
Abstract
Description:
New York State Department of Health (NYSDOH) recommends that all pregnant patients receive human immunodeficiency virus (HIV) screening during pregnancy. This study assessed the prevalence of repeat prenatal HIV testing and factors associated with receipt of the recommended tests.
Methods:
Data from the NYSDOH newborn screening program were used to randomly select pregnant persons without HIV who delivered a liveborn infant in 2017. Receipt of repeat testing was defined as an initial HIV test in the first or second trimesters and the final in the third trimester (relaxed); or an initial test in the first trimester and the final in the third trimester (strict). Relative risks (RRs) and 95% confidence intervals were calculated in bivariate analyses. Adjusted RRs were calculated to determine associations between demographic and clinical factors and receipt of repeat HIV testing.
Results:
The cohort included 2,225 individuals. Roughly one quarter (24%) received the recommended tests in the first or second and third trimesters and 17% received them in the first and third trimesters. Individuals who reported Hispanic or Asian race/ethnicities, had government-funded insurance, started prenatal care in the first trimester, delivered in New York City, or received prenatal hepatitis C virus screening were significantly more likely to receive repeat testing using either definition.
Conclusions:
Despite the benefits and cost-effectiveness, the prevalence of repeat prenatal HIV screening during the third trimester remains persistently low. Improved messaging and targeted education and resources to assist prenatal providers could reinforce the importance of repeat testing and reduce residual perinatal HIV transmission.
Introduction
Since 2006, the Centers for Disease Control and Prevention has recommended that pregnant persons living in jurisdictions with elevated rates of HIV diagnoses receive repeat human immunodeficiency virus (HIV) screening in the third trimester to prevent perinatal HIV transmission associated with acute HIV infection acquired late in pregnancy. 1 Consistent with these guidelines, the New York State Department of Health (NYSDOH) recommends that all pregnant patients receive universal opt-out HIV screening early in pregnancy with repeat testing in the third trimester, preferably before 36 weeks gestation, for those with initial HIV antibody negative tests. 2 Despite these recommendations, 3,4 residual perinatal HIV transmissions persist within New York State (NYS), with 16 transmissions occurring in the past decade. 5
The NYSDOH monitors prenatal and expedited HIV testing for birthing parents and their infants at approximately 120 birth facilities in NYS using facility-reported data. Data are reported back to the facilities via biannual performance letters as part of regulatory oversight and continuous quality improvement. These data show that while the percentage of all pregnant people in NYS aware of their HIV status before delivery has remained high (≥95%) since 2004, the percentage with repeat testing during the third trimester has been persistently low (16% on average) since monitoring began in 2013. Inadequate prenatal screening may delay HIV diagnosis leading to high maternal viral load and increased risk of perinatal HIV transmission. 6 –11
This analysis aimed to: (1) evaluate if the low prevalence of third trimester HIV testing reported by NYS regulated birth facilities accurately reflects the prevalence of repeat prenatal HIV testing, (2) identify factors associated with receipt of the recommended test, (3) establish a baseline for future program evaluation, and (4) provide findings to inform the development and implementation of tailored interventions to address any identified inequities in prenatal rescreening.
Materials and Methods
Data sources and study population
This study used a retrospective cohort constructed using data from the NYSDOH newborn screening program, a program that screens all infants born in NYS for genetic disorders and in utero HIV exposure. 12 A random sample of people who delivered a liveborn infant at one of 127 NYS regulated birth facilities and were not diagnosed with HIV at the time of delivery was selected for medical record review from 223,038 eligible records available in NYSDOH newborn screening program data in 2017. The sampling process was designed to select patient records based on the NYS geographic region and size of the birth facility, in proportion to the number of births at facilities within each region. There were seven birth facility regions: Buffalo, Capital, Central, Central Islip, New Rochelle, New York City, and Rochester. Birth facilities with <1,200 births annually were classified as “low volume,” facilities with 1,200 or more but <3,000 births were classified as “medium volume,” and facilities with 3,000 or more births were classified as “high volume”. This ensured all birth facilities, regardless of their birth volume, were represented in the sampling process. Three parameters were used to determine the minimum sample sizes required per region: (1) the expected proportion of repeat prenatal HIV testing in NYS (a conservative estimate of 0.5 was used); (2) the desired margin of error (0.05 was used); and (3) confidence level (at 95%). The probability that medical records selected would have useable information was also factored in (at 95%). HIV testing during pregnancy and other study variables were obtained through medical record abstraction conducted by the Island Peer Review Organization using standardized data collection tools. Extracted records were deidentified before the data analysis.
Pregnant people were excluded from the analysis if they had no known HIV testing history or lacked information on the timing of their HIV testing in relation to trimester, gave birth before 37 weeks of gestation, had no record of prenatal care, or resided outside of NYS at the time of delivery. The NYSDOH Institutional Review Board determined that this activity was non-research and consistent with program evaluation and quality improvement authorized through NYS statutes and regulations.
Study outcome
Receipt of repeat prenatal HIV screening was defined as either: (1) an initial HIV test in the first or second trimester with repeat testing in the third trimester (relaxed) or (2) an initial HIV test in the first trimester with repeat testing in the third trimester (strict).
Study covariates
Study covariates included sociodemographic, clinical, and social behavioral characteristics. Sociodemographic characteristics were maternal age at delivery, race/ethnicity, marital status, insurance payor type, birth facility region, and birth facility volume. Clinical characteristics were trimester of prenatal care initiation, documentation of mental health disorder in the medical record, history of sexually transmitted infection (STI) diagnosis before the reviewed pregnancy, and STI and hepatitis C virus (HCV) testing during the reviewed pregnancy. Social behavioral characteristics were substance use before pregnancy, substance use during pregnancy, and tobacco use during pregnancy. Substance use included illicit substances and alcohol.
Statistical analysis
Relative risks (RRs) and 95% confidence intervals were calculated in bivariate and multivariable analyses to examine the association between study covariates and the relaxed and strict definitions of receiving the recommended prenatal HIV testing. Significant variables from the respective bivariate analyses were included in separate multivariable models. Backwards elimination was used to determine which covariates remained in the final models; covariates significant at p < 0.05 were retained. Adjusted relative risks (aRRs) were calculated using Poisson regression analyses with robust variance estimates. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Study population characteristics
A total of 4,001 individuals from the NYSDOH Newborn Screening Program data were selected for medical record review. A total of 2,225 were retained for analyses after excluding 1,776 individuals who resided outside of NYS at the time of delivery (n = 923), gave birth before 37 weeks of gestation (n = 381), lacked information on the timing of their HIV tests in relation to trimester (n = 336), had no record of HIV testing (n = 127), or had no record of prenatal care (n = 9). (Fig. 1)
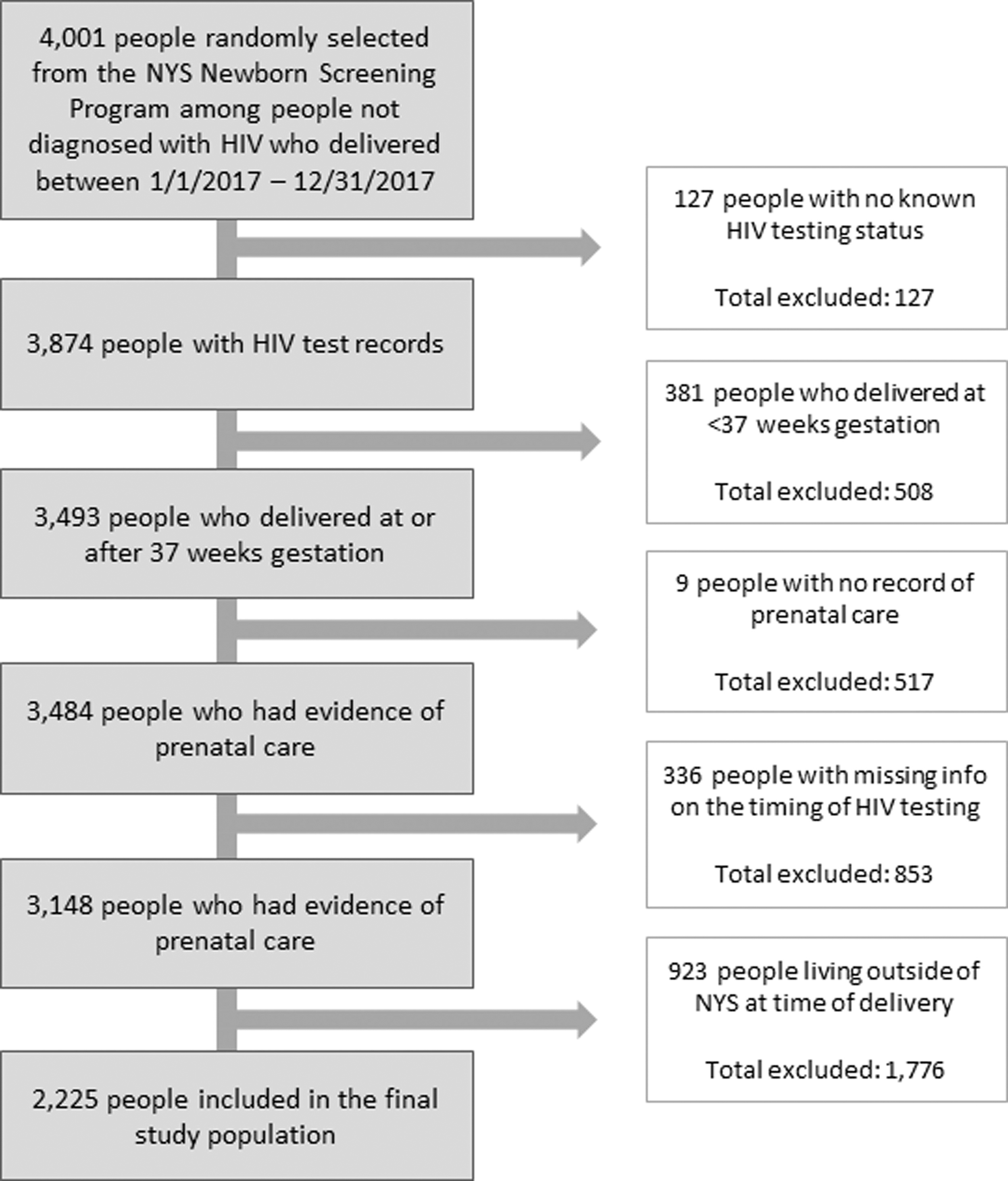
Flow chart of inclusion and exclusion criteria for HIV negative pregnant people who delivered a liveborn infants in NYS in 2017.
Most patients in the study population were non-Hispanic White (57%), age 20–29 years at the time of delivery (49%), married (55%), or started prenatal care in the first trimester (53%) (Table 1). Privately-funded policies were the predominant source of health insurance (58%). A small proportion of participants had documented substance use during the reviewed pregnancy (8%), a documented mental health disorder (15%), or a history of STI diagnosis (5%). Most participants (99%) received a test for STIs, but only 23% received a test for HCV; 99.7% had at least one documented HIV test.
Study Population Characteristics and Regression Results for the Relaxed Outcome Definition a
≥1 HIV test in the first or second trimester and ≥1 HIV test in the third trimester.
During reviewed pregnancy.
CI, confidence interval; NYS, New York State; RR, relative risk; STI, sexually transmitted infection.
Repeat HIV testing (relaxed definition)
Roughly one in four (24%) participants received an HIV test in the first or second trimester followed by a repeat test in the third trimester. In bivariate analyses, maternal age at delivery, race/ethnicity, marital status, trimester of prenatal care initiation, insurance payor type, receipt of HCV testing, birth facility region, and birth facility volume were all significantly associated with receipt of repeat HIV testing during pregnancy (Table 1). In multivariate analyses, all except for marital status and birth facility volume remained significant. Individuals of age <20 years (aRR: 1.38, 95% CI: 1.04–1.8) were significantly more likely to receive the recommended testing compared with those of age 20–29 years. While attenuated, the association between receipt of the recommended testing and race/ethnicity remained strong for individuals who identified as non-Hispanic Black (aRR: 1.34, 95% CI: 1.1–1.6), Hispanic (aRR: 1.64, 95% CI: 1.3–2.1), and non-Hispanic Asian (aRR: 1.78, 95% CI: 1.4–2.2) compared with those who identified as non-Hispanic White. Individuals tested for HCV (aRR: 1.38, 95% CI: 1.2–1.6) were more likely to receive the recommended HIV rescreening as were those who had government compared with privately-funded health insurance (aRR: 1.41, 95% CI: 1.2–1.7); pregnant persons who delivered in NYC compared with outside of NYC (aRR: 2.23, 95% CI: 1.9–2.6) were also more likely to be rescreened for HIV. Not surprisingly, initiation of prenatal care in the third versus the first trimester (aRR: 0.33, 95% CI: 0.2–0.5) remained associated with a significantly lower likelihood of repeat prenatal HIV testing after adjusting for covariates (Table 1) as there was limited opportunity or potential need to retest.
Repeat HIV testing (strict definition)
Seventeen percent of participants received an HIV test in the first and third trimesters. In bivariate analyses, race/ethnicity, trimester of prenatal care initiation, insurance payor type, receipt of HCV testing, birth facility region, and birth facility volume were significantly associated with receiving repeat HIV testing during pregnancy (Table 2). In multivariate analyses, all except birth facility volume remained significant in multivariable analyses. Compared with individuals who identified as non-Hispanic White, those who identified as Hispanic (aRR: 1.94, 95% CI: 1.5–2.6) or Asian (aRR: 1.82, 95% CI: 1.4–2.4) were almost twice as likely to be rescreened for HIV in the third trimester. Those who tested for HCV were more likely to receive repeat HIV testing (aRR: 1.41, 95% CI: 1.2–1.7), as were those who had government funded compared with privately-funded insurance (aRR: 1.27, 95% CI: 1.04–1.6). Compared with those who initiated prenatal care during the first trimester, those who initiated prenatal care during the second (aRR: 0.36, 95% CI: 0.3–0.5) or third (aRR: 0.28, 95% CI: 0.2–0.5) trimester were less likely to have received repeat testing. Individuals who delivered at a facility in NYC were more likely to receive repeat testing than those who delivered outside of NYC (aRR: 2.21, 95% CI: 1.8–2.8).
Study Population Characteristics and Regression Results for the Strict Outcome Definition a
≥1 HIV test in the first trimester and ≥1 HIV test in the third trimester.
During reviewed pregnancy.
CI, confidence interval; NYS, New York State; RR, relative risk; STI, sexually transmitted infection.
Discussion
Most pregnant people (99.7%) in this study had at least one HIV test during pregnancy but few received the recommended repeat HIV screening as defined by the relaxed or strict definitions, at 24% and 17%, respectively. The 17% is comparable to previous observations from NYSDOH monitoring of regulated self-reported birth facility data. Our findings were lower than those presented in other studies using United States data, which indicate that late gestation HIV rescreening remains highly variable, 8,13,14 ranging from 28% to 90%. 8,14
Regardless of the definition used, strict or relaxed, those who identified as non-Hispanic White, who did not receive an HCV test, or who delivered outside of NYC had a significantly lower likelihood of receiving the recommended repeat prenatal test after adjustment for other covariates. Age >20 years (relaxed definition) and privately-funded health insurance were also associated with a decreased likelihood of receiving the recommended screening. These findings are consistent with prior studies that also observed a lower prevalence of rescreening among pregnant people who were non-Hispanic White, privately insured, and older, 8,13,15 suggesting that maternal characteristics and regional differences may reflect provider bias regarding pregnant patients’ HIV exposure risk.
Our data showed that a small proportion of pregnant people initiated prenatal care in the third trimester. Timely initiation of prenatal care is vital to avert adverse maternal and fetal/child outcomes, as persons who begin prenatal care late in pregnancy are less likely to receive adequate prenatal care, which includes comprehensive HIV screening. 16,17 Late entry and underutilization of prenatal care are associated with higher maternal morbidity and mortality, including late or missed maternal HIV diagnosis and perinatal HIV transmission. These negative outcomes are highest among non-Hispanic Black persons giving birth. 5,18,19 In the current study, 40% of pregnant persons identifying as non-Hispanic Black initiated prenatal care in the first trimester compared with 44% Hispanic, 46% non-Hispanic Asian, and 60% non-Hispanic White. While they were least likely to receive early prenatal care, non-Hispanic Black pregnant people were significantly more likely to be rescreened for HIV with the relaxed definition, but not the strict definition. Importantly, disparate rescreening across all communities of color was not observed. Pregnant people who identified as Hispanic and non-Hispanic Asian were more likely to be rescreened using either the relaxed or strict definitions. Together these data indicate that interventions aimed at improving timely, accessible, and quality prenatal care, particularly for Black women, are necessary. Interventions should include equitable access to HIV testing, treatment, and prevention and focus on structural determinants and the social context given their significant impact on timing and consistency of prenatal services. 16,20,21
Federal and state statutes and regulations that govern the care of pregnant people and their infants, including mandates for the provision of HIV testing, are more likely to be followed than recommendations. 22,23 In NYS, prenatal testing and the proportion of individuals receiving an expedited test markedly increased following the passage of expedited HIV testing regulations in 1999 and 2003. 22 A similar result for recommended repeat HIV testing in the third trimester has not been realized despite evidence that timely prenatal HIV diagnosis, prompt initiation of and adherence to antiretroviral treatment, and appropriate intrapartum and newborn management reduce the risk of perinatal HIV infection. 6 –11,24
In addition to the short- and long-term health benefits afforded to birthing parents and infants with early maternal HIV diagnosis, several studies have indicated that prenatal rescreening is cost-effective. 25 –28 Bert et al. (2018) found that both universal prenatal HIV screening and repeat third trimester screening were cost-effective in both high- and low-resource countries in areas of both high and low HIV prevalence. Specifically in NYS, Laufer et al. (2016) found that expenditures for HIV treatment protocols (e.g., zidovudine prophylaxis) and interventions to prevent perinatal HIV transmission, including late gestation rescreening, were low-cost and generated substantial dollar savings in averted medical costs for infants perinatally exposed to HIV.
Strengths/Limitations
NYS has collected statewide birth facility and maternal–infant HIV-related testing information using standardized tools for more than 2 decades. Robust systems and infrastructure within the state are well established and ensure coordinated efforts and quality assurance between regulated birth facilities and the NYSDOH Newborn Screening Program, HIV/AIDS Surveillance Program, and the Maternal-Pediatric HIV Prevention and Care Program. Previous program evaluation has affirmed the validity and reliability of NYS’ population-wide maternal–infant HIV testing program. 22 Demographic characteristics in the study population reflected the overall population giving birth to liveborn infants in NYS in 2017 (57% vs. 48% non-Hispanic White; 49% vs. 42% of age 20–29 years at delivery; 55% vs. 61% married). 29 The medical record review and self-reported birth facility data for initial prenatal HIV testing for 2017 overall were very similar at 99% and 97%, respectively.
However, the NYS average for repeat HIV testing as reported by birth facilities was slightly lower (16%) than what was found through medical record review (17% and 24% strict and relaxed definition, respectively). This analysis did not capture all prenatal care settings (e.g., community-based health center, private practice, academic hospital-based clinic), which limits our understanding of clinical setting in relation to prevalence of repeat testing and how setting may impact intervention strategies and future evaluation. Some prenatal care occurred in settings other than birth facilities, which could have contributed to underreporting of third trimester testing. Moreover, NYS population, health care settings, clinical services, and geography are highly diverse. There are large, dense urban areas as well as extremely rural regions, some of which do not have a birth facility within their counties. The lower proportion of pregnant persons outside of NYC with a documented third trimester test may reflect overall challenges associated with care provision to the less concentrated population. We could also not account for regional differences in factors such as provider education or electronic medical record systems that can impact the completeness of reporting. Our study sample was designed to address this diversity by inclusion of subjects from different regions and birth facilities with various birth volumes.
Conclusions
In NYS, universal opt-out repeat HIV testing during the third trimester remains a critical and cost-effective, yet underutilized, strategy for detecting the acquisition of acute HIV late in pregnancy. These findings, in conjunction with community and provider input, will inform individual, community, and systems-focused interventions to further reduce perinatal HIV transmission in NYS. Intervention strategies will aim to better educate providers and pregnant people regarding the benefits of testing, create effective social messaging campaigns, improve the accuracy of provider-reported testing history, and provide support to NYS clinicians to operationalize late gestation HIV rescreening. Moreover, findings will serve as a basis for developing system-focused interventions to address structural factors that impede equitable access to and utilization of timely, high-quality prenatal care, particularly for non-Hispanic Black women. HIV testing in pregnancy is a vital component of comprehensive prenatal care. By reducing HIV testing disparities, we can help to prevent perinatal HIV transmission and improve maternal morbidity and mortality in NYS.
Footnotes
Acknowledgments
The authors would like to acknowledge Dhanushki Samaranayake, PhD and Wilson P. Miranda, MPH for developing the sampling strategy to obtain the study population; Michelle Cummings, MS for assistance with the initial cleaning and analysis of the chart review data; Barbara L. Warren, BSN, MPH, PNP for conceptualization; and Beth S. Weir, BS, BA, RN for assistance with reviewing and editing the article.
Author’s Contributions
M.R.: Methodology, formal analysis, writing—original draft, writing—review and editing. A.S.: Writing—original draft, writing—review and editing, data curation. L.H.: Conceptualization, Writing—review and editing. J.L.: Conceptualization, supervision, methodology, writing—review and editing. C.W.: Data curation. T.O.: Writing—review and editing. C.-A.S.: Methodology, formal analysis, conceptualization, supervision, writing—original draft, writing—review and editing. S.K.: Project administration, conceptualization, writing—original draft, writing—review and editing.
Authors Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.