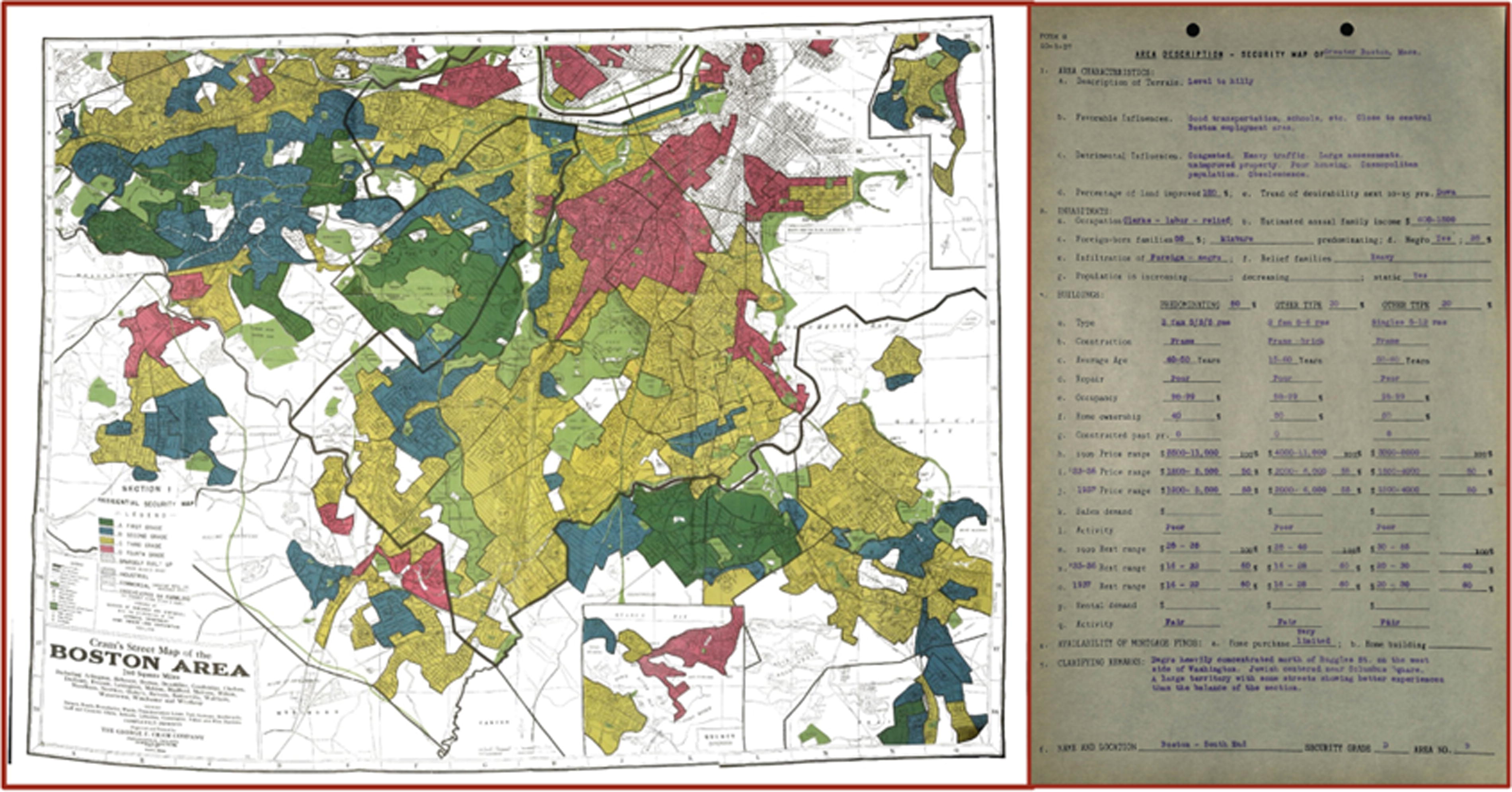
The Home Owners’ Loan Corporation (1930s) redlining map of the Greater Boston area and supporting document of redlined area in the South End. Green indicates “Best” and red indicates “Hazardous” or redlined.
Outcomes
Pregestational and gestational diabetes
In pregnancy, it is standard care to evaluate and manage both pregestational and gestational diabetes to maintain the health of the pregnant person and developing child. 19 From MABR, we abstracted information on chronic conditions and pregnancy complications. Based on criteria from the American Diabetes Association (ADA), pregestational diabetes is defined as an elevated fasting blood glucose level ≥126 milligrams/deciliter before pregnancy or during the first trimester. 20 For gestational diabetes, we defined it based on the ADA’s definition as any form of glucose intolerance diagnosed in the second or third trimester of pregnancy.
Hypertensive disorders of pregnancy and chronic hypertension
Hypertensive disorders of pregnancy and chronic hypertension are routinely managed as a part of obstetrics care, and blood pressure is monitored throughout pregnancy. Hypertensive disorders of pregnancy are defined as gestational hypertension and preeclampsia. The International Society for the Study of Hypertension in Pregnancy defines gestational hypertension as elevated blood pressure measures (≥140 mmHg systolic blood pressure or ≥90 mmHg diastolic blood pressure) with onset after 20 weeks of gestation without proteinuria. Preeclampsia is defined by these same elevations in combination with proteinuria. Chronic hypertension is defined by these same blood pressure elevations with onset that precedes 20 weeks gestation, which could include individuals currently taking antihypertensives.
Birth outcomes
We also obtained data from MABR on our birth outcomes of interest which included gestational age (estimated using self-reported last menstrual period and measured in weeks at time of birth) and birth weight (measured in grams at time of birth). In addition, we collected data from MABR on our secondary birth outcomes of interest: preterm birth (PTB, <37 weeks gestation), low birth weight (LBW, <2,500 grams), small for gestational age (SGA, birth weight less than the sex-specific 10th percentile), and large for gestational age (LGA, birth weight greater than the sex-specific 90th percentile). We further categorized PTB as very preterm (<32 weeks gestation), moderately preterm (32–34 weeks gestation), and late preterm (34–36 weeks gestation) and birth weight as very LBW (<1,500 grams) and LBW (1,500-2,500 grams), based on previous classifications. 21,22 We were unable to separately include extremely preterm (<28 weeks gestation) and extremely low birth weight (<1,000 grams) based on the small sample size of both categories.
Statistical analyses
We calculated descriptive statistics and fit separate binomial regression models for each dichotomous outcome to evaluate their associations with HOLC grade (A–D). HOLC grade A, indicating “best,” was selected as the reference category for all analyses. We fit separate linear regression models for continuous outcomes. We included the following covariates as predictors of the pregnancy and birth outcomes of interest selected a priori: parental race/ethnicity (non-Hispanic White, non-Hispanic Black, Asian/Pacific Islander, Hispanic, Other), educational attainment (less than high school, high school degree or GED, some college, bachelor’s degree, graduate degree), Medicaid coverage (yes/no), married (yes/no), and gestational weight gain (pounds). To account for the role of current day neighborhood-level characteristics, specifically racialized economic segregation, we included census tract level index of concentration at the extremes (ICE) race/ethnicity plus income as a covariate for our primary outcome models, which is described in more detail elsewhere. 23
In sensitivity analyses, we fit separate multivariable, multinomial logistic regression models for PTB categories (very preterm, moderately preterm, and late preterm) and LBW categories (very LBW and LBW). In addition, we assessed if age was an effect modifier by stratifying by median parental age. Given that missingness was uniformly low across all covariates (< 5%), we conducted a complete case analysis. All statistical analyses were performed in R Version 3.5.1.
Results
Table 1 summarizes the parental sociodemographic characteristics, pregnancy complications, and birth outcomes overall and by HOLC grade (A–D and “Not Classified”). Of the HOLC-assigned births, 2.1% occurred in HOLC grade A (“Best”), 14.5% in HOLC grade B (“Still desirable”), 57.9% in HOLC grade C (“Definitely declining”), and 25.5% in HOLC grade D (“Hazardous”). In terms of chronic conditions and pregnancy complications, 1.4% had pregestational diabetes, 4.1% had gestational diabetes, 1.6% had chronic hypertension, and 3.5% had hypertensive disorders of pregnancy. Differences in current parental sociodemographic characteristics by HOLC grade were observed.
Chronic conditions and pregnancy outcomes
Table 2 presents the associations between HOLC grades and each chronic condition and pregnancy outcome. HOLC grades B, C, and D were positively associated with each of the adverse chronic conditions and pregnancy outcomes. Specifically, pregnant people living in areas with a HOLC grade D compared with A had a 70% increased risk of pregestational diabetes (adjusted for parental characteristic [PC] only risk ratio [adjusted RR]: 1.7; 95% confidence interval [CI]: 1.3, 2.4) and a 50% increased risk of chronic hypertension (adjusted PC RR: 1.5; 95% CI: 1.1, 1.9). In addition, pregnant people in HOLC grade D compared with A had a 50% increased risk of gestational diabetes (adjusted PC RR: 1.5; 95% CI: 1.3, 1.8) and a 20% increased risk of hypertensive disorders of pregnancy (adjusted PC RR: 1.2; 95% CI: 1.1, 1.5). Interestingly, HOLC grade C consistently presented the highest RRs for chronic conditions and pregnancy complications compared with HOLC grade A, though the CIs between HOLC grades C and D overlapped. The strongest associations were for the chronic disease outcomes, pregestational diabetes (adjusted PC RR HOLC grade C: 1.9; 95% CI: 1.4, 2.5) and chronic hypertension (adjusted PC RR HOLC grade C: 1.7; 95% CI: 1.3, 2.2). Associations were elevated but slightly more modest for individuals living in HOLC grade B versus A. Compared with the models adjusted for parental characteristics, the unadjusted models for all pregnancy outcomes presented similar RRs. The models adjusted for ICE only, and parental characteristics with ICE were generally attenuated compared with the unadjusted and adjusted for parental characteristics only models.
Covariate-Adjusted and Unadjusted Risk Ratios with 95% Confidence Intervals for Pregnancy Outcomes and Chronic Conditions (Pregestational Diabetes, Gestational Diabetes, Chronic Hypertension, and Hypertensive Disorders of Pregnancy) in HOLC Grade B-D Areas Compared to HOLC Grade A
Adjusted models controlled for parental age, race/ethnicity, education, Medicaid coverage status, and parental weight gain.
Adjusted models controlled for Index of Concentration at the Extremes (ICE) race/ethnicity plus income at the census tract level.
Adjusted models controlled for parental characteristics (parental age, race/ethnicity, education, Medicaid coverage status, and parental weight gain) and ICE race/ethnicity plus income.
Birth outcomes
Table 3 presents the estimates and 95% CIs for the associations between HOLC grade and our primary birth outcomes. Both HOLC grades C and D showed similar decreases in birth weight relative to HOLC grade A (adjusted PC estimate HOLC grade C: −22.1 grams, 95% CI: −34.9, −9.4; adjusted PC estimate HOLC grade D: −25.9 grams, 95% CI: −39.0, −12.8). These estimates were attenuated in all adjusted models (parental characteristics only, ICE only, parental characteristics with ICE), however, still presented notable decreases in birth weight comparing HOLC grades B through D to HOLC grade A. No notable associations were identified between HOLC grade and gestational age. Supplementary Table S1 presents the RRs of our secondary birth outcomes of PTB, LBW, SGA, and LGA in HOLC grades (B–D) compared with a HOLC grade of A. We observed a 20% increased risk of SGA in HOLC grades C and D areas compared with HOLC grade A areas (adjusted PC RR HOLC grade C: 1.2; 95% CI: 1.1, 1.4 and adjusted PC RR HOLC grade D: 1.2; 95% CI: 1.1, 1.4).
Covariate-Adjusted and Unadjusted Differences in Mean Gestational Age at Delivery (Weeks) and Birth Weight (g) and 95% Confidence Intervals in HOLC Grade B-D Areas Compared to HOLC Grade A
Adjusted for parental age, race/ethnicity, education, Medicaid coverage status, and gestational weight gain.
Adjusted models controlled for Index of Concentration at the Extremes (ICE) race/ethnicity plus income at the census tract level.
Adjusted models controlled for parental characteristics (parental age, race/ethnicity, education, Medicaid coverage status, and parental weight gain) and ICE race/ethnicity plus income.
Sensitivity analysis
In the sensitivity analyses examining LBW and PTB categories (Supplementary Table S2), we did not find any notable associations with HOLC grade after adjustment for parental characteristics. In addition, Supplementary Table S3 presents our sensitivity analyses examining all chronic conditions, pregnancy complications, and birth outcomes stratified by median parental age. Among older pregnant people (> median: 30.6 years), we found a 29.1 grams (95% CI: −43.6, −14.7) decrease in birth weight and a 38.3 grams (95% CI: −53.5, −23.2) decrease in birth weight for HOLC grades C and D, respectively, compared with HOLC grade A. Comparatively, among those younger than 30.6 years, decreases in birth weight were also reported, though the confidence intervals were wide. In addition, older pregnant people in HOLC grades C and D had a 30% increased risk of SGA (adjusted PC RR HOLC grade C: 1.3; 95% CI: 1.1, 1.4 and adjusted PC RR HOLC grade D: 1.3; 95% CI: 1.2, 1.5). Among HOLC grade D areas, younger pregnant people showed a stronger association between HOLC grade and pregestational diabetes (adjusted PC RR: 2.6; 95% CI: 1.0, 7.0). Attenuated positive associations were observed for older pregnant people when looking at pregestational diabetes comparing HOLC grade D with grade A (adjusted PC RR: 1.6; 95% CI: 1.2, 2.3). Associations were similar for younger and older pregnant people when evaluating HOLC grades and both chronic hypertension and hypertensive disorders of pregnancy. The estimates from the unadjusted models were generally stronger and/or similar to the estimates from the adjusted models, with overlapping CIs.
Discussion
In this study evaluating historical redlining from the 1930s and current parental health outcomes in close to 300,000 live births in the state of Massachusetts, we found associations between HOLC grade B through D communities and several chronic conditions and pregnancy/birth outcomes, notably the chronic conditions of pregestational diabetes and chronic hypertension. We also found significant associations with birth weight and SGA. We did not find notable associations with PTB or LGA. After adjusting for racialized economic segregation using ICE, the estimates were attenuated yet generally consistent with the unadjusted estimates. These findings present evidence of associations between historic redlining and current day pregnancy conditions and birth outcomes that are independent of certain current day characteristics. These findings suggest that racist policies from the 1930s may still impact pregnancy outcomes and the health of individuals living in redlined neighborhoods before their pregnancy with implications for adverse health outcomes for both pregnant people and their children. This analysis adds to the literature on the long-term effects of structural racism on health, with a focus on chronic conditions that have not been previously examined.
Emerging evidence has shown that neighborhoods assigned HOLC grades C and D almost a century ago remain mostly home to low-SES communities of color in the present day. 12,24 Redlined communities are more likely to experience higher exposure to air pollution, less access to green space, greater proximity to industry, toxic waste sites, and flood zones, as well as poorer housing quality and health care infrastructure. 25 –28 With structural racism contributing both to decreased access to health-promoting resources and higher toxic environmental exposures, living in these neighborhoods may contribute to the disproportionate burden of chronic conditions that impact reproductive outcomes. 29,30 Indeed, the present study found that living in areas assigned HOLC grades B through D had an increased risk of chronic and acute pregnancy complications and birth outcomes.
A growing body of evidence across the U.S. suggests that historical residential redlining is associated with a variety of birth outcomes, 13 –15 where current day racial/ethnic disparities persist. 1,31 Nardone et al. reported positive associations between higher HOLC grades (C versus B and D versus C) and adverse birth outcomes, including PTB and SGA, in three metropolitan cities in California from 2006 to 2015. 14 Our results supported a portion of these findings, and we observed a 20% increased risk of SGA in HOLC grades C and D regions compared with HOLC grade A regions. Other studies from across the U.S. also reported an increased risk of preterm birth among HOLC grades B through D. 13,15 In contrast, our study did not observe a significantly increased risk of preterm birth among HOLC grade B through D regions compared to HOLC grade A regions. This finding may be driven by the small number of PTB infants reported in HOLC grade A regions in this study or differences in risk factors for the population living in Massachusetts relative to other states. For example, compared with the U.S. population, pregnant individuals living in Massachusetts are older (27.7 years in Massachusetts compared with 25.0 years for the U.S. overall) 32 and have less obesity (20.8% obesity in Massachusetts compared with 26.1% for the overall U.S. population). 33 Differences in access to healthcare or other health-promoting resources may also contribute to our reported findings. 34,35 Furthermore, adjusting for ICE race/ethnicity plus income, a measure of racialized economic segregation, resulted in attenuated yet consistent findings with our other analyses, indicating that the effects of current day racialized economic segregation may only partially explain the association between historic redlining and present day chronic and acute parental and birth outcomes. This finding of attenuated associations between historic redlining and birth outcomes after adjusting for current census tract racialized economic segregation was also reported in Kreiger et al. 13
A number of potential pathways could link historic redlining with chronic disease, as well as adverse pregnancy outcomes. One potential pathway is the weathering effect, which is the long-term impact of cumulative adverse environmental health exposures that can translate to increased psychosocial stress, as well as alterations in biological processes. 36 –39 Indeed, elevated cortisol levels, increased blood pressure reactivity, and cytokine production, as well as higher waist-to-hip ratio and elevated glycated hemoglobin levels have all been linked to poor social and environmental factors. 36 –39 Interestingly, the present study shows the strongest associations between historic redlining and chronic conditions associated with diabetes and hypertension among younger pregnant people. These findings may suggest that historic redlining contributes to higher cumulative adverse exposures that alter the metabolic aging process.
Qualitative research allows us to understand some of the specific challenges and experiences that communities face, particularly as they relate to the long-term distribution of resources that intersect with race, class, and nativity. For historically red- and yellow-lined communities, these experiences may be related to access to health-promoting resources and the excess burden of health-detrimental factors that may contribute to psychosocial stressors and higher exposure to environmental pollutants with downstream health consequences. Relevant to MA, one analysis explored access to healthcare among Brazilian immigrant families in Brighton and Somerville, MA and while reporting generally high satisfaction with the U.S. healthcare compared to Brazil, barriers were identified including communication, discrimination, and cultural competency. 40 Indeed, this qualitative research was focused on a specific community in MA; however, Brighton was historically graded by HOLC as C and D, and Somerville was graded as B and C, 17 which could raise questions for future research about access to health care among these non-HOLC grade A neighborhoods/cities. In addition, an analysis exploring the experiences of residents living in Ironbound, an environmental justice community in New Jersey, brought to light certain themes including being distressed by known pollution sources and being worried about the health effects of pollution. 41 The Ironbound neighborhood of Newark was historically graded D by HOLC. 17 In addition to documenting barriers and experiences of residents living in these communities, future qualitative research should be used to also identify solutions and potential interventions.
Several limitations of this study are important to consider. First, the spatial coverage of the Massachusetts HOLC Security Maps was limited to primarily the Greater Boston area, which may have introduced selection bias. However, the sociodemographic characteristics of those with missing HOLC grades did not differ from those living in HOLC-graded areas (A–D). Second, these findings may not apply to those living outside of Boston or urban areas, given that these maps were primarily used in urban settings. Third, we only had access to information on parental residential address at time of birth, which may not reflect the longest residence and exposures relevant to the evaluated health outcomes. However, parental address at the time of birth may be an important risk factor for conditions occurring in late pregnancy, particularly preterm birth and birth weight measures. Fourth, we did not have unique identifiers that provided information on multiple births delivered by the same pregnant person, a risk factor for adverse birth outcomes. Therefore, we were unable to account for prior history of pregnancy complications and adverse pregnancy outcomes in our analyses. Fifth, we used parental Medicaid coverage status and marital status as imperfect proxies for parental SES.
Despite these limitations, this study has several strengths. First, this study evaluated a large, state-wide dataset, MABR, and historical redlining data. Second, this is among the first studies to evaluate the association between historical redlining and chronic conditions in pregnant individuals, including chronic hypertension and pregestational diabetes, which are associated with inequities in parental mortality and cardiovascular disease. 42,43 Third, we evaluated other important pregnancy complications, including gestational diabetes and hypertensive disorders of pregnancy. Lastly, we examined effect modification by age, allowing us to elucidate differences in age as it related to HOLC grade and chronic conditions in pregnancy.
Conclusions
Our findings present evidence that in MA, historical redlining policies continue to play a role in pregnancy complications and adverse birth outcomes. Of importance, chronic conditions before pregnancy appeared to be most strongly associated with historical redlining. Our findings may help to guide interventions for communities impacted by these racially biased policies, specifically as it relates to preconception care and the need for evaluating resilience factors, such as social networks, green space, and access to health-promoting resources that could offset the perinatal health impacts of these historical policies in the current day.
Footnotes
Authors’ Contributions
M.C.: study design, analysis, article writing, and editing. S.P.: study conception and design, analysis, and article drafting. E.W.: assistance with data analysis, data management interpretation, article editing. J.L.S.: analysis planning, interpretation of study results, and article editing. E.C.: assistance with data analysis and mapping, data management and interpretation, and article editing. L.P.T.: biostatistical support for conceptualization of contemporary factors, data interpretation, and article editing. J.S.: study conception and design, data management and interpretation, article writing and editing. T.J.T.: study conception and design, data analysis and interpretation, article writing and editing.
Author Disclosure Statement
The authors have no potential or actual conflicts of interest to report.
Funding Information
This work was supported in part by grants from the
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.