
Abstract
Background:
Previous studies have found that unintended pregnancy rates are higher among racial minorities and active duty servicewomen (ADSW), correlating with lower rates of effective contraceptive use. The Military Health System (MHS) provides universal health care benefit coverage for all ADSW, including access to all highly effective contraceptive (HEC) methods. This study investigated the association between race and HEC use among ADSW.
Materials and Methods:
We conducted a cross-sectional study using fiscal year 2016–2019 data from the MHS Data Repository for all ADSW ages 18–45 years. Statistical analyses included descriptive statistics and logistic regression models, adjusted and unadjusted, determining the odds of HEC use, overall and by method.
Results:
Of the 729,722 ADSW included in the study, 59.7% used at least one HEC during the study period. The highest proportions of users were aged 20–24 years, White, single, Junior Enlisted, and serving in the Army. Lower odds of HEC use were demonstrated in Black (odds ratio [OR] = 0.94, 95% confidence interval [CI] = 0.92–0.95), American Indian/Alaska Native (OR = 0.85, 95% CI = 0.82–0.89), Asian/Pacific Islander (OR = 0.81, 95% CI = 0.80–0.83), and Other (OR = 0.97, 95% CI = 0.94–0.99) ADSW compared with White ADSW.
Conclusions:
Universal coverage of this optional preventive service did not guarantee its use. The MHS can serve as a model for monitoring racial disparities in HEC use.
Introduction
A highly effective contraceptive (HEC) is any reversible contraceptive with a failure rate of less than 10%. 1 HECs include hormonal pills (progestin-only and combination), patches, vaginal rings, shots/injections, subdermal implants, and both hormonal and nonhormonal intrauterine contraceptive devices (IUDs). 1,2 The Military Health System (MHS), which provides universal health care benefit coverage for all active duty service members (ADSMs), offers access to all common forms of short-acting and long-acting prescription contraception at no cost. Permanent sterilization is also available to male and female ADSMs.
Healthy People 2030 (HP2030) identifies family planning, to include contraceptive management, as a significant health behavior warranting targeted public health efforts. 3 Effective family planning enables reproductive autonomy, allowing individuals and families to live with confidence in their reproductive health choices. Ineffective family planning results in negative reproductive health outcomes, such as unintended pregnancy. 3,4 Nearly half of pregnancies occurring in the United States are unintended, meaning they are either mistimed (pregnancy desired but not at the time of conception) or unwanted (did not want to conceive at all). 3,5,6 Unintended pregnancy poses a significant risk to individual and military unit readiness. 4,5,7,8 Active duty servicewomen (ADSW) are reported to have a higher rate of unintended pregnancy than the general U.S. population. 5,9 Within the general U.S. population, unintended pregnancy rates are higher among young women and racial minorities. Higher rates of unintended pregnancy appear to correlate with lower rates of effective contraceptive use. 5,9,10
Health disparities persist within the U.S. health care system, including the provision of women’s reproductive health and family planning services. 10 The MHS has been identified as a potential model for investigating health disparity mitigation efforts aiming to increase access to and utilization of family planning services. 7,11 Previous studies have demonstrated successful mitigation of racial disparities for ADSW within the MHS for other preventive services, such as cervical cancer screening and mammography. 11,12 Although there have been recent studies investigating contraceptive use among ADSW, a review of the current literature failed to identify studies specifically investigating the association between race and effective contraceptive use. 1,5,8,9,13 –17 This study investigated the association between race and HEC use among ADSW to determine whether racial disparities observed within the general U.S. population regarding effective contraceptive use persist within the MHS.
Materials and Methods
We performed a cross-sectional study utilizing fiscal year (FY) 2016–2019 health care encounter, prescription, claims, and Defense Enrollment Eligibility Reporting System (DEERS) data from the MHS Data Repository (MDR). The study population included all females, ages 18–45 years, serving on active duty status in the U.S. Army, Navy, Air Force, and Marine Corps. Service members were excluded if they served in the U.S Coast Guard or were listed as active/inactive National Guard or Reserve status. These individuals do not rely upon the MHS for the entirety of their health care coverage, as is the case for ADSMs, so their data in the MDR are often incomplete/missing. Service members were also excluded if they were over the age of 45, consistent with the larger body of contraceptive literature.
The primary outcome of interest was HEC use, recorded as use or nonuse. The secondary outcome of interest was HEC use categorized by HEC method. For the purpose of this study, any contraceptive method with a failure rate of less than 10% (less than 10 in 100 women became pregnant within their first year of typical use during effectiveness trials) was considered an HEC method (Table 1). 2 Individuals were identified as having used an HEC if their record demonstrated a filled prescription, an International Classification of Diseases diagnostic code, or a Current Procedural Terminology/Supply code for an HEC during the study period (Table 2). 18 HEC methods were categorized into short-acting reversible contraceptives (SARCs), long-acting reversible contraceptives (LARCs), and female sterilization. SARCs included pills, patches, vaginal rings, and shots/injections. LARCs included subdermal implants and IUDs. Individuals noted to have used more than one HEC method during the study period were categorized as “Multiple HEC Use.”
Contraceptive Method Effectiveness a
Data source. 2
Denotes a highly effective contraceptive (HEC) method.
Contraceptive Management Codes a
Data source. 18
CPT, Current Procedural Terminology; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification.
Brand and generic formulary.
The primary exposure variable of interest was race, categorized in the MDR as White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other, or Missing. Ethnicity is highly missing in MDR data and was not included in analyses. Other exposure variables of interest included age (by group, reported in years), marital status (single applied to individuals who were single/never married, divorced, and/or widowed), rank (by group, used as a proxy for socioeconomic status [SES]), and branch of service.
Descriptive statistics were performed on the demographic data obtained from DEERS and reported as frequencies and percentages. For any time-sensitive variables, such as age, the most recent demographic data from DEERS were used if an individual appeared multiple times during the study period. Binomial logistic regression models, both unadjusted and adjusted, were performed for HEC use, overall and by method, and reported as odds ratio (OR) with 95% confidence interval (CI). Individuals’ missing data for race were excluded from these models. All covariates of interest (age-group, race, marital status, rank, and branch of service) were included in the adjusted models. Statistical significance (α) was set a priori at 0.05. All analyses were performed using SAS 9.4. This work was considered exempt by the Institutional Review Board of the Uniformed Services University of the Health Sciences.
Results
Of the 729,722 ADSW identified for inclusion in the study, 59.7% (n = 435,370) used at least one HEC during the study period (Fig. 1). Considering those individuals identified as HEC users, the largest proportions were individuals who were White, 20–24 years old, single, Junior Enlisted, and serving in the U.S. Army (Table 3). These served as the reference groups for the logistic regression models. There were 21,544 individuals (2.95% of total study population) identified as missing data for race and excluded from the regression analyses. Among the 435,370 ADSW identified as HEC users, 36.7% used an SARC, 33.2% used an LARC, 28.2% used multiple HEC methods, and 2.0% used female sterilization (Table 4). White ADSW constituted the largest proportion of users for each of the HEC method categories considered. Of note, the largest proportions of ADSW identified as using female sterilization were individuals who were White, 30–34 years old, married, Senior Enlisted, and serving in the U.S. Army.
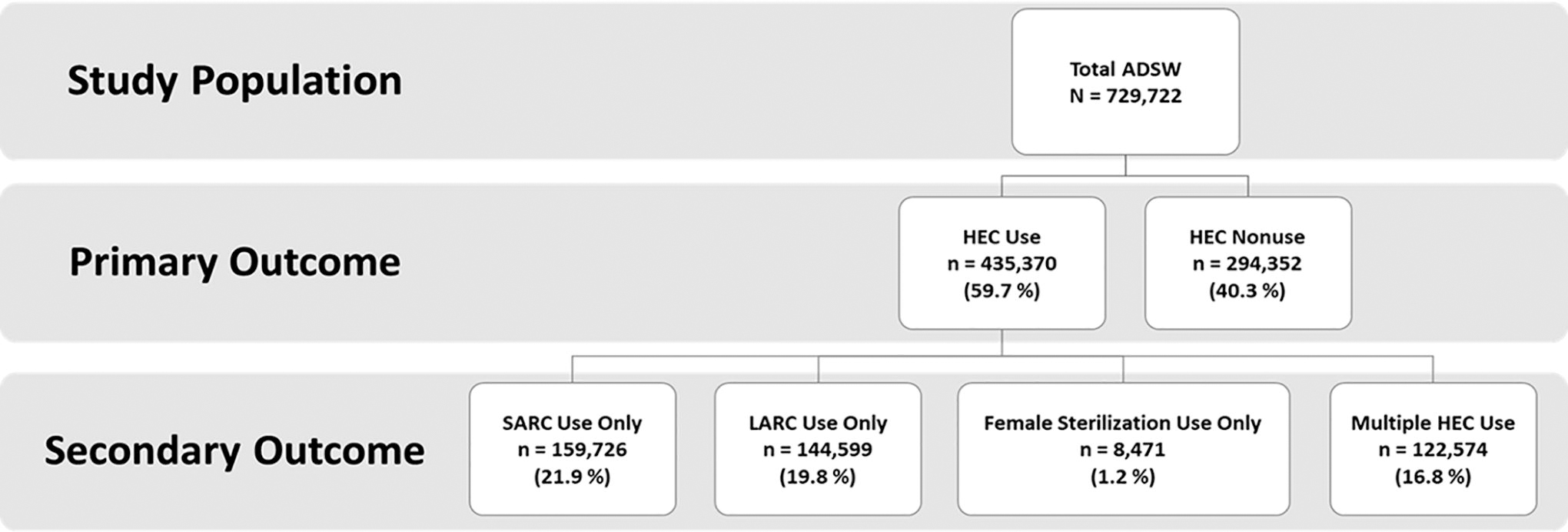
Flowchart of highly effective contraceptive use among U.S. active duty servicewomen, fiscal years 2016–2019. N denotes the number of women in the study population, and n denotes the number of women in each subgroup. Percentages listed are of the total study population. ADSW, active duty servicewomen; HEC, highly effective contraceptive; LARC, long-acting reversible contraceptive; SARC, short-acting reversible contraceptive.
Descriptive Statistics of U.S. Active Duty Servicewomen, Fiscal Years 2016–2019
ADSW, active duty servicewomen; HEC, highly effective contraceptive.
Values reported as frequencies and percentages = n (%).
Age reported in years.
Definitions: Junior Enlisted—E1–E4, Senior Enlisted—E5–E9, Junior Officers—O1–O4, Senior Officers—O5–O10.
Descriptive Statistics of HEC Use Among U.S. Active Duty Servicewomen, Fiscal Years 2016–2019 a
HEC, highly effective contraceptive; LARC, long-acting reversible contraceptive; SARC, short-acting reversible contraceptive.
Values reported as frequencies and percentages = n (%).
Age reported in years.
Definitions: Junior Enlisted—E1–E4, Senior Enlisted—E5–E9, Junior Officers—O1–O4, Senior Officers—O5–O10.
Lower odds of HEC use were demonstrated in all ADSW racial subgroups, when compared with White ADSW, in both the adjusted and the unadjusted models. The following adjusted ORs were demonstrated, when compared with White ADSW, for Black (OR = 0.94, 95% CI = 0.92–0.95), American Indian/Alaska Native (OR = 0.85, 95% CI = 0.82–0.89), Asian/Pacific Islander (OR = 0.81, 95% CI = 0.80–0.83), and Other (OR = 0.97, 95% CI = 0.94–0.99) ADSW. The adjusted model demonstrated that the odds of HEC use decreased with increasing age, was lower for single as compared with married ADSW, was lowest among Junior Enlisted ADSW as compared with any other rank group, and was lowest among ADSW in the U.S. Marine Corps as compared with any of the other branches of service (OR = 0.91, 95% CI = 0.89–0.93) (Fig. 2).
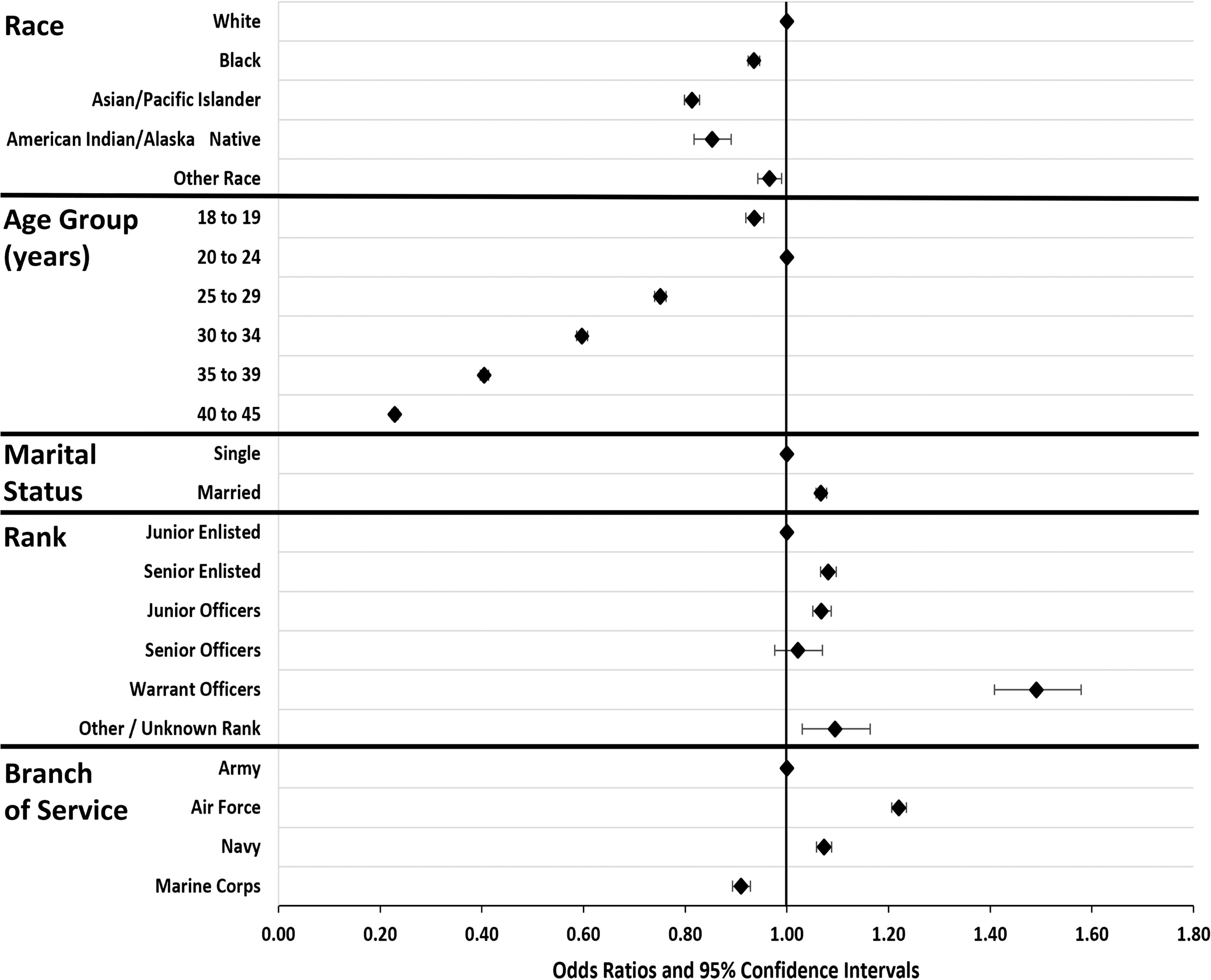
Forest plot of adjusted odds ratios for highly effective contraceptive use among U.S. active duty servicewomen, fiscal years 2016–2019. Model reference groups are plotted on the 1.00 odds ratio value line. Diamonds indicate the odds ratio value with the bracketed lines indicating the associated 95% confidence interval. Definitions: Junior Enlisted—E1–E4, Senior Enlisted—E5–E9, Junior Officers—O1–O4, Senior Officers—O5–O10.
Adjusted regression models were performed for each HEC method category (Table 5). The odds of HEC use by method for non-White ADSW, as compared with White ADSW, varied depending upon the HEC method category considered. For LARC use only, all non-White ADSW had lower odds of use as compared with White ADSW, with Black ADSW demonstrating the lowest odds of use (OR = 0.81, 95% CI = 0.80–0.83). The adjusted model demonstrated that the odds of LARC use only increased with increasing age, was lower for single as compared with married ADSW, was lowest among Junior Enlisted ADSW as compared with any other rank group, and was highest among ADSW in the U.S. Marine Corps as compared with any of the other branches of service (OR = 1.73, 95% CI = 1.69–1.78).
CI, confidence interval; HEC, highly effective contraceptive; LARC, long-acting reversible contraceptive; OR, odds ratio; SARC, short-acting reversible contraceptive.
Regression model adjusted for age-group, race, marital status, rank, and service.
Age reported in years.
Definitions: Junior Enlisted—E1–E4, Senior Enlisted—E5–E9, Junior Officers—O1–O4, Senior Officers—O5–O10.
*denotes cell count was too small to compute, but the model converged.
Discussion
As of 2019, the U.S. military was composed of 1,326,200 ADSMs, with 16.9% identifying as female. 19 The proportion of ADSMs who are women of childbearing age continues to rise and with it the population at risk for unintended pregnancy within the MHS. 7,20 One of the family planning objectives established by HP2030 is to “increase the proportion of women at risk for unintended pregnancy who use effective birth control.” The target goal for this objective is for 65.1% of women aged 20–44 years and at risk of unintended pregnancy to use moderately or most effective methods of contraception. 3 The National Survey of Family Growth reported that, between 2015 and 2017, 60.3% of U.S. women aged 20–44 years who were considered at risk of unintended pregnancy used moderately or most effective methods of contraception. Our study found that, between 2016 and 2019, 59.7% of ADSW aged 18–45 years used highly effective methods of contraception. Despite the MHS providing universal coverage of all HEC methods and ADSW receiving health care in a no-cost system, the proportion of ADSW using effective birth control continues to fall below that of the general U.S. population and the HP2030 target goal. This would indicate that universal coverage alone is insufficient to achieve the goal of increasing effective contraceptive use among this at-risk population. 8
Rank is a surrogate for SES with Junior Enlisted being considered the lowest SES group. Recent studies have reported unintended pregnancy rates as high as 65% for ADSW, with the highest rates reported among young, single, Junior Enlisted ADSW. 4,5,9,14 These higher rates of unintended pregnancy tend to correlate with lower rates of effective contraceptive use. 4,9 Our study determined that the odds of HEC use were lowest for young, single, Junior Enlisted ADSW. A study investigating contraceptive use and pregnancy rates in newly accessioned Enlisted U.S. military members found that policy differences between the various services may play a role in contraceptive access and utilization, especially by the notably vulnerable population of young, Enlisted ADSW. 1,9 This would indicate that there continue to be barriers to effective contraceptive use for subgroups of ADSW, keeping these populations at greater risk of unintended pregnancy and poor reproductive health outcomes. 7 Identifying and implementing mitigation strategies for these vulnerable populations should be a priority for military public health efforts. 5
The first step in mitigating health care disparities is identifying that they exist. The MHS uses the same data repository for all branches of service, offering a comprehensive view of health care received across the entire active duty force. This enabled us to identify a sample size large enough to allow for racial subgroup analysis. Race data are self-reported in this system and are relatively complete for ADSMs. Racial minority ADSW (American Indian/Alaska Native, Asian/Pacific Islander, Black, and Other) comprised 40.0% of our total study population and 34.0% of our ADSW using HEC subpopulation. Both these proportions exceeded the 31.2% of ADSW who identified as racial minorities (American Indian/Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, Multiracial, and Other/Unknown) in 2019. 19 Native American and Asian/Pacific American racial subgroups are often excluded from research studies and national health surveys because of missing or insufficient data. 6 Our study demonstrated that the MHS provides sufficient representation of these groups to include them in future research focused on racial subgroup analyses.
A 2013 survey of women in the general U.S. population demonstrated racial disparities in contraceptive use with 58% of Black women versus 65% of White women reporting the use of a form of contraception. 6 Our study was the first to investigate the association between race and effective contraceptive use among ADSW. ADSW in all racial minority subgroups had lower odds of HEC use as compared with White ADSW, demonstrating that racial disparities in contraceptive use persist within the MHS with racial minority ADSW less likely to use effective contraceptives. 10,21
The MHS, owing to its universal health care benefit coverage for all ADSMs, had already been suggested as a potential model for investigating health disparity mitigation efforts aiming to increase access to and usage of family planning services. 7,11 Previous studies that demonstrated successful mitigation of racial disparities for preventive services (cervical cancer screening and mammography screening) within the MHS dealt with services that are considered mandatory for ADSW. 11,12 Contraception, in contrast, is and should remain an optional preventive service. Comprehensive education about and access to counseling for the full range of contraceptives have been identified as gaps in provision of the highest quality health care for women in the service. 4 Policies and procedures to ensure that all ADSW receive culturally and ethnically appropriate education regarding their contraceptive options would be a potential mitigation strategy to support the reproductive autonomy and medical readiness of ADSW.
Although this study had many strengths, there were also limitations that should be considered when interpreting the data. Although we were able to identify whether an individual used a specific HEC method during the study period, data pertaining to the duration of use, along with contraceptive adherence, discontinuation, and/or failure, were not reported. Neither was whether an individual identified as using multiple HEC methods was using them simultaneously or consecutively. Our dataset did not include qualitative data, such as an individual’s personal, cultural, or religious beliefs and/or intentions regarding contraceptive use, which limited our ability to identify reasons for nonuse. The MHS covers all forms of prescription contraceptives. Other forms of contraception (abstinence, natural family planning, barrier methods, and withdrawal method) are not covered by benefits within the MHS and are poorly tracked within the MDR. This study focused on those methods of contraception that are considered highly effective, which are all covered by the MHS.
Conclusions
Family planning in the form of contraceptive management is available at no cost for all ADSW within the MHS. Racial disparities in HEC use were observed among ADSW despite universal coverage of this optional preventive service. This study contributes to the growing body of literature demonstrating racial disparities in the reproductive health experiences of ADSMs. It highlights that continued efforts to identify barriers to family planning services access and utilization within the MHS are warranted and that the MHS can serve as a model for monitoring racial disparities in HEC use. To better understand the reproductive experiences of racial minority ADSW, future studies should incorporate data assessing beliefs, intentions, and behaviors related to contraception use and family planning. This would improve the ability of the MHS to develop appropriately tailored public health interventions to mitigating observed racial disparities, increasing reproductive autonomy for ADSW, and ultimately leading to a more effective and medically ready fighting force.
Footnotes
Authors’ Contributions
H.M.B., A.B., and T.P.K. contributed equally to all aspects of the research design, analysis, interpretation, and writing of the article. All authors are accountable for all aspects of the article.
Disclaimer
The views expressed in this article are the sole responsibility of the authors and do not necessarily reflect the views, assertions, opinions, or policies of the Uniformed Services University of the Health Sciences, the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the Department of Defense, or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. government.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
This study was funded by the Department of Defense, Defense Health Program, Grant #HU0001-20-20035.