
Abstract
Background:
Maternal mortality decreased globally by about 38% between 2000 and 2017, yet, it continues to climb in the United States. Gaping disparities exist in U.S. maternal mortality between white (referent group) and minority women. Despite important and appropriate attention to disparities for black women, almost no attention has been given to American Indian/Alaska Native (AI/AN) women. The purpose of this scoping review is to synthesize available literature concerning AI/AN maternal mortality.
Methods:
Databases were searched using the terms maternal mortality and pregnancy-related death, each paired with American Indian, Native American, Alaska Native, Inuit, and Indigenous. Criteria (e.g., hemorrhage) were paired with initial search terms. Next, pregnancy-associated death was paired with American Indian, Native American, Alaska Native, Inuit, and Indigenous. Criteria in this category were homicide, suicide, and substance use.
Results:
The three leading causes of AI/AN pregnancy-related maternal mortality are hemorrhage, cardiomyopathies, and hypertensive disorders of pregnancy. AI/AN maternal mortality data for homicide and suicide consistently include small samples and often categorize AI/AN maternal deaths in an “Other” race/ethnicity, which precludes targeted AI/AN data analysis. No studies that reported AI/AN maternal mortality as a result of substance use were found. Health care characteristics such as quality, access, and location also may influence maternal outcomes and maternal mortality.
Conclusions:
Despite AI/AN maternal mortality being disproportionately high compared to other racial/ethnic groups, relatively little is known about root causes.
Introduction
A
An indicator of a society's health, the maternal mortality ratio (MMR; maternal deaths per 100,000 live births) decreased globally by about 38% between 2000 and 2017, 2 yet, it continues to climb in the United States. Ranked worst in the developed world, the United States reports almost 700 pregnancy-related deaths annually. 3 In 2018, the U.S. MMR was 17.4, 4 with 60% of these deaths deemed preventable. 5
Gaping disparities exist in U.S. maternal mortality between white (referent group) and minority women. The Centers for Disease Control and Prevention's Pregnancy Mortality Surveillance System (PMSS) data (2007–2016) show an overall pregnancy-related mortality ratio (PRMR; pregnancy-related deaths per 100,000 live births) of 16.7 for the general population of U.S. women; the PRMR for white women was 12.7. 3 For non-Hispanic black and American Indian/Alaska Native (AI/AN) women, PRMR was 40.8 and 29.7, respectively, 3 revealing a persistent racial/ethnic disparity. Although education can be protective, AI/AN women with some college education had higher PRMR than all other racial/ethnic groups with less than a high school diploma. 3 Despite important and appropriate attention to disparities for black women, almost no attention has been given to AI/AN women.
The purpose of this scoping review is to synthesize available literature concerning AI/AN maternal mortality. Specific aims are to determine leading cause(s) of AI/AN pregnancy-related and pregnancy-associated maternal mortality 6 (Table 1), identify and analyze gaps in the literature, and recommend directions for future research.
Maternal Mortality Terminology
Source: Centers for Disease Control and Prevention (CDC). 6
Background and Significance
AI/AN people experience unequal rates of chronic disease and mortality, as well as poorer health outcomes. 7 AI/AN life expectancy at birth is 5.5 years less than the general U.S. population. 8 Since the colonization of America, certainly the greatest insult to AI/AN health, health disparities have persisted. 9 Colonization introduced destruction through wars, disease, and loss of land—all resulting in the significant loss of life and decimation of populations. 9,10 Later, such federal policies as the reservation system and assimilation through boarding schools perpetuated social injustice and worsened AI/AN health. 9
AI/AN people have a unique history with the U.S. federal government. Treaties promised health care and other services to AI/AN people in exchange for natural resources and vast tracts of land. 11 Established in 1955, the Indian Health Service (IHS) administers comprehensive health services to 574 federally recognized tribes. 12 Resource deficiency and underfunding, however, continue to impede optimal health services, partly from inadequate numbers of providers and dwindling numbers of hospitals as facilities age and close. 13 Furthermore, not all AI/AN tribes are federally recognized and some are therefore ineligible for IHS services. In addition, urban AI/AN residents often do not have access to IHS services.
Methods
Using the PRISMA extension for scoping reviews checklist, 14 we comprehensively assessed and synthesized the maternal mortality literature concerning AI/AN women. An AI/AN woman was defined as any female who is a member of an Indigenous tribe, band, or nation who maintains affiliation or community attachment.
The search strategy included Cumulated Index to Nursing and Allied Health Literature (CINAHL) Complete, Google Scholar, MEDLINE, MEDLINE Complete, PsycARTICLES, Psychology & Behavioral Sciences Collection, and PubMed databases, searched up to March 2020. Initial search terms were maternal mortality and pregnancy-related death, each paired with American Indian, Native American, Alaska Native, Inuit, and Indigenous. Next, specific criteria (e.g., hemorrhage) were paired with the initial search terms, based on CDC's mutually exclusive categories of pregnancy-related causes of death 5 (Table 2). Next, pregnancy-associated death was paired with American Indian, Native American, Alaska Native, Inuit, and Indigenous. Specific criteria in this category were homicide, suicide, and substance use.
Pregnancy-Related Causes of Death
CV, cardiovascular.
Source: Petersen et al. 5
Abstracts were reviewed to identify relevant articles, and reports were read in full if deemed relevant or if their relevance was uncertain. Irrelevant, duplicate, and non-English language articles and research outside the United States were excluded. Additional citations were retrieved manually from selected articles' reference lists. The search produced a final yield of 21 articles (Fig. 1).
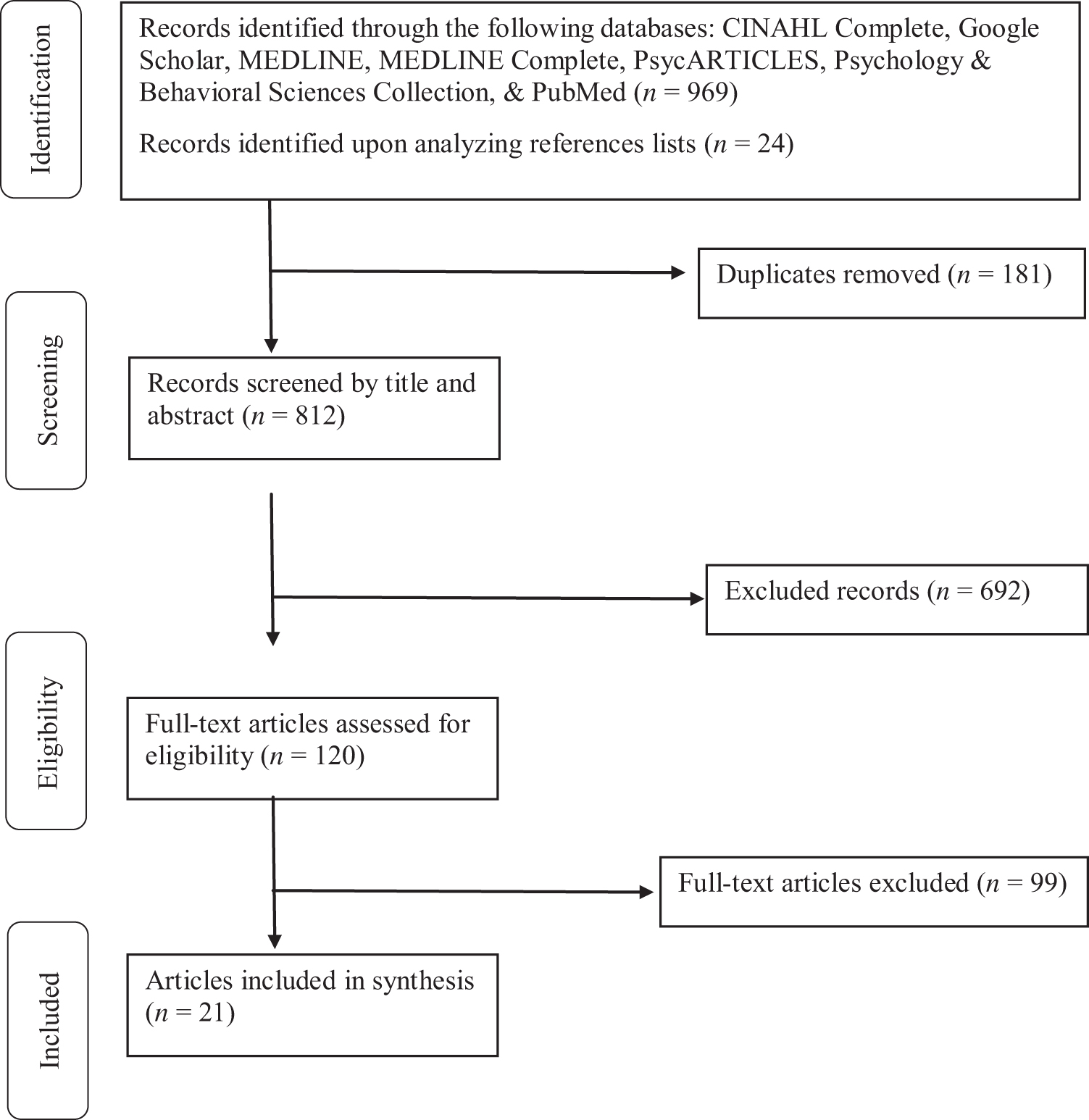
Flow diagram of study selection that sequences the review process. CINAHL, Cumulated Index to Nursing and Allied Health Literature; MEDLINE, online counterpart to MEDLARS (Medical Literature Analysis and Retrieval System); the U.S. National Library of Medicine® premier bibliographic database. Adapted from Moher et al. 72
Results
Results are discussed according to search categories (Tables 3 –5). Not all reviewed studies used the racial/ethnic category “American Indian/Alaska Native.” Some used “American Indian” or “Native American” alone; therefore, our results do also. No studies discussed Alaska Native women alone.
Summary of Pregnancy-Related Causes of Death Studies (N = 6)
AI/AN, American Indian/Alaska Native; N/A, not applicable; PMSS, Pregnancy Mortality Surveillance System; PRAMS, Pregnancy Risk Assessment Monitoring System; R/E, race/ethnicity.
Summary of Pregnancy-Associated Causes of Death Studies (N = 9)
NYC, New York City; VDRS, Violent Death Reporting System.
Summary of Socioecological and Health Care Influences Studies (N = 6)
NCHS, National Center for Health Statistics; NLBID, National Linked Birth & Infant Death; NR, not reported; PNC, prenatal care.
Pregnancy-related maternal mortality
The three leading causes of AI/AN pregnancy-related maternal mortality are hemorrhage (19.7%), cardiomyopathies (14.5%), and hypertensive disorders of pregnancy (12.8%). 3
Cardiovascular complications
Cardiovascular disease is the leading cause of U.S. maternal death, responsible for over 33% of pregnancy-related deaths. 5 The national trends of delayed childbearing and more chronic disease mean more women enter pregnancy with medical comorbidities (e.g., diabetes, obesity, and hypertension), and prevalence of these conditions is higher among AI/AN women. 18
In PMSS data (2007–2016) cardiomyopathy accounted for 14.5% of AI/AN pregnancy-related maternal mortality, representing a greater proportionate cause of death than any other racial/ethnic group; among black and white women, cardiomyopathy accounted for 14.2% and 10.2% of mortality, respectively. Other cardiovascular complications (e.g., congenital heart disease), accounted for 11.1% of AI/AN pregnancy-related mortality, a smaller proportionate cause of death than other racial/ethnic groups. 3
Obstetric/noncardiovascular complications
In PMSS data (2007–2016), hemorrhage (19.7%) and hypertensive disorders of pregnancy (12.8%) accounted for a significantly higher proportion of AI/AN than white pregnancy-related maternal mortality (p < 0.05), higher than all other racial/ethnic groups. White rates of pregnancy-related maternal mortality for these conditions were 9.1% and 6.7%, respectively. 3
In a retrospective study of 1062 women, postpartum hemorrhage and uterine atony were significantly higher in Native American than white women. 15 Higher rates of severe maternal morbidity in Native American women are driven largely by blood transfusions. 15 The reasons for increased postpartum hemorrhage and more blood loss in AI/AN women are unknown. Further research is urgently needed in this area.
AI/AN women in Washington State had a 17% increased risk of preeclampsia compared to white women, even after adjusting for age, socioeconomic status, and smoking. 19 Obesity was a confounder, highlighting an important risk factor for pregnancy-related morbidity and mortality. 19 Hypertensive disorders first diagnosed during pregnancy were also higher for AI/AN than white women (12.8% and 6.7%, respectively, p < 0.05). 3 Deaths related to noncardiovascular medical conditions (e.g., renal) were similar between AI/AN and white women. 3
In a sample of 89,076 women who had cesarean deliveries with epidural catheters, anesthesia complications were more common in Native American women than other racial/ethnic groups; no difference existed in rates of amniotic fluid embolism. 16 Contrasting other causes of maternal death, AI/AN women had a significantly lower proportion of infection compared with white women (8.5% and 15.2%, respectively, p < 0.05). 3
Pregnancy-associated maternal mortality
Homicide
Maternal deaths attributable to homicide, as well as suicide, often are associated with intimate partner violence (IPV). 26,35 For instance, 45.3% of pregnancy-associated homicides are associated with IPV. 26 Lifetime and 12-month prevalence rates of IPV are consistently higher for AI/AN (47.5%) than white women (37.3%), and AI/AN women have the highest reported IPV prevalence of all other racial/ethnic groups. 36
Eight studies explored AI/AN maternal deaths by homicide; because of data privacy policies, all studies used an “Other” racial/ethnic category instead of AI/AN, because there were too few cases to discuss. Homicide rates for “Other” women ranged from 0% to 3.8%. 20 –23,26 –28 Although this rate appears consistently low, homicide remains a leading cause of pregnancy-associated injury deaths in the United States. 22,26,35 Disparate numbers of missing and murdered Indigenous women 37 suggest that homicide may be responsible for more pregnancy-associated AI/AN deaths than has been recognized to date.
Suicide
A leading cause of death and disability in the United States, suicide among AI/AN people is higher than all other racial/ethnic groups. 7 An intimate partner conflict potentially contributed to 54.3% of pregnancy-associated suicides. 26 Nine studies investigated AI/AN maternal deaths by suicide. Mirroring homicide data, small samples and categorization as “Other” race/ethnicity precludes targeted AI/AN data analysis.
Reporting of AI/AN maternal suicide deaths is inconsistent. Palladino et al. 26 reported that prenatal and postpartum suicide disproportionately affects AI/AN and white women, yet, others report little or no risk for AI/AN women. 20,21,23 –25,27 This result could be explained partially by the use of an “Other” race/ethnicity category; Palladino et al. was the only study that reported AI/AN women as AI/AN versus “Other.”
One study combined suicide with accidental overdose and reported 4 out of 59 maternal deaths for “non-Hispanic Others” 25 ; although this report was likely for statistical purposes, it only complicates matters. One study that included AI/AN maternal deaths as “Other” still reported too few suicides to discuss. 21 Suicide rates for “Other” women (an unknown portion of which were AI/AN) ranged from 0% to 13.3%. 20,23,24,27,28,38
Substance use
We found no studies examining AI/AN pregnancy-associated maternal mortality from substance use. Most data examine prevalence of tobacco use, which is higher for AI/AN than white women. 17 In Alaska, prenatal tobacco use was threefold higher for Alaska Native (43.4%) than white women (13.4%). 17 Danielson et al. found markedly elevated risk of smoking, alcohol, and illicit drug use during pregnancy among AI/AN women compared to white women. 39 The AI/AN to white ratios for use of these substances were 2.6, 6.4, and 3.1, respectively. 39 In a report of overdose deaths, AI/AN rates for all opioids were higher than all other racial/ethnic groups except whites; rates were not disaggregated by gender within racial/ethnic categories. 40 These data suggest that overdose may account for more pregnancy-associated AI/AN deaths than is generally recognized.
Socioecological and health care influences
Poor perinatal outcomes are associated with poverty, lack of education, and neighborhood-level factors. 41 Understanding the complex interactions among social determinants (root causes) of health is crucial to understanding effects on maternal outcomes. 42 Health care characteristics such as quality, access, and location may also influence maternal outcomes.
Health care quality
Disparities in health care quality related to maternal mortality have been examined largely from a racial perspective of white versus nonwhite or black. Although information specific to AI/AN people is lacking, existing models may be applicable. Howell 43 developed a conceptual model depicting pathways to racial/ethnic disparities in severe maternal morbidity and mortality that examines patient, neighborhood, provider, and system-level factors.
Prenatal care
Adequate prenatal care (PNC) improves perinatal outcomes, 44 yet, about 13% of AI/AN women receive late (i.e., third trimester initiation) or no PNC, compared to 4.5% of white women. 33 In urban settings, AI/AN women received late or no PNC at twice the rate of all other women combined. 30 This may be explained partially by barriers they already experience, such as lack of health insurance or reliable transportation. 32
Poor understanding of AI/AN culture and inability to tailor care to the unique needs of AI/AN women are provider characteristics that negatively affect PNC quality. 34 AI/AN women reported such negative provider experiences as disrespect and being stereotyped as “drunks and drug users.” 32,34,45 The inability to see one provider throughout pregnancy, providers that seemed too busy to address concerns, and hearing negative stories from others were additional barriers. 32
Relationships between PNC and maternal outcomes are complex, comprising more than simply timing and number of visits. Location can influence the likelihood of adequate PNC (operationalized with various measures); 14.4% of all urban AI/AN women received inadequate PNC, but rates ranged from 4.4% to 29.8% based on location. 31 Even larger disparities appeared in rural settings, with 33.9% of AI/AN women receiving inadequate PNC compared to 13.5% of white women. 29
Rural-urban influences
Although rurality is associated with increased maternal morbidity and mortality, AI/AN maternal morbidity and mortality exceeded that for white women in both rural and urban locations. 18 Also noted were increased rates of blood transfusion among AI/AN women, particularly in rural settings, 18 which is consistent with other reports that blood transfusions appear to drive severe maternal morbidity. 15 When blood transfusion, as the sole marker of severe maternal morbidity and mortality, was removed from the analysis, AI/AN women still experienced higher rates of severe maternal morbidity and mortality. 18
Discussion
Despite AI/AN maternal mortality being disproportionately high compared to other racial/ethnic groups, relatively little is known about the root causes. Research examining causation points to higher rates of hemorrhage and pregnancy-associated hypertension (obesity may contribute), 3 but these causes do not account entirely for the increase in deaths compared to other racial/ethnic groups. Even less is understood about AI/AN pregnancy-associated deaths, with divergent studies reporting that suicide disproportionately affects AI/AN women 26 while others report the opposite. 20,21,23 –25,27 Mental illness contributes to U.S. maternal mortality and is a leading cause of death. 46 Although suicide can be a consequence of mental illness such as depression, 47 we found no studies exploring the relationship between depression and AI/AN maternal mortality. Given that AI/AN women experience more postpartum depression than white women, 48 –50 further investigation into postpartum depression and other mental illness as root causes is warranted. In addition, pregnancy-associated homicide deaths might be disproportionate among AI/AN women of childbearing age because they experience increased rates of IPV and homicide.
Historical trauma is considered a significant social determinant of health for AI/AN people, 9,10 resulting from cumulative exposure to traumatic events produced by colonization. 51 It manifests in subsequent generations as depression, substance use, diabetes, and other adversities that damage social determinants of health. 52 Comorbidities such as mental illness and substance use increase the likelihood of maternal morbidity and mortality. 42 IPV is another cumulative trauma that can result in adverse physical and psychological effects.
Life expectancy at birth has increased among all U.S. racial/ethnic groups, yet, AI/AN people continue to die at younger ages than the general population. 53 Consistent with the weathering hypothesis, this effect might be explained partially by barriers to quality health care that AI/AN people face. The weathering hypothesis suggests that cumulative stress from racism and socioeconomic disadvantage produces a weathering effect on health that can explain disparate outcomes. 54 Weathering degrades health across the lifespan, making it more difficult for women of color to enter pregnancy in optimal health. 55 Perhaps the same is true for maternal mortality; a recent analysis supports the weathering hypothesis for AI/AN and black women. 3
Inequities in health care availability, access, and utilization warrant elucidation to decrease AI/AN maternal mortality 56 because systems-level factors (e.g., facility clinical processes) are linked to maternal morbidity and mortality. 41 Widespread use of midwives could play a key role; on national and international levels, midwife-led care is an important contributor to improved quality of care and perinatal outcomes. 55,57,58 Approaches to improve delivery might include care coordination, home visiting, telehealth, and peer support. 5,25 To reduce AI/AN maternal mortality and eliminate racial/ethnic disparities, provider-related factors such as inappropriate management and implicit bias must be addressed via targeted cultural humility, trauma-informed care, quality improvement, and other types of training. 5,34,55
Although this scoping review focused on AI/AN maternal mortality, we identified many studies concerning AI/AN maternal morbidity linking preexisting health conditions (e.g., obesity) to increased mortality risk. AI/AN and black women reported the highest number of stressful life events in the year preceding childbirth, 59 and stress and racism might influence maternal morbidity and mortality. 60 Of all racial/ethnic groups, AI/AN women were most likely to report having two or more risk factors (e.g., at-risk drinking, smoking) for adverse perinatal outcomes. 61 Obesity, high school noncompletion, diabetes, and fewer than 10 prenatal visits have been linked to maternal mortality for some racial/ethnic groups of women, 62 but we found no evidence for AI/AN women specifically.
Consistent with long-standing data collection issues, 63 we offer multiple reasons for AI/AN data paucity and limitations. The absolute number of AI/AN pregnancy-related and pregnancy-associated deaths is small. For example, in PMSS data analyses (2007–2016), only 117 AI/AN maternal deaths were reported. 3 Studies examining pregnancy-related mortality often exclude deaths from trauma. 64 In addition, with low numbers, cases are discussed together to protect confidentiality and privacy. 21,26,38 AI/AN maternal deaths are classified in an “Other” racial/ethnic category where the AI/AN proportion could be anywhere from 0% to 100%, complicating interpretation of AI/AN maternal mortality. This lack of data prevents clear understanding and hindered us from determining leading cause(s) of AI/AN pregnancy-associated maternal mortality. Ultimately, this practice obstructs intervention development to address root causes of AI/AN maternal mortality.
Racial/ethnic misclassification on death certificates potentially leads to underreporting 26 and compromised estimates of mortality, with as many as 45% of AI/AN deaths being misclassified as another race. Given the relatively small AI/AN population, even negligible misclassifications can markedly affect data analyses, 65 likely resulting in an underestimation of AI/AN maternal mortality.
Given the historical trauma 10,66 and medical and research abuses 67 that AI/AN people have experienced, research teams are more successful when they elicit tribal interest and engage communities in setting research agendas. Research partnerships are more meaningful when teams include or are led by Indigenous researchers. For these reasons, community-based participatory research (CBPR), or similar approaches that center on community needs, produces mutually beneficial outcomes and is often favored by tribes. 68 –70 CBPR has contributed to reducing health disparities while providing equity in research relationships with tribal groups. 71
Conclusion
AI/AN women die at disproportionate rates during and in the year following pregnancy compared to white women. Together, hemorrhage, cardiomyopathy, and hypertensive disorders of pregnancy might account for nearly half of AI/AN pregnancy-related deaths, and drivers of severe maternal morbidity include obesity, diabetes, and blood transfusions. Homicide, suicide, and substance use, all linked to IPV, clearly contribute to AI/AN pregnancy-associated maternal mortality, yet, severe data limitations prohibit our understanding of true incidence and prevalence.
Although specific and cumulative impacts of social and structural determinants on AI/AN maternal mortality have received little attention, implications may be drawn cautiously from what is known about existing disparities. Inadequate PNC and culturally uninformed health care increase risk for AI/AN maternal mortality. Unequal care and structural racism undoubtedly affect U.S. maternal mortality, and the complex role of AI/AN identity in increased maternal mortality demands further examination. Investing in participatory research approaches and community-driven programs to improve early access to quality health care warrants further attention in diverse rural and urban tribal communities to optimize AI/AN maternal health. Amidst ongoing federal, state, and local efforts to address maternal mortality, researchers must use novel approaches to collect meaningful data, elucidate root causes, guide public health efforts, and inform policy to improve maternal health outcomes and reduce AI/AN maternal mortality. Until this is accomplished, history will continue to repeat itself.
Footnotes
Disclaimer
The information contained herein is not the official position of the IHS.
Author Disclosure Statement
All the authors disclose no competing, personal, or other financial interests.
Funding Information
No funding was received for this article.