
Abstract
Background:
Retail health clinics offer easy access and lower costs in seeking nonemergent and usually focused care. The objective of this observational study was to describe the use of retail clinic services by women at MinuteClinic at CVS, the largest network of retail clinics in the United States.
Methods:
The retail clinic’s large database included complete national data for every in-person encounter as recorded on the same electronic health record. Virtual care and pharmacist-delivered services like COVID-19 testing were excluded from the analysis. The primary reason for the visit and the patient’s age group (<15, 15–44, 45–64, ≥65 years) and self-reported sex were recorded at each encounter from the most recent 5 years (January 1, 2018, to December 31, 2022).
Results:
There were 17,969,483 encounters by women seeking care, and women ≥15 years old were more likely than men to attend the clinics. Half of all encounters (50.6%) were for non-gynecologic acute care, whereas one-third (33.6%) dealt with either an infection or the need for a vaccination. Gynecologic reasons involved 5.6% of all encounters in women ≥15 years of age. No obstetrical care was provided except for pregnancy testing with referral, acute non-obstetric needs, or guideline-recommended vaccinations.
Conclusion:
Women, especially of reproductive age, are more inclined than men to seek care at retail clinics. Acute care is the most common need, although requests for immunizations, infection screening and treatment, and reproductive health issues occurred often.
Introduction
Clinics located in retail stores with adjacent pharmacies have steadily grown in the health care marketplace since their inception in 2000. 1 More than 2,300 retail clinics operate in 43 states in the United States. 2 Typical services include acute care, minor illnesses and injuries, immunizations, and preventive screening. Clinics are staffed by licensed advanced practice providers, such as nurse practitioners and physician associates, and supervised by physicians in accordance with state regulations.
The appeal of retail clinics includes access to convenient quality care services with fixed and transparent low prices. 3 These characteristics may be particularly appealing to women who are more influenced by the convenience because they deal with constraints such as extended family and work responsibilities. 4 The objective of this observational study was to describe the use of retail clinic services by women at MinuteClinics inside CVS store locations, the largest network of retail clinics in the United States.
Materials and Methods
The study was deemed exempt by the WIRB-Copernicus Group (WCG) Institutional Review Board and was granted a full HIPAA waiver of authorization. MinuteClinics gave permission for the authors to use their database of de-identified aggregate data. This large database included complete national data for every in-person encounter as recorded on the electronic health record.
MinuteClinic deploys Epic Systems Corporation (Epic) software that captures demographic, insurance, and clinical encounter data. The Epic system is programmed with clinical workflows and embedded decision support tools (e.g., U.S. Preventive Services Task Force, relevant specialty guidelines) for standardization of evaluation and treatment protocol adherence. Data analytic tools include Epic Slicer Dicer and Tableau software (Salesforce) for analysis of service encounters and volume data.
The primary reason for the visit and the patient’s age group (<15, 15–44, 45–64, ≥65 years) and self-reported sex were recorded at each encounter from the most recent 5 years (January 1, 2018, to December 31, 2022). The data included the peak years of the COVID-19 pandemic (2020, 2021). Primary reasons for women to seek care were subdivided into the most common categories: acute care, request for immunizations, presumed infection, health maintenance and preventive care, and other categories. Examples of conditions seen in each category are shown in Box 1. Reproductive health care involved concerns related to the lower abdomen and reproductive tract. Virtual care and pharmacist-delivered services like COVID-19 testing were excluded from the analysis.
Results
There were approximately 1,100 MinuteClinics located in predominantly metropolitan areas of 35 states and the District of Columbia. There were 28,974,891 patient encounters during this 5-year period, of which 17,969,483 (62.0%) were with women. This percentage (61.2%) remained steady during the COVID-19 pandemic.
The distribution of encounters was wide-ranging according to the age group (Fig. 1). Except for an equal distribution of encounters for those of age <15 years, women were more likely to receive services than men in all adult age groups. Encounters were most common in the 15- to 44-year-old group compared with all other age groups combined.
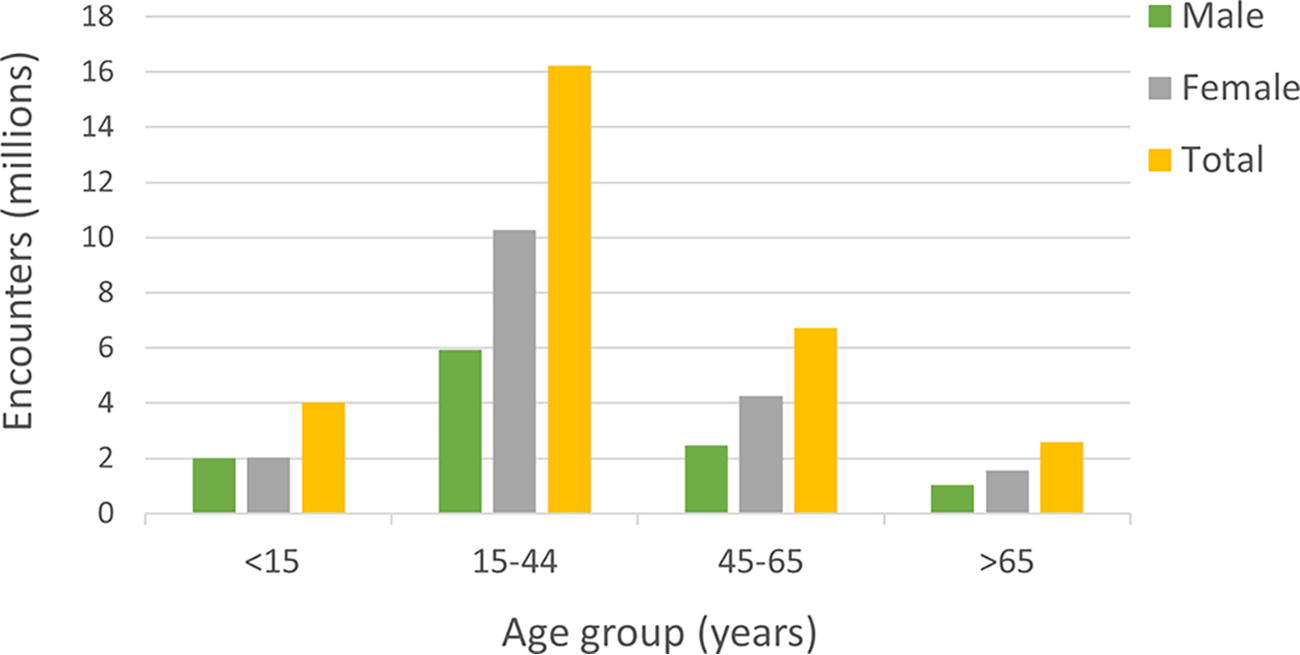
Comparison between MinuteClinic encounters by patient sex and age, 2018–2022.
The primary reasons for women to seek care are shown in Table 1. An overlap in categorizing the primary reasons for the visit was infrequent (4.2%). Acute care requests were most common, accounting for about half of all encounters, regardless of the age group. A request for non-COVID-19 immunizations was the next most common reason. The third most frequent reason was the treatment of a presumed infection. The percentage of suspected infections was low for either the urinary tract (19.9%) or sexually transmitted infections (STIs; 2.9%). Health maintenance and preventive care were requested mostly by <45-year-olds. Other service types such as behavioral health, chronic illness, and medication management were least commonly sought and mostly by ≥45-year-olds.
Distribution of Primary Reasons for Clinic Visits by Women in Each Age Group
Data are presented as percentages in each age group (years).
Evaluation of a reproductive health condition was the most frequent among women of ages 15–44 and constituted 5.6% of all encounters in that age group. Conditions that required care were in the following declining order: urinary tract infections, contraception, screening for STIs, vaginitis, pregnancy testing and referral, cervical cancer screening, and menstrual cycle disorders. Screening for cervical cancer began in 2020 and has scaled up at most clinics today. No obstetrical care was provided except for on-site urine pregnancy testing with referral, non-obstetric acute needs, and pregnancy-approved vaccinations. All blood, cervicovaginal, and urine specimens are sent to a national reference laboratory.
Contraception counseling and treatment services included all hormonal oral, vaginal, and injectable (Depo-Provera) methods. Long-acting reversible implantation contraception and intrauterine devices (IUD) were unavailable. Despite this, services included counseling about the pros and cons of IUD and implant options and referring as desired.
Counseling, screening, and referral for treatment for STIs included HIV and syphilis. Screening and antimicrobial treatment were available for chlamydia and gonorrhea (pharyngeal, vaginal, and rectal specimen collection). Counseling and suppressive therapy for genital Herpes simplex was available. Evaluation of vulvovaginitis included screening with a vaginal culture and DNA probes. STI screening results were routinely reported to the patients, and positive results were reported to state health departments as required by law.
Discussion
Retail health clinics represent a growing model for health care delivery. This investigation from the largest national retail health provider demonstrated that a high proportion of in-person encounters were by adult women, especially those of reproductive age. Their desired care was primarily for acute, nonemergent conditions without the need for a return visit. This finding is similar to a recent analysis that found that, when compared to men, women had a 24% higher rate of use of urgent care centers or retail health clinics in the past 12 months. 5 The study timeframe included peak COVID-19 pandemic years, which posed access barriers to in-person care, yet more women came to the clinics than men.
Consumer websites list women’s health services at MinuteClinics. The website design and content have changed over time. Reproductive health services are shown to include family planning, menstrual health, STI screening and treatment, vaginitis, UTI evaluation and treatment, mastitis, and vaccinations. It is premature to comment about an increase in reproductive health services because of the recent phasing in cervical cancer screening.
The study included a period when COVID-19 was a pandemic. Routine screening was done through the pharmacy only. Written and verbal counseling was provided by the pharmacists about when the result would be reported and what was to be done if the results were positive or negative. MinuteClinics were not to be used as a site for COVID-related complications, so data were not reported in this report.
Cost is an important consideration for any health care delivery system. MinuteClinic serves a wide payer mix including commercial and government (Medicaid and Medicare) plans. MinuteClinic serves self-pay patients and provides posting of transparent pricing for individual services. Retail health is, in many clinical situations, less costly compared with urgent care centers and emergency departments. 2,6,7 The current study was not intended to examine the costs of care delivered for specific reproductive health care. A future investigation comparing cost and reimbursement between retail clinics and obstetrician-gynecologist (OB-GYN) clinics for specific reproductive health needs would be informative.
A limitation of the present study was the inability to track referrals to OB-GYN or other specialist offices. Although data about referral were usually reported, a specialty may not have always been identified. Tracking of referrals was most common with clinics that shared the same electronic medical record system. Furthermore, MinuteClinics do not routinely capture whether patients complied with the referral. This time-consuming limitation is not different from other health care settings. It may be worthwhile to examine success with referrals for specific reproductive health needs.
No radiologic studies are available at MinuteClinics, including chest X-rays and intravaginal and abdominal ultrasound exams of the pelvis. Instead, patients with conditions involving major trauma or respiratory difficulty would require X-rays and would be referred to their primary provider, urgent care center, or emergency department. Diagnostic tests at MinuteClinics are comparable to most standard clinics and include the ability to send samples (e.g., blood, urine, throat swab) to reference laboratories (e.g., Quest, LabCorp).
Women accessing care at retail clinics will likely grow owing to easier unscheduled access, convenience, and affordability. 6 –8 Establishing relationships between nearby women’s health care clinics and retail clinics can be mutually beneficial but require open-mindedness, communication, and coordination. OB-GYNs and other women’s health providers should educate their patients about retail clinics, especially during off-clinic hours to perhaps avoid urgent care or emergency department visits, while emphasizing that their clinic can still be the patient’s medical home. 7 Providers at retail clinics can also inform patients that nearby women’s health clinics offer more comprehensive services and continuity of care. Communication between clinics can create a community-based health team, which benefits women of all ages.
Conclusions
In this study of a large national retail health clinic network, adult women were found to be more frequent users of care than men. Retail health clinics provide an alternative for women seeking predominantly acute care that may offer convenience or complement a women’s health outpatient practice. Most conditions were for acute non-gynecologic care, yet visits for vaccinations, contraception, lower abdominal discomfort, or urinary vaginal infections can be managed in either a retail or women’s health clinic. It is important to acknowledge that some women seen at retail clinics do not have primary care physicians or OB-GYNs from which they can obtain an immediate appointment. The model is being considered for extension to more rural areas where workforce limitations are more common.
As retail health services continue to grow, efforts to ensure that care is coordinated with women’s health service providers will be essential. Coordination would be more likely if the traditional office practice is overwhelmed with patient needs. Having a retail clinic nearby may help to unload some of the patient volumes, allowing specialists to focus on the more complicated diagnostic or treatment cases. We are unaware whether these retail clinics will have difficulty in coordinating care with traditional clinic settings, as they may be seen by OB-GYN offices as competitors for their patients. The value of this research project was to “open the door” for more discussion such as surveying nearby OB-GYN offices as to whether retail clinics are viewed as supportive or unsupportive of their current or future patients.
Examples of Conditions Seen in each Category of the Primary Reason for Clinic Visits by Women
Footnotes
Authors’ Contributions
W.F.R., J.A., D.F.: Conceptualization, Design, Acquisition and interpretation of data, and Writing—Original draft preparation and Review and editing.
Author Disclosure Statement
No competing financial interest exists. W.R. did not report any potential conflicts of interest and received no funding. J.A. and D.F. are employees of CVS Health Corporation and own stock but have no conflicts germane to this study.
Funding Information
Funding was provided by CVS Health only for the costs associated with an independent institutional board review and approval by the WCG Institutional Review Board.