
Abstract
Background:
Peripheral artery disease (PAD) is a common cardiovascular pathology that affects mobility. In previous research, supervised exercise, a recommended treatment for claudication, was less effective in women. This study retrospectively investigated whether functional outcomes exhibit sex differences following a pain-free, home-based exercise program for PAD patients.
Materials and Methods:
Patients with PAD and claudication enrolled to a structured home-based program from 2003 to 2016 were studied. The program was prescribed at the hospital and based on two daily 10-minute pain-free walking sessions at progressively increasing speed. Outcome measures, which were assessed at baseline and discharge, were pain threshold speed (PTS) and maximal (Smax) during a treadmill test and pain-free walking distance (PFWD) and total distance walked in 6 minutes (6MWD). The ankle-brachial index (ABI), program duration, and patient adherence were determined.
Results:
A total of 1007 patients (women; n = 264; 26%) were enrolled. At baseline, compared to men, women exhibited similar ABI values but lower PTS and PFWD values (p < 0.001). At discharge, with similar adherence (score 3/4 ± 1 each) in both groups, superimposable improvements were observed for PTS (0.8 ± 0.8 km/h each), Smax (0.4 ± 0.5 km/h each), PFWD (women 95 ± 100; men 86 ± 104), 6MWD (women 32 ± 65; men 35 ± 58), and ABI (women 0.07 ± 0.12; men 0.06 ± 0.11) without between-group differences (confirmed after propensity analysis).
Conclusion:
A personalized, structured pain-free exercise program for PAD patients performed inside the home for a few minutes a day was equally effective in both sexes. Programs favoring adherence and functional outcomes in women should be tested in prospective studies.
Introduction
Cardiovascular disease (CVD) remains the primary cause of death in women, with an estimated 44 million women either living with or at risk of heart disease in the United States. 1 Resistant hypertension, 2 poor lipid control due to either lack of social support 3 or higher discontinuation of lipid-lowering treatment, 4 and even mild-to-moderate reduced kidney function 5 are all novel pieces of the complex puzzle of the gender gap in CVD. Among the wide spectrum of CVDs, peripheral artery disease (PAD) is a highly prevalent pathology in the elderly; it is responsible for disability and reduced quality of life (QoL) at the intermediate stages. 6 However, the burden of PAD is increasingly striking in young adults 7 and women. Due to the increased disability and mortality associated with PAD in the past 20 years, 7 the prevalence in women is equal to that in men. 7 –9 Although women with PAD may be more frequently asymptomatic or report atypical symptoms 9 in the presence of claudication, compared to men, they show lower functioning even with similar hemodynamic severity, 10 a higher prevalence of mood disturbance, and bodily pain. 11
In terms of treatment, the female sex also represents a risk factor that negatively affects vascular intervention outcomes, with a differential impact according to race and intervention type. 12 –17 For the abovementioned reasons, exercise therapy and primary treatment of claudication symptoms 6 might be crucial for the management of walking disabilities among women. Unfortunately, a lower response or adherence to rehabilitation has been reported in women with various chronic diseases 18 –20 as well as with PAD, possibly due to interest, comorbidities, or rehabilitation strategies. 21 –23
An alternative model of unsupervised rehabilitation based on a structured, home-based, personalized, symptom-free prescription of exercise with only monthly check-ups at the hospital (test in–train out, Ti-To) has been developed for PAD. 24,25 The model, which aimed to overcome many barriers to exercise, has also been successfully tested in several selected populations, for example, dialysis patients 26 –28 and stroke survivors, 29,30 and obtained significant functional and clinical improvements.
Since this model has sustainable and feasible features such as setting, intensity, and low impact that could be suitable for women, we hypothesized that equal improvements in functional outcomes are attainable after rehabilitation in both women and men. The aim of this study was to evaluate whether sex-based differences in PAD patients with claudication are observable at discharge from the program.
Materials and Methods
Study design and setting
This single-center, retrospective cohort study was carried out at the Department of Rehabilitation Medicine of the Azienda Ospedaliero-Universitaria of Ferrara between 2003 and 2016. The study was developed during usual care practice for PAD patients at this hospital. The local ethics committee of the University of Ferrara approved the study; no written informed consent was obtained from the patients because they no longer attended the program. This article was written according to the Strengthening the Reporting of Observation Studies in Epidemiology (STROBE) checklist for cohort studies. 31
Participants
A total of 1164 PAD patients who had attended the vascular rehabilitation program were analyzed for possible inclusion in the study. PAD was previously diagnosed at the vascular surgery unit of the Hospital of Ferrara by clinical and echo-color-Doppler examination. 32
Patients of all ages and sexes were included in the study based on the presence of PAD at stage II of the Leriche–Fontaine classification, with stable claudication for at least 3 months. Patients with conditions contraindicating safe training execution at home (e.g., unstable angina, severe heart failure, major amputation, or clinical conditions limiting treadmill testing) were excluded from the analysis. Finally, patients who did not complete the exercise program for any reason were not included in this analysis.
Variables and comorbidities at entry
During the first session of the program, information regarding clinical status and functional impairment was collected by consulting patients' medical documents by means of physician examination or by specific tests. Particularly, scholar qualification, cardiovascular risk factors, comorbidities adjunct to PAD (with the Charlson comorbidity index calculation 33 ), and location of endovascular lesions were identified. Patients' reported claudication distance was also noted.
Outcome measures
Hemodynamic and functional measurements were performed at entry and discharge from the rehabilitation program. All outcome measures were carried out in a temperature-controlled environment in the morning between 8:00 AM and 12:00 PM.
Hemodynamic assessment
After 5 minutes of rest, patients underwent ankle-brachial index (ABI) measurements according to a standard procedure 32 using Doppler ultrasound (Stereodop 448.S; Ultrasomed, Milan, Italy) with a 9.3 MHz transducer and a standard blood pressure cuff. The leg with the lowest ABI value was considered the worse leg. The vessels were considered “not compressible” for ABI measurements >1.31 or for a procedure that had been interrupted due to painful symptoms at a cuff pressure of 300 mmHg with a Doppler signal still present.
Functional measurements
An incremental treadmill test based on level walking 34 was performed by each patient. Participants were familiarized with the motorized treadmill (Technogym RunRace, Cesena, Italy) by walking on it at a low speed for 1 minute. Use of the handrail to maintain balance was permitted. The testing procedure was explained to the patients who were asked to immediately report the onset, intensity, and location of symptoms. After the warm-up, the test started at a speed of 1.5 km/h, which was progressively increased by 0.1 km/h every 10 m. The pain threshold speed (PTS), as reported by the patient, was noted. The test finished when the patient was unable to maintain the walking speed imposed for any reason (fatigue, dyspnea, and claudication); this walking speed was recorded as the maximal walking speed (Smax).
After a 10-minute resting period, the 6-minute walking test was performed according to the published standard. 35 Patients were instructed to walk back and forth along a 22 m corridor alone at their own pace with the aim of covering as much distance as possible in 6 minutes. The total distance walked (6-minute walking distance, 6MWD) and pain-free walking distance (PFWD) were recorded.
Exercise program
The Ti-To structured, home-based exercise program 24 was prescribed to all patients. The Ti-To program encompasses a center-based phase and home-based phase with walking exercises. The first phase included circa-monthly visits at the hospital for clinical assessment, ABI and PTS/PFWD measurements, an updated prescription of the home-based walking program, and evaluation of patient adherence to the program. The home-based phase included the execution of exercise at home, preferably indoors (e.g., hallway or heated room). The program was based on two 10-minute walking sessions per day (6 days/week) of intermittent walking (1-minute work and 1-minute seated rest) at a prescribed speed. The training speed was converted into walking cadence (steps/minute) to be maintained at home by a metronome by patients who were specifically educated to walk in rhythm with it. The exercise program was increased weekly from 60 to 84–100 steps per minute according to the severity of claudication at baseline. Progressively, the length of each bout was amplified with a work:rest ratio from 1:1 to 2:1 and 3:1, while the entire duration of each session remained constant. Patients were also asked to fill out a daily training log, indicating completion of the exercise, which was certified by a caregiver when possible. The exercise program ended when the patients reached a PFWD normal for their sex and age or when no more improvements in functional parameters were registered in two consecutive tests. Additional details on the exercise program are reported elsewhere. 24,25
Evaluation of patient adherence
At discharge, rehabilitation team members evaluated the training diaries of each patient to determine the adherence score. 25 The arbitrary score ranged from 1 (lowest adherence) to 4 (highest) and was calculated by summing the percentages of certified exercise sessions completed (≥75% = 3 points; ≥50% and <75% = 2 points; ≥25% and <50% = 1 point; and <25% = 0 point) and with respect to the prescribed training speed (yes = 1 point; no = 0 point).
At discharge, the total duration of the program and number of hospital visits were also recorded.
Study group definition and bias management
The whole population at baseline was divided by sex into WomenPAD (WPAD) and MenPAD (MPAD).
Several potential biases in the interpretation of the study results were foreseeable and mainly related to significant changes in patient clinical status. Nonetheless, considering the hemodynamic and functional outcome measures examined, the main confounding issue was endovascular or surgical lower limb revascularization procedures that have a potential impact on study outcomes. Therefore, all patients who underwent a revascularization procedure during the exercise program were excluded from this analysis.
Sample size calculation
Based on the starting hypothesis, we calculated the power for an equivalence trial. Sample size calculations indicated that 264 participants were required to be 95% certain that the 90% confidence interval (CI) excluded a difference in the change in PFWD greater than the equivalence limit of 20 m, corresponding to the minimal clinically important difference established in this population. 36
Statistical analysis
Data are expressed as mean ± standard deviation, or median and 95% CIs (according to the data distribution), or as the percentage frequency (categorical data). Comparisons between WPAD and MPAD patients were made by independent t-test (normally distributed data), the Mann–Whitney test (nonnormally distributed data), or the chi-squared test (categorical data), as appropriate.
Within-group comparisons were performed by paired t-test (normally distributed data) or Wilcoxon rank test (nonnormally distributed data), as appropriate. The between-group comparison was performed with one-way analysis of variance. Within- and between-group differences are expressed as mean changes and 95% CIs.
A propensity score model was estimated using the 23 variables described in Table 1. To estimate the propensity score, we used a logistic regression model in which gender (MPAD vs. WPAD) was regressed on the baseline characteristics listed in Table 1. Patients were then pooled and sorted in ascending order according to their propensity score. The selection process began from the cases with the lowest score. If patients were MPAD and WPAD, both were selected as a matched pair according to 1:1, 2:2, 3:3, or 4:4 blocks. A patient who did not have a suitable match within the acceptable rank range was excluded.
Baseline Characteristics of the Patients Included in the Study
Statistically significant values have been indicated in bold.
ABI, ankle-brachial index; CVD, cardiovascular disease; PFWD, pain-free walking distance; PTS, pain threshold speed; Smax, maximal speed.
Statistical analyses were performed with MedCalc Statistical Software version 18.5 (MedCalc Software bvba, Ostend, Belgium).
Results
A total of 1164 PAD patients were considered eligible; 153 were not included in the final analysis because they did not complete the rehabilitation program or because of biases potentially affecting data interpretation. The reasons for exclusion are reported in Figure 1. Within the excluded sample of patients, the same proportions of WPAD and MPAD were maintained (WPAD n = 40). Thus, the final study population comprised 1011 PAD patients divided into 264 WPAD and 747 MPAD.
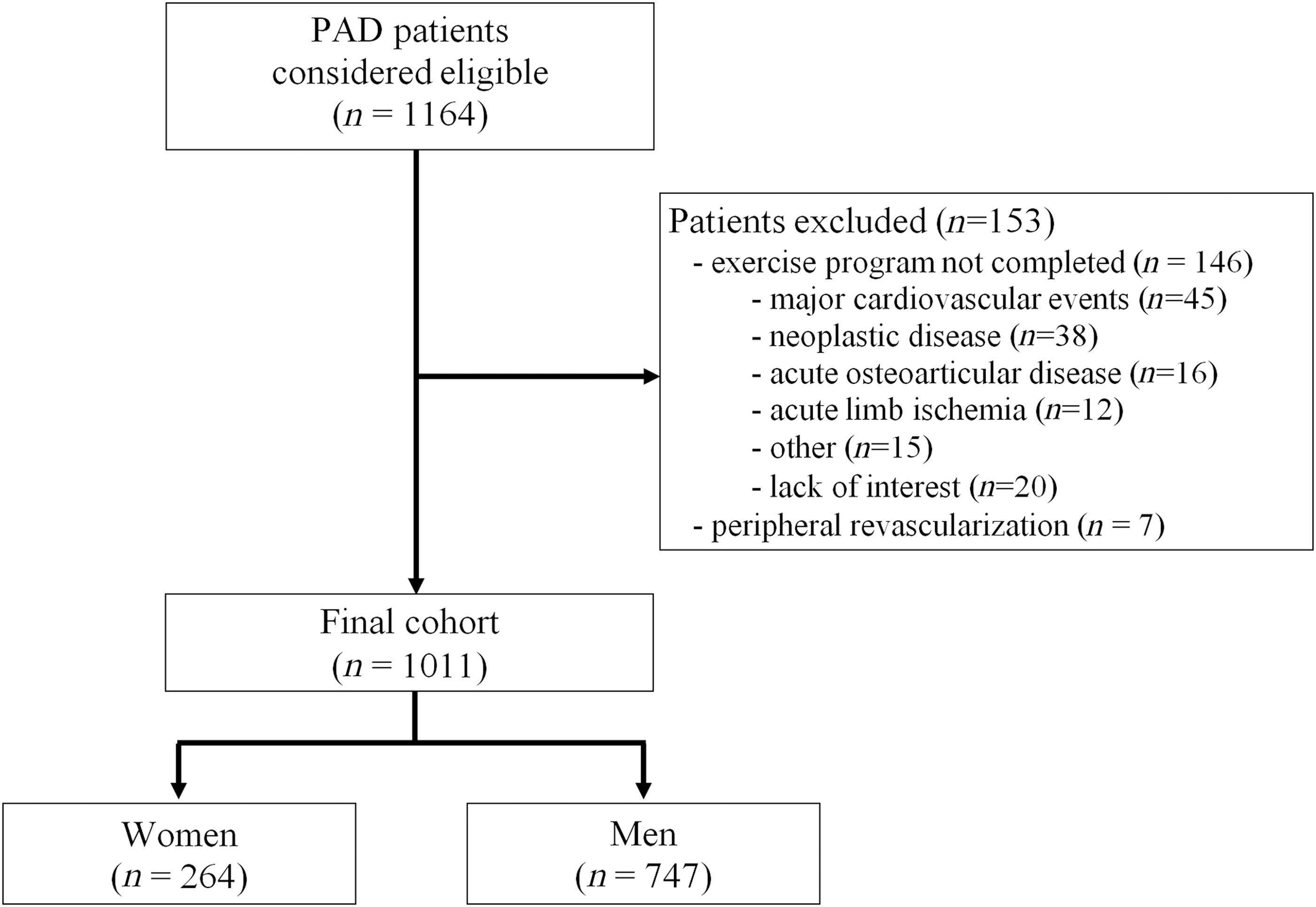
Study flow diagram.
Baseline group comparison
At baseline, the two groups did not differ in age or educational level. Considering cardiovascular risk factors, a smoking habit (93% vs. 67%; p < 0.001) and diabetes (37% vs. 30%; p = 0.049) were more prevalent among MPAD, whereas WPAD were more affected by hyperlipidemia (68% vs. 61%; p = 0.059) but not significantly. No differences were observed for hypertension and family history for CVDs.
In terms of comorbidities, MPAD presented a higher incidence of coronary heart diseases (45% vs. 28%; p < 0.001) and cerebrovascular diseases (12% vs. 7%; p = 0.007). In contrast, WPAD showed more osteoarticular (39% vs. 28%; p < 0.001) and rheumatic diseases (11% vs. 4%; p < 0.001). Despite these differences, the Charlson comorbidity index was equal in both groups (6 ± 2; p = n.s.).
Finally, both groups reported a similar duration of claudication symptoms (WPAD 5 ± 5; MPAD 6 ± 7; p = n.s.), as well as similar self-reported claudication distances (WPAD 178 ± 144 m; MPAD 205 ± 162 m; p = n.s.; Table 1).
Outcome measures at baseline
At entry, the two groups did not differ in PAD severity for the more affected limb (ABI: WPAD 0.62 ± 0.19; MPAD 0.62 ± 0.18; p = n.s.) and the less affected one (ABI: WPAD 0.83 ± 0.22; MPAD 0.85 ± 0.20; p = n.s.).
The WPAD group presented a significantly lower functional capacity in the incremental treadmill test and the 6-minute walking test. Furthermore, WPAD exhibited a lower PTS (2.3 ± 0.9 vs. 3.0 ± 1.1 km/h; p < 0.001) and Smax (2.8 ± 1.1 vs. 3.5 ± 1.1 km/h; p < 0.001), as well as a lower PFWD (132 ± 95 vs. 215 ± 115 m; p < 0.001) and 6MWD (279 ± 73 vs. 340 ± 88 m; p < 0.001; Table 1).
Rehabilitation outcomes
Data concerning the duration, participation, and adherence to the exercise program were similar between the groups except for total rehabilitation days. These data are reported in Table 2.
Features of the Program in Terms of Duration and Adherence in the Two Groups
Statistically significant values have been indicated in bold.
Median (95% confidence interval); bmean (95% confidence interval).
Both groups showed significant improvements in hemodynamic measurements and functional capacity from baseline to the end of the program.
The WPAD group exhibited a significant improvement in the ABI in both limbs (more diseased; p < 0.001; less diseased; p = 0.001). Additionally, all exercise capacity parameters showed a significant enhancement, particularly for PTS (+40%; p < 0.001) and PFWD (+108%; p < 0.001).
Similar outcomes were observed for the MPAD group, with significant ABI variations in both limbs (p < 0.001) as well as improvements in all four functional parameters (particularly evident for PTS +35%, p < 0.001; PFWD +71%, p < 0.001). Similarly, the mean claudication onset time improved in both groups (WPAD from 166 to 253 seconds; MPAD from 207 to 298 seconds). Data are reported in Table 3.
Within- and Between-Group Differences in Rehabilitation Outcomes
Statistically significant values have been indicated in bold.
Data are expressed as mean and 95% confidence interval.
ABI, ankle-brachial index; 6MWD, 6-minute walking distance; PTS, pain threshold speed; Smax, maximal speed..
The subsequent between-group comparison showed superimposable variations, without any statistically significant difference for PTS (WPAD 0.8 ± 0.9 km/h; MPAD 0.8 ± 0.9 km/h; p = n.s.), Smax (WPAD 0.4 ± 0.8 km/h; MPAD 0.4 ± 0.7 km/h; p = n.s.), PFWD (WPAD 95 ± 100 m; MPAD 86 ± 103 m; p = n.s.), and 6MWD (WPAD 33 ± 58 m; MPAD 32 ± 65 m; p = n.s.). Similarly, no differences were observed for ABI variations in both limbs (Table 3).
Propensity score analysis
After propensity score matching, two independent groups comprising 188 patients each without baseline covariate differences were identified (Table 4). In addition, the program duration (WPAD 402 ± 245 vs. MPAD 356 ± 202 days; p = 0.07), number of visits (WPAD 7.4 ± 3.3 vs. MPAD 7.3 ± 3.3; p = 0.57), and adherence (WPAD 3.1 ± 0.8 vs. MPAD 3.2 ± 0.8; p = 0.24) were measured at the end of the program and were balanced between the groups.
Baseline Characteristics of the Patients Included in the Study After the Propensity Analysis
6MWD, 6-minute walking distance; ABI, ankle-brachial index; CVD, cardiovascular disease; PFWD, pain-free walking distance; Smax, maximal speed.
The within-group analysis in the reduced samples confirmed the significant improvements for all hemodynamic and functional parameters for both groups. The between-group comparison also showed similar variations, without any significant difference for any hemodynamic and functional parameters (Table 5).
Within- and Between-Group Differences in Rehabilitation Outcomes in the Propensity Score-Matched Groups
Statistically significant values have been indicated in bold.
Data are expressed as mean and 95% confidence interval.
6MWD, 6-minute walking distance; ABI, ankle-brachial index; PFWD, pain-free walking distance; PTS, speed at onset of claudication; Smax, maximal speed.
Discussion
In this study, compared to men, women with PAD and claudication following a structured low-intensity program obtained the same benefits in terms of reduction in walking disability as well as a similar degree of adherence. This observation was also confirmed after propensity analysis, which balanced the two groups in baseline characteristics and proved that no differences in rehabilitation outcomes existed between sexes.
To the best of our knowledge, the available literature on the response of women to rehabilitation in PAD is poor, and the present results represent a novel report. The only confirmation of previous data 10,37 is the low walking performance of women compared to that of men in absolute terms. The functional capacity at entrance to the program measured with both treadmill and ground-walking tests was lower in the female population with the same hemodynamic condition. This aspect may refer to the lower aerobic efficiency typical of the female sex or the lower biomechanical efficiency aggravated by deconditioning, possibly related to the presence of comorbidities. 37,38 In daily activities, women move at a slower rate than men and present a different ambulatory pattern. 39 However, after rehabilitation, the same degree of functional improvement, which was the main focus of our study, was observed in the two subpopulations, with an average variation in exercise capacity between 20% and 110% for patients of both sexes.
Different outcomes following rehabilitation programs in chronic pathologies were reported in women compared to men, 21 –23 with problematic issues related to interest/motivation, adherence to physical activity, or effects achieved. 18,21,22
Various reasons were hypothesized to explain these results, such as the presence of comorbidities 22,37 or the type of intervention. According to the authors, programs for the rehabilitation of cardiovascular patients should not be based on exercise alone 19,22 ; these programs may also benefit from the presence of staff members providing support. 40 In general, the necessity of sex-based claudication treatment strategies should be considered. 23
Therefore, we hypothesize that the novel results observed in the present study were derived from the rehabilitation program proposed and successfully tested in frail subjects 24 –30 where the type of exercise and organizational model could have favored equal adherence and outcomes in both sexes.
Normally, the exercise recommended for the rehabilitation of patients with chronic PAD is under supervision in specialized facilities. This exercise is based on repeated walking sessions at a level of pain that increases patient tolerance and thus improves tolerance to exercise, thereby obtaining progressively longer gradual sessions. 41 Considering the lower attitude of women toward exercise 18 and the sex difference in the perception of pain, 11 a different approach might be favorable in this subgroup, based on a progressively higher pain-free walking cadence supported by the aerobic adaptations obtained during the program at controlled speed. 42,43 In a previous study faster ambulatory cadence during a step-monitored, home-based exercise program was associated to greater walking improvements in women. 44
Walking without pain with interval breaks within each exercise session was well tolerated and often performed with pleasure. A significant improvement in physical functioning 42 and QoL was observed at discharge from the pain-free program in a sample of 90 subjects with a 50% increase in the bodily pain domain. 25
Notably, other authors reported that a low-intensity treadmill program without pain was as effective for subjects with PAD, 45 with similar benefits in women compared to men. 46
Moreover, the proposed program based on individualized, low-dose exercise with interval breaks allows the enrollment of patients with severe PAD, important comorbidities, and gait problems who are often excluded from traditional rehabilitation programs due to the exercise intensity used 41,47 ; interestingly, these patients obtain more benefits from the Ti-To program. Among barriers to physical activity, low energy levels related to the presence of diabetes, a low ABI, and a low walking capacity for leg pain have been reported. 48 Additionally, comorbidities did not influence the outcomes of the study. In the female study population, every rehabilitation outcome parameter is favorably increased with or without diabetes or osteoarticular diseases. 38
However, the program in this study aimed to overcome other barriers to exercise through its organizational model.
In recent years, home-based programs have been considered feasible and effective for improving walking ability in PAD patients, 41,49,50 and recent trials have provided support for this therapeutic option. 51,52 In the present program, the modality of exercise allows the possibility to comfortably carry out all the exercises at home without giving up the surveillance of the family or the management of the house, which are typical duties of most elderly women in our region (personal observation).
The daily low dose of exercise required for an acceptable and fixed working time, which was inserted into daily life, gives women the possibility to manage housework and grandchildren.
Moreover, compared to a supervised program that requires the need to travel daily or three times a week to facilities for exercise execution, 50 the present model calls for few visits to the hospital, with low costs and a negligible or sustainable commitment on the part of the family. Finally, the program is offered to patients without cost, which is possible because of the low organizational costs of the procedures. 25,53
As a further result, in the study we observed significant changes in the ABI value. This result, which is not usually reported following the traditional programs but confirms to previous observations, 24,25,43,53,54 was similar in the two groups.
We are aware that our study has several limitations, such as its single-center retrospective design and the lack of a control group. However, being a single-center study performed by the same operators over the entire study period represents an evident strength due to the operator-dependent limitations in the evaluation of the outcome measures.
The percentage of women was ∼26%, which is far from the values reported by some authors but is consistent with other articles and representative of the whole population sent to rehabilitation. However, an analysis that considers a different percentage has also been carried out. Finally, data analysis was not performed in a blinded fashion.
Conclusions
A moderate-intensity, pain-free rehabilitation program in PAD patients was equally effective in men and women in terms of functional and hemodynamic improvements and adherence. Of course, further confirmation by a prospective study is needed. However, the implementation of effective organizational models tailored to the female population for the setting, exercise intensity, time of execution requested, tolerability, and costs warrants further research efforts.
Footnotes
Acknowledgments
We would like to acknowledge the professional editing services of American Journal Experts. This article is supported in part by an institutional research grant from the University of Ferrara, Fondo di Ateneo per la Ricerca (Prof. Roberto Manfredini).
Author Disclosure Statement
No competing financial interests exist.