
Abstract
Background:
There is evidence that women with gestational diabetes are at increased risk of the common mental disorders of anxiety and depression. The COVID-19 pandemic may have exerted an additional burden on the mental health of this population. The aim of this analysis was to compare levels of symptoms of common mental disorders and experiences during the COVID-19 pandemic between pregnant and postnatal women exposed and unexposed to gestational diabetes.
Methods:
Cross-sectional study utilizing quantitative data from an online survey administered across 10 countries to women who were pregnant or up to 6 months postpartum from 15 June to October 31, 2020. Women self-reported gestational diabetes and completed the Edinburgh Postnatal Depression Scale and GAD-7 (Generalized Anxiety Disorder 7 items) measures. The COPE-IS (Coronavirus Perinatal Experiences–Impact Survey) tool was also administered. Complete case analyses were conducted on a sample of 7,371 women.
Results:
There was evidence of an association between gestational diabetes and increased levels of depression symptoms, which was robust to adjustment for age, education, and employment status. There was only evidence of an association with anxiety in postnatal women. There was also evidence that women with gestational diabetes, particularly those in the postnatal period, experienced higher levels of pandemic-related distress, although they did not experience higher levels of COVID-19 infection in this sample.
Conclusions:
The increased risk of common mental disorders in women with gestational diabetes underscores the importance of integrated physical and mental health care for pregnant and postnatal women both during and beyond the pandemic. Clinical Trial Registration no. NCT04595123.
Introduction
The common mental disorders of anxiety and depression are the commonest morbidities of the perinatal period (during pregnancy and up to 1 year postpartum), affecting between 5% and 10% of women during this time. 1 Perinatal anxiety and depression are frequently co-morbid. 2 There is some evidence to support an association between perinatal common mental disorders and gestational diabetes mellitus (GDM), with evidence for an increased risk of antenatal and postnatal depression in women with GDM. 3 GDM is diabetes that occurs for the first time during pregnancy and has a global prevalence of between 5% and 10%. 4
A range of potential mechanisms may underpin this relationship between GDM and common mental disorders, including biological mechanisms such as inflammation and the psychosocial stressors associated with receiving a diagnosis of diabetes during pregnancy. Both GDM and perinatal common mental disorders are associated with a range of potential adverse outcomes for women and children, including an increased risk of obstetric and neonatal complications. 1,4
Since the advent of the COVID-19 pandemic, women in the perinatal period have been experiencing a range of stressors impacting their mental health and wellbeing. These include reduced contact with friends, family, and health and social care services during a time when women may need it most, alongside the anxiety of becoming infected with COVID-19 and transmitting the virus to their baby. 5,6 Indeed there is now a growing body of evidence that symptoms of anxiety and depression have increased in the perinatal population compared to prepandemic levels. 7 –11
Given that women with GDM may be at an increased risk of perinatal anxiety and depression, we hypothesized that they may also be at an increased risk during the pandemic; the pandemic may exert an additional adverse impact on mental health in women with GDM, particularly as they may be more vulnerable to some of the aforementioned risk factors. For example, there have been concerns about an increased risk of COVID-19 infection and more severe disease in those with diabetes; there is now some evidence that GDM is associated with an increased risk of COVID-19 infection and more severe disease. 12,13
Women with GDM may also be even more in need of contact with health services to support their physical and mental health during pregnancy. Yet there has been limited exploration of the mental health and wellbeing of women with GDM during the pandemic. Thus, the aim of this analysis was to compare both levels of symptoms of common mental disorders and exposure to COVID-19 during the pandemic among perinatal women with versus without GDM.
Methods
Sample
This analysis utilized quantitative survey data collected in adult pregnant and postnatal (up to 6 months following delivery) women from 15 June to 31 October, 2020, during baseline data collection for the observational international study “Impact of the COVID-19 Pandemic on Perinatal Mental Health (Riseup-PPD-COVID-19)”. Women were recruited through social media advertising (e.g., Instagram), networks of organizations, policymakers, local organizations, and other stakeholders. Participants who voluntarily provided informed consent completed the online questionnaire by using the project website link (
Details of how the sample was derived are displayed in Figure 1. From an original 15,611 respondents, 13,553 met eligibility criteria and provided informed consent. A further 2,965 respondents were excluded due to high levels of incomplete data (classified as not completing beyond question 2 of the survey), incongruent data (e.g., date of birth indicates a child older than 6 months), or duplicate respondents. This gave an eligible sample of 10,588. For the purposes of this analysis, two countries with a very small sample (Albania and Bulgaria) were excluded, as this meant that they provided negligible numbers of women with GDM. After excluding participants with missing data on the analysis variables, this gave a final sample of 7,371 women.
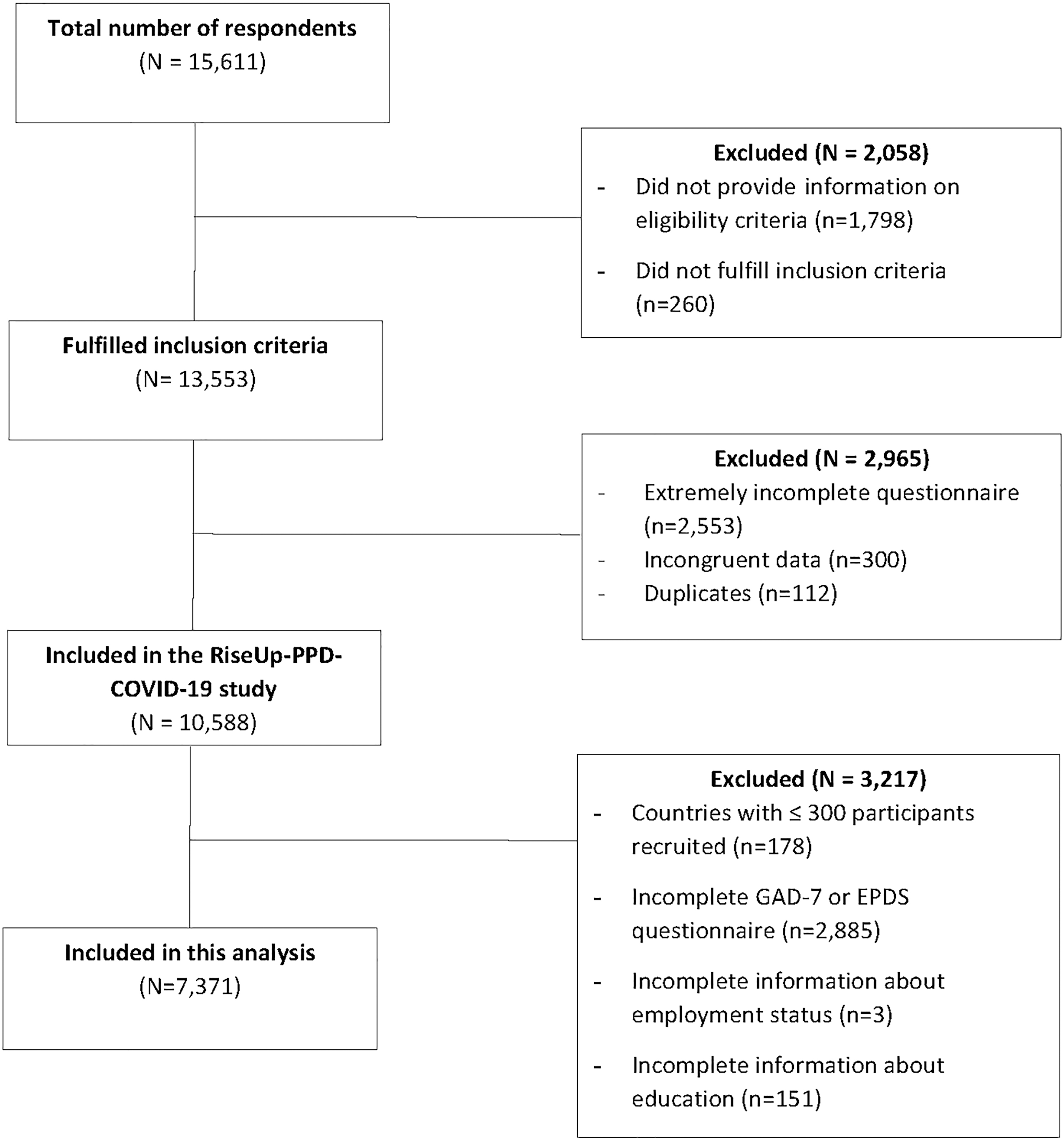
Flow diagram of participants in the study.
Measures
Sociodemographic variables
These included age of the woman, marital and employment statuses, and education level. Women were also asked if they are experiencing or had experienced GDM during pregnancy.
COVID-19-related variables
Experiences of women during the pandemic were assessed using the Coronavirus Perinatal Experiences–Impact Survey (COPE-IS). 15 In this study, the variables included were as follows: (1) diagnosis of and/or any symptoms compatible with COVID-19 (yes/no) and (2) COVID-19 concerns and distress (five items): (i) relating to one's own health, (ii) child's health, (iii) impact on employment and finances, (iv) impact on daily life, and (v) overall level of distress. Each of these items was Likert scale rated from 1 (no distress) to 7 (highly distressed). Psychometric properties of COPE-IS are not yet available. 15 Researchers from each country involved in the study performed the translation and cultural adaptation of questionnaires from English into the official language of their country.
Symptoms of depression
The Edinburgh Postnatal Depression Scale (EPDS) was used to enquire about common symptoms of depression. 16 The EPDS is a 10-item self-report scale used during the perinatal period. Each item is scored on a 4-point scale (from 0 to 3), giving a total score out of 30, with higher scores indicating higher levels of depression symptoms. Recent research suggests that an EPDS cutoff value of 11 maximizes both sensitivity and specificity for “caseness” (not necessarily a disorder), with a cutoff of 13 being less sensitive, but more specific. 17 Thus, 11 was used as a threshold, but 13 was also used to identify higher symptom levels.
The reliability for this scale was good. Cronbach's α was 0.882 for the entire sample and 0.882 and 0.881 for pregnant and postnatal women, respectively. The reliability by country and the range from minimum to maximum in EPDS scores are shown in the Supplementary Tables S1A and S2A.
Symptoms of anxiety
The Generalized Anxiety Disorder 7-item (GAD-7) measure of Generalized Anxiety Disorder symptoms was used in the survey to enquire about anxiety. 18 It has shown good reliability and construct validity in pregnancy and the postnatal period. 19,20 It is a self-report scale consisting of 7 items, each scored from 0 to 3, giving a total score out of 21; higher scores indicate higher levels of anxiety symptoms. It has been suggested that a cutoff of 10 be used as an indicator of anxiety “caseness”. 18 The reliability for the GAD-7 in our sample was good. Cronbach's α coefficient was 0.903 for the entire sample and 0.902 and 0.903 for pregnant and postnatal women, respectively. The reliability by country and the range from minimum to maximum in GAD scores are shown in Supplementary Tables S3A and S4A.
Statistical analysis
Survey data were manually checked for accuracy and consistency before analysis. Normality of the data was explored through the Q-Q plot graph and through the skewness and kurtosis statistics. They all confirmed normal distribution of the data. Data were analyzed using SPSS version 26.0 statistical software. Descriptive data analyses were performed to report frequencies and percentages for categorical data and means and standard deviations (SD) for continuous variables. 21 Differences between included versus excluded participants were explored using the χ 2 statistic (between categorical variables) or Student's t-test (when the dependent variable was continuous). In addition, differences between COVID-19-related variables and perinatal depression and anxiety by GDM status were examined using the χ 2 statistic (between categorical variables) or Student's t-test (with a continuous variable as dependent).
Effect sizes were presented following the interpretation proposed by Cramer's V and Cohen's d as follows: 0–0.19: negligible, 0.20–0.49: small, 0.50–0.79: medium, and 0.80 and above: high. 22 To control for the effect of country as a cluster over the relationships between the exposure and the outcomes, linear and logistic multilevel regression analyses, stratified by pregnant or postnatal status, were performed for continuous and categorical variables, respectively. A null model to test the adequacy of the inclusion of country as a cluster was performed before this. In addition, analyses involving mental health measures were adjusted for the relevant confounders of age, education, employment status, the date of survey completion, and for the pregnant subgroup, gestational age, as per the principles of confounder selection. 23 All p-values were two sided and considered significant below 0.05. All confidence intervals (CI) were reported at 95%.
Sensitivity analyses
Women who responded to the survey in the postnatal period and based on their date of delivery were likely to have experienced GDM before the onset of the pandemic in March 2020, were removed from the group of women with GDM in the comparison of EPDS and GAD-7 continuous scores between those with and without GDM. A second sensitivity analysis involved removing women who reported a history of diabetes (pregestational diabetes) from the sample.
Results
Sample characteristics
Characteristics of the sample are presented in Table 1. The mean age of participants was 32 years. Around 45.6% of the women were pregnant at the time of baseline survey completion and 54.4% were up to 6 months postnatal. For pregnant women, the mean gestational age in weeks was 27.27 (SD 8.5). Approximately 9.6% of the women reported being diagnosed with GDM. The majority (96.7%) of the sample reported being married or co-habiting with a partner. Sixty-nine percent of women were in employment; this included maternity leave. Around 72.7% of the sample had a higher education (college degree or higher).
Participant Characteristics
EPDS, Edinburgh Postnatal Depression Scale; GAD-7, Generalized Anxiety Disorder 7 items; GDM, gestational diabetes mellitus; SD, standard deviation.
The sample included women from Brazil, Chile, Cyprus, Greece, Israel, Malta, Portugal, Spain, Turkey, and the United Kingdom. Approximately 10.2% of women reported having been infected with COVID-19 themselves and 10.7% had been in contact with somebody infected. Around 40.3% of women in the sample scored ≥11 on the EPDS, with 29.9% scoring ≥13. On the GAD-7, 23.5% scored ≥10.
Analysis of missing data
Supplementary Table S5A compares the characteristics of the 7,371 included respondents to the 6,182 excluded among the 13,553 participants who fulfilled inclusion criteria. The analysis sample was older (mean age 32 years vs. 30 among those excluded). The effect sizes for differences between other variables were negligible (work status, stage of the peripartum, GDM status, and level of distress about future employment and finances related to the pandemic).
Symptoms of anxiety and depression in women with versus without GDM
Table 2 compares levels of symptoms on the EPDS and GAD-7 as both a continuous score and as a dichotomous variable above or below the prespecified cutoff scores adjusted for cofounders and cluster effect (country). In pregnant women, there was evidence of an association between GDM and increased levels of depression (p < 0.001), which was robust to adjustment for age, education, employment status, date of the survey, and gestational age. It must be noted that there was no evidence of an association with anxiety symptoms, nor for depression defined as EPDS ≥13. Regarding postnatal women, there was evidence of an association between GDM and increased levels of anxiety (p < 0.001) and depression (p < 0.001), which was robust to adjustment for age, education, employment status, and date of the survey.
Mental Health Symptoms in Women With Versus Without Gestational Diabetes Mellitus
Adjusted for cluster effect (country).
Adjusted for cluster effect (country) and covariates (age, educational level, work status, survey date, and gestational age).
Adjusted for cluster effect (country) and covariates (age, educational level, work status, and survey date).
95% CI, 95% confidence interval; OR, odds ratio.
Experiences of COVID-19 in women with versus without GDM
There was no evidence of an association between GDM and COVID-19 infection (p = 0.819) in either pregnant or postnatal women (Table 3). However, in pregnant women, concerns about future employment and finances (adjusted mean difference: 0.27; 95% CI 0.0205 to 0.519; p = 0.034) were higher in women with GDM. In postnatal women, levels of personal COVID-19-related distress (adjusted mean difference: 0.31; 95% CI 0.105 to 0.520; p = 0.003), concerns about future employment and finances (adjusted mean difference: 0.22; 95% CI 0.027 to 0.418; p = 0.026), and overall level of distress (adjusted mean difference: 0.19; 95% CI 0.029 to 0.359; p = 0.021) were higher in women with GDM versus without GDM.
COVID-19-Related Variables in Women With Versus Without Gestational Diabetes Mellitus
Adjusted for cluster effect (country).
Sensitivity analyses
Removal from the GDM group of those participants (N = 30) who were postnatal and experienced GDM before the pandemic resulted in little change to mean scores on the EPDS and GAD-7 in the GDM group; there remained evidence of an association between GDM and higher levels of anxiety and depression (Table 4).
Sensitivity Analysis, Excluding Those Who Were Postpartum and Experienced Gestational Diabetes Mellitus Before the COVID-19 Pandemic (N = 30)
Adjusted for cluster effect (country).
Adjusted for cluster effect (country) and covariates (age, educational level, work status, survey date, and gestational age).
When women who reported a history of diabetes before pregnancy (N = 310) were removed from the analysis, there was less evidence than had been observed in the primary analysis, of an association between GDM and depression symptoms (Table 5).
Sensitivity Analysis, Excluding Those Who Reported a History of Diabetes (N = 310)
Adjusted for cluster effect (country).
Adjusted for cluster effect (country) and covariates (age, educational level, work status, survey date, and gestational age).
Adjusted for cluster effect (country) and covariates (age, educational level, work status, and survey date).
Discussion
Main findings
In this sample of 7,371 perinatal women surveyed during the COVID-19 pandemic, a cross-sectional association was observed between self-reported GDM and increased levels of depression symptoms during pregnancy and anxiety and depression symptoms postpartum. Women with GDM also experienced higher levels of pandemic-related distress, particularly postpartum, which may help to explain the greater differences between women with versus without GDM in the postpartum than during pregnancy. Women with GDM did not appear to have experienced higher levels of COVID-19 infection.
Strengths and limitations
This is the first study to investigate the relationship between GDM and common mental disorders during the COVID-19 pandemic. The analysis also considered differences across a number of COVID-19-related variables, which may affect mental health. This was done in a large sample, including participants from across 10 different countries. Well-validated instruments were used to measure mental health, which also exhibited adequate levels of reliability in this sample.
Nonetheless, the findings must be interpreted with caution. First, many of the effect sizes were small. Moreover, the evidence for a relationship between GDM and increased levels of symptoms represents cross-sectional associations; research suggests that the association between GDM and common mental disorders may be complex and bidirectional. 3,24 There were also no measures of prepandemic mental health in this sample; so it is unclear the extent to which the increased levels of anxiety and depression in women with GDM are due to factors relating to the pandemic, although the GDM group had higher levels of pandemic-related distress.
Other limitations inherent in an observational study design, which restrict causal inference, are the issues of bias and confounding. One potential source of bias is that from missing data, although a comparison of included versus excluded participants did not reveal differences with a significant effect size, except age, with included participants being older than excluded. While analyses were adjusted for a range of hypothesized sociodemographic confounders of the association between GDM and mental health, another important potential confounder is ethnicity; there is an increased risk of GDM, and possibly perinatal common mental disorders, in Black and South Asian women. 25,26 However, unfortunately, the survey only asked respondents whether or not they were born in the country in which the survey was administered, which is not indicative of ethnic group.
While the sample is drawn from a range of European and South American countries, representing a range of settings, it is also important to note that different countries may have been experiencing the pandemic in different ways during the period of data collection; for example, the onset of the pandemic in South America lagged behind Europe. 27 Stratification of analyses by country was considered, but would have resulted in a number of very small subsamples.
Findings in context
In this sample, around 40% of participants scored ≥11 on the EPDS, with 30% scoring ≥13. Approximately 24% scored ≥10 on the GAD-7. It is important to note that questionnaire measures of mental disorder can only ever provide information on levels of symptoms, with “caseness” reflected above a prespecified threshold score. This does not equate with a clinician-diagnosed disorder. Nonetheless, these levels are somewhat higher than would be expected in the perinatal population. 28,29 This may be a result of pandemic-related stressors. These include changes to maternity care delivery, social isolation, uncertainty surrounding the effect of COVID-19 infection on pregnant and breastfeeding women and their developing infants, and increases in domestic violence and abuse. 5,6
Indeed, levels of common mental disorder symptoms in this analysis are similar to that of a recent meta-analysis of studies conducted during the pandemic, although conversely to this analysis, anxiety levels were higher compared with depression in the meta-analysis. 8 Another factor impacting the estimates in this analysis is the study design; surveys may over-represent those who are particularly distressed and keen to voice their distress. Moreover, the convenience nature of the survey sample is reflected in the participant characteristics, which suggest relatively low levels of socioeconomic deprivation (73% reported achieving higher education).
The frequency of self-reported GDM in the sample of around 10% equates to wider population prevalence, 4 suggesting face validity of the self-report measure utilized in the survey. However, it should be acknowledged that diagnostic criteria differ substantially between countries. 4 Moreover, the change in results observed in sensitivity analysis, excluding women who reported experiencing diabetes before pregnancy, suggests that women with pregestational diabetes erroneously reporting gestational diabetes may have influenced the results. The body of research exploring the relationship between GDM and mental health is growing, although findings are mixed as to whether or not there is an increased risk of perinatal common mental disorders in those with GDM. 3 A range of mechanisms have been postulated, including biological ones such as inflammation.
However, qualitative research has also explored the thoughts and feelings of women experiencing GDM, such as guilt and fear, 30,31 which may also impact their mental health. The finding in this analysis that women with GDM experience greater levels of pandemic-related distress suggests that there may be additional stresses associated with the pandemic disproportionately affecting those with GDM, which may affect mental health. During the pandemic, women with GDM experienced a reduction in face-to-face health care and the uncertainties associated with changes to clinical care guidelines, including more remote delivery of care through telemedicine, changes to GDM screening protocols, and delays to type 2 diabetes screening in the postpartum. 32 The impact of such changes on the physical and mental health of women with GDM is not yet known.
Conclusions
Future research could usefully focus on exploring further the experiences of women with GDM during the pandemic. Greater understanding of these experiences could inform initiatives aimed at providing more support for this population to address sources of pandemic-related distress. The findings of this analysis highlight the importance of prompt and holistic assessment and management of women in the perinatal period focusing on both physical and mental health during the current pandemic and beyond.
Footnotes
Authors' Contributions
E.M. and A.M. are principal investigators on the Riseup-PPD COVID study from which data for this analysis are drawn. C.A.W., E.M., R.C., A.M., E.V., Y.C.-G., D.L., V.M., A.C., E.F., and P.D.-Y. were involved in recruitment of participants to the survey. C.A.W. conceived the research question and designed the study analysis plan. All authors approved the data analysis plan. I.G.-G. conducted the data analyses. C.A.W. and E.M. wrote the first draft of the article. All authors critically revised this draft and have approved the final version.
Acknowledgments
The authors would like to thank all women who participated in the survey.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This paper is part of the European Cooperation in Science and Technology (COST) Action Riseup-PPD CA18138 and was supported by COST under COST Action Riseup-PPD CA18138. R.C. is supported by the FSE and FCT under an individual Post-Doctoral Grant SFRH/BPD/117597/2016. D.L. received funding from the Bar-Ilan Dangoor Centre for Personalized Medicine, Israel. C.A.W is supported by the UK's National Institute for Health and Care Research (NIHR). Open access fees from an NIHR senior investigator grant (NIHR200241).
Supplementary Material
Supplementary Table S1A
Supplementary Table S2A
Supplementary Table S3A
Supplementary Table S4A
Supplementary Table S5A
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.