
Abstract
Many women suffering from vasomotor symptoms (VMS) are now seeking nonpharmaceutical treatments for symptom relief. Recently, S-equol, an intestinal bacterial metabolite of the soybean isoflavone daidzein has received attention for its ability to alleviate VMS and provide other important health benefits to menopausal women. S-equol is found in very few foods and only in traces. About 50% of Asians and 25% of non-Asians host the intestinal bacteria that convert daidzein into S-equol. Clinical trials that evaluated the efficacy of an S-equol-containing product found that VMS were alleviated but these trials were limited in scope and primarily involved Japanese women for whom hot flashes are a minor complaint. The only trial in the United States evaluating hot flashes found symptoms were significantly reduced by S-equol, but the study lacked a placebo group, although it did include a positive control. The daily dose of S-equol used in most trials was 10 mg, and because the half-life of S-equol is 7–10 hours, to maximize efficacy, it was taken twice daily. Subanalysis of epidemiologic studies suggests that equol producers are more likely to benefit from soyfood consumption than nonproducers with respect to both cardiovascular disease and osteoporosis, although the data are inconsistent. The limited safety data for S-equol do not suggest cause for concern, especially with regard to its effects on breast and endometrial tissue. Further studies are needed before definitive conclusions of its effectiveness for VMS can be made, but the preliminary evidence warrants clinicians discussing the potential of S-equol for the alleviation of VMS with patients.
Introduction
F
In this regard, it is notable that the soy isoflavone metabolite S-equol (which is chemically classified as an isoflavan) has received attention as a potential nonpharmaceutical candidate for the alleviation of VMS as well as for other health effects, especially relevant to menopausal women. 7 –9 Soybean isoflavones have been extensively studied for an array of health benefits since 1990 when the U.S. National Cancer Institute first expressed interest in the purported chemopreventive activity of these soybean constituents. 10 genistein, daidzein, and glycitein, and their respective glycosides (the form in which they are predominantly found in soybeans), account for approximately 50%, 40%, and 10%, respectively, of the total isoflavone content of soybeans. Of these three natural isoflavones, genistein is the most biologically active and has been studied to the greatest extent. 11
Equol is a chiral compound that can exist in two forms, R-(+)equol and S-(–)equol (simply described here as S-equol). Racemic (±)equol, a 1:1 mixture of these two isomers is also commercially available (Fig. 1). 12 Although very minor amounts are found in foods such as eggs, milk, and a fermented tofu, 13 –20 humans have been exposed to S-equol for centuries primarily because certain types of intestinal bacteria, which approximately 25% and 50%, respectively, of non-Asians and Asians host are able to synthesize this bioactive compound from daidzein found in foods. 21 –23
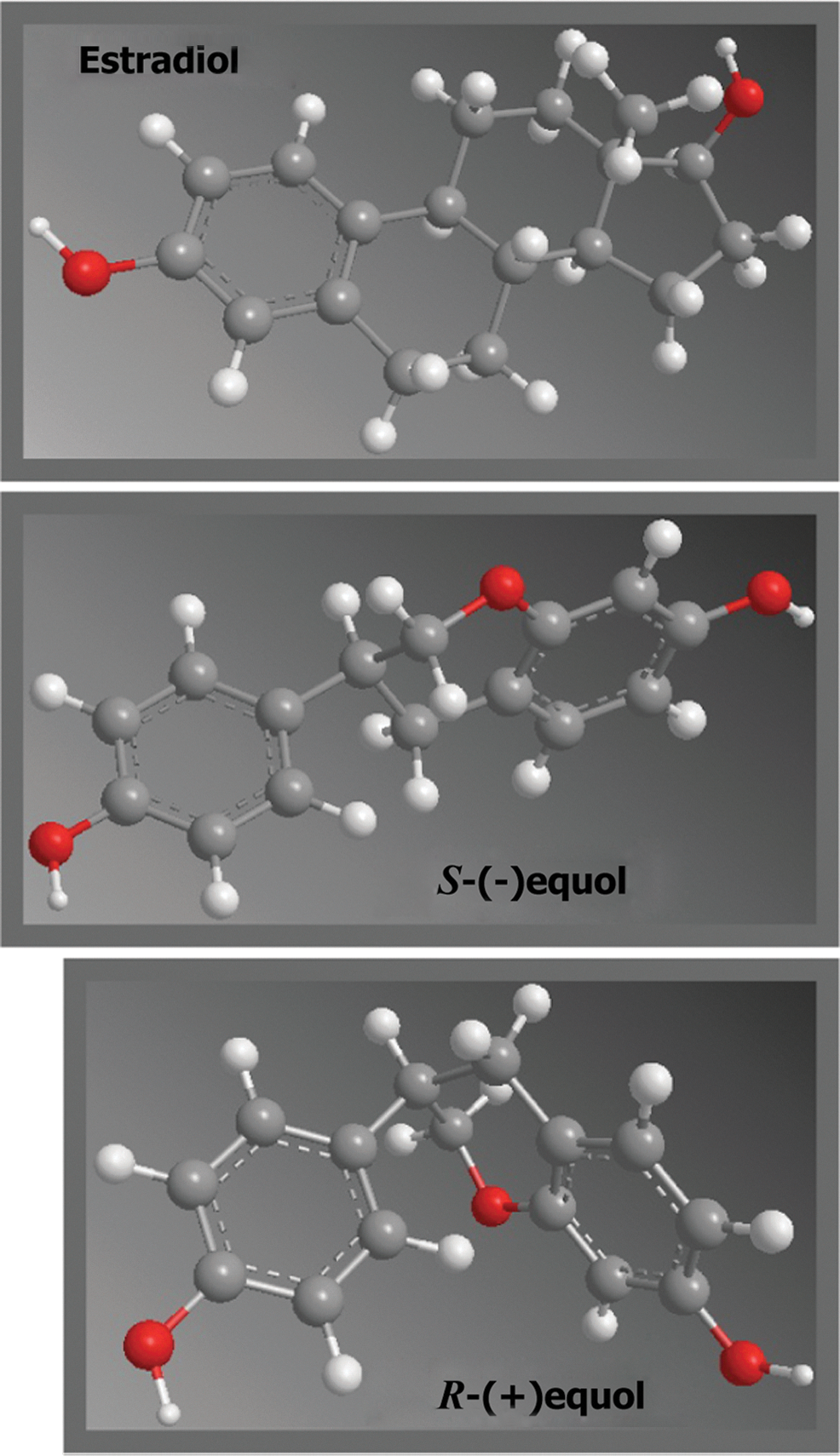
A comparison of the conformation structures of estradiol and R- and S-equol.
Although equol was first identified in mare's urine in 1932, 24 it attracted little clinical interest until the 1980s when it was identified for the first time in human urine and thought to be a new hormone. 25 In 2002, Setchell et al. 9 proposed the “equol hypothesis,” which maintained that individuals who host equol-synthesizing bacteria are more likely to benefit from the consumption of soyfoods. This hypothesis in turn raised the issue of whether the benefits associated with equol production are due to the synthesis of S-equol per se, or because the equol-synthesizing phenotype is associated with a particular health status. 26 Only within the past several years, with the advent of an S-equol-rich product, which has been made available for research purposes, has the equol hypothesis been able to be tested clinically.
In 2010, Setchell et al. 12,27 published comprehensive reviews covering the biological and pharmacokinetic properties of equol as well as providing an historical overview of research on this molecule. The intent of this brief review is to now discuss the potential for S-equol to address health issues of most relevance to postmenopausal women, with an emphasis on VMS, so that clinicians can provide informative advice to their patients about the use of this compound.
In the following described studies, an S-equol supplement was the intervention product tested and this was manufactured from soy germ, which has a high proportion of daidzein, by fermentation with an equol-producing bacteria, Lactococcus garvieae spp, by a process patented by the Otsuka Pharmaceutical Co. Ltd. in 2004 and 2006. The supplement contained a standardized amount of S-equol and there were other residual components of the soy germ and its byproducts present, none of which have known estrogenic activity. Genistein, a natural isoflavone of soy germ that has been shown to influence VMS in a meta-analysis 28 was also present but at a level (20% that of S-equol) that would be considered too low to be efficacious. While there are reports that pure S-equol is being developed as a pharmaceutical, 29 to our knowledge there have been no reported clinical trials of its effectiveness in postmenopausal women with VMS. So, in evaluating the effects of S-equol on VMS we currently have to rely on data from studies of this supplement and circumstantial data from dietary studies correlating equol-producers with nonproducers.
General Background
The estrogen-like properties of S-equol have been investigated for more than four decades, but only more recently, with the discovery of the second estrogen receptor (ERβ) in 1996, ERβ 30 has an important distinction between S-equol and endogenous estrogens been defined. Unlike estradiol, which binds with similar affinity to both ERα and ERβ, S-equol preferentially binds to the latter. 21,23 To this point, Muthyala et al. 21 reported that the S-equol concentration required to displace 50% of estradiol from ERα was 200 nM whereas a concentration of only 16 nM was required to displace estradiol from ERβ. This distinction between estradiol and S-equol is potentially important because ERα and ERβ have different tissue distributions within the body and when activated can result in different and sometimes opposite physiological effects. This appears to be the case in the breast wherein ERβ activation inhibits the proliferative effects of ERα activation, and this is considered a benefit. 31
Interestingly, although less than 5% of estradiol is present in the free (unbound) form, which is the fraction that is available for receptor occupancy, while it has been reported that about 50% of S-equol circulates in the free form, which is significantly higher (18.7%) than for its precursor daidzein. 22 Thus, the biological activity of S-equol should therefore be enhanced by both its reduced binding to serum proteins.
Pharmacokinetic studies have found that S-equol is highly bioavailable with 60%–80% of ingested S-equol absorbed. Maximum plasma S-equol concentrations occur between 1 and 3 hours after oral administration and it is cleared from plasma with a half-life of 7 to 10 hours. 23,29,32,33 Consequently, over 80% of S-equol is excreted in the urine within 24 hours after administration. 23,32,33 Based on these pharmacokinetics to achieve sustained steady-state serum concentrations, a twice-daily dose, rather than a once-daily dose of S-equol is considered optimal.
VMS/Menopausal Symptom Relief of S-equol
While only the results of clinical data allow meaningful conclusions to be made about the impact of S-equol on VMS, it is noteworthy that two observational studies are supportive of its efficacy. In one, a study of 108 Japanese peri- and postmenopausal women, 51.6% of whom were equol-producers, it was found that there was no difference in the urinary excretion of genistein and daidzein between women with high and low menopausal symptom scores, as measured by a simplified menopausal index (SMI), whereas S-equol urinary levels in women with higher SMI scores were significantly lower than in those with lower SMI scores. 34
In agreement, are the results of a U.S. population-based observational study involving 355 women (45–55 years) determined to be in the menopause transition or postmenopausal, who consumed at least three servings of soyfoods weekly and had a urinary daidzein or genistein concentration ≥100 ng/mL. 35 When compared with women in the lowest quartile of daidzein intake (mean, 4.9 mg/day), equol-producers (n=129) in the highest intake quartile (mean 28.6 mg/day) were nearly 80% more likely to report the number of VMS below the mean (odds ratio, 0.24; 95% confidence interval: 0.07, 0.83), with testing for trends across levels of daidzein intake statistically significant (p=0.06). In contrast, there was no association between daidzein intake and VMS per day among equol nonproducers. 35
Clinical Research
The first clinical trial to evaluate the effects of S-equol on VMS was a 12-week placebo-controlled pilot study involving 134 postmenopausal Japanese women, which included both equol producers and nonproducers. 36 During the intervention, women were permitted to consume up to 20 mg/d of soy isoflavones via dietary soyfood intake. In the subgroup of equol nonproducing women (n=19) taking a total of 30 mg/day S-equol (divided evenly in 3 doses) there were statistically significant decreases in the somatic subscore of the menopausal symptom score (p<0.05) as well as decreases in tension/anxiety (p<0.05), depression/dejection (p<0.05) and fatigue (p<0.01), which were included as part of the validated Profile of Mood States instrument. However, no benefits were observed among women who took a lower 10 mg/day dose of S-equol. One limitation of this study is that hot flashes were not recorded, perhaps because hot flashes are not considered a major symptom of menopause in Japanese postmenopausal women 36 (Table 1).
All S-equol intervention studies were accomplished via SE5-OH, which is a fermented soy germ including S-equol. †Analyzed number for S-equol efficacy. §Modified Climacteric Symptom Evaluation Form Checklist including daily HF frequency and severity record. ¶unrelated to treatment by PI, GCS, Green Climacteric Scale; POMS, Profile of Mood States; SMI, simplified menopause index; using a 4-point scale for complaints (0: no, 1: mild, 2: moderate, 3:severe) of 10 menopausal symptoms (facial flushing, perspiration, chilliness of the back and extremities, palpitation or shortness of breath, insomnia, irritability, depression, headache/ dizziness/ nausea, fatigue, stiff shoulder/ back pain/ pain of extremities); VAS, Visual Analog Scale; AE, adverse event; FSH, follicle-stimulating hormone; LH, luteinizing hormone; TSH, thyroid-stimulating hormone; T3, triiodothyronine; T4, thyroxine; SHBG, sex hormone-binding globulin; ECG, electrocardiogram.
Interestingly, in contrast to the lack of effect of 10 mg/day S-equol noted in the previous study, Aso 37 found in a 12-week study involving 99 Japanese non-equol-producing women that in comparison to the placebo, this dose improved menopausal symptoms, especially with regard to shoulder stiffness, a frequent complaint among Japanese menopausal women (p=0.034). 37 Again, hot flashes were not recorded although “facial flashing” score in the SMI which was recorded did not differ between any S-equol and placebo groups (Table 1).
A later study by Aso et al. 38 was the first to evaluate the effects of S-equol on hot flashes. In this 12-week trial non-equol-producing women were randomly assigned to receive placebo (n=83) or 10 mg/day S-equol (n=77) and all completed a standardized menopausal symptom checklist and rating five common menopause symptoms using a visual analog scale at baseline, and after 12 of treatment and at 18 weeks, representing 6 weeks post intervention. 38 At baseline, daily hot flash frequency (mean±standard deviation) was 3.2±2.4 and 2.9±2.1 in the placebo and S-equol groups, respectively. After the 12-week intervention, hot flash frequency decreased by 58.7% and 34.5% in S-equol and the placebo groups, respectively (difference between groups, p=0.009). After treatment was discontinued for 6 weeks there were no longer differences between groups. The severity of hot flashes (p=0.015) and neck or shoulder muscle stiffness (p=0.015) also significantly decreased in the S-equol group in comparison to the placebo. This trial is notable not only because it is the first to specifically evaluate hot flashes but also because it included a 4-week placebo run-in period during which time participants who demonstrated≥50% symptom reduction were excluded from the treatment phase (Table 1).
The only U.S. trial to evaluate S-equol was a 4-week placebo run-in phase and 8 week intervention in duration that involved 102 postmenopausal women aged 45–65 years. 39 The majority of the subjects were White (81%) and Black/African American (16%). The criteria for body mass index was less than 33 kg/m2 and ∼26 kg/m2 in average. Finally, 28% of equol producers were included in the subject population. This trial included four groups, three of which were given different amounts of S-equol, whereas the fourth group served as a positive control. More specifically, women in the positive control group consumed 50 mg/day soy isoflavones (expressed as aglycone equivalents) containing approximately equal amounts of genistein and daidzein, and the other three groups were administered 10, 20, or 40 mg/d S-equol.
The dose of isoflavones used in this study was recently shown in a meta-analysis by Taku et al. 28 to alleviate hot flashes provided it contained sufficient amounts of genistein (∼19 mg/day). Each subject was provided with a standardized VMS diary card on which they recorded daily VMS experienced the previous night and that day. Hot flashes were rated as mild, moderate, or severe recorded as a score 1, 2, or 3 respectively. The baseline averages of daily hot flashes frequency and severity score in the entire study population were ∼10 times per day (range 5–20 times per day) and ∼2.2, respectively with similar values between the groups. Reported reductions in hot flash frequency were similar in all treatment groups, but the cumulative effect analyses revealed that women taking 40 mg/day S-equol experienced a greater reduction in hot flash frequency than those consuming isoflavones (p=0.021) and the effect of the 20 mg/day S-equol approached superiority (p=0.076). Also, subanalysis found that among participants who reported having>8 hot flashes per day at baseline, both the 20 and 40 mg/day dose of S-equol reduced hot flash frequency more than isoflavones (p=0.045 and p=0.001, respectively) while the effect of 10 mg/day S-equol approached superiority at p=0.063. The percent of responders at week 8 (i.e., ≥50% reduction in hot flash frequency) in 40 mg/d S-equol was more than twice that in isoflavones (43% vs. 16%, p=0.056) and 27% and 25% in 20 and 10 mg/d, respectively. The hot flash severity was not significantly different among the doses or isoflavone groups. In addition, both the 10 and 20 mg/day doses of S-equol improved muscle and joint pain scores significantly more than isoflavone group (p=0.003 and p=0.005, respectively). However, despite the robust results, a major limitation of this study was the lack of a placebo control group. 39 In any of the subscale scores of the Green Climacteric Scale, there were no significant differences between the S-equol doses and the isoflavone group in the change from baseline to 8 weeks (Table 1).
In addition to the above trials, clinical studies have indirectly evaluated the effects of S-equol on VMS by providing isoflavones to study participants and determining whether the response differed according to equol-producing status. For example, in one 6-month study, 96 women were randomized to receive a placebo or soygerm that provided 135 mg/day isoflavones. 40 The severity of menopausal symptoms was quantified using a 17-item modified Kupperman Index. In equol-producers, the scores for hot flashes and excessive sweating were significantly reduced (p<0.05) after 3 months, and the scores for hot flashes, weakness, palpitations, limb paresthesia, and total symptoms after 6 months, compared with the placebo group. However, there were no significant differences in any scores between nonproducers and placebo.
Additional support for the importance of S-equol production comes from a subanalysis of a small scale pilot study (n=130) in which peri-and post-menopausal women aged 40 to 69 years were randomized into one of three groups—placebo, 100 mg/day, 200 mg/day isoflavones—crossed with three dosing frequencies (once, twice, and three times daily). 41 For both daytime and nighttime hot flash intensities, equol producers had consistently greater declines than nonproducers in women randomized to the 100 or 200 mg/day isoflavone groups, although these differences between producers and nonproducers did not achieve statistical significance.
Finally, results from a 6-month Chinese study from Hong Kong involving 270 postmenopausal equol-producing women who were divided into three groups: (1) 40 g/day soy flour, (2) 40 g/day low-fat milk powder+63 mg of daidzein and (3) 40 g/day low-fat milk powder (placebo group) 42 found no differences in any of the menopausal symptoms assessed by a validated and structured symptom checklist among the groups.
Beyond VMS
There are a number of clinical investigations in Japanese individuals, albeit limited, of the effects of S-equol on cardiovascular disease and bone and skin health. For example, a 12-week study of 54 overweight or obese Japanese women and men, 74.1% of whom had metabolic syndrome 43 compared S-equol (10 mg/day) to placebo and found a significantly lower hemoglobin A1c (–0.2%±0.1 versus 0.1%±0.1 for placebo; p<0.05), serum low-density-lipoprotein cholesterol (–0.2 mmol/L±0.1 versus 0.1 mmol/L 0.1; p<0.01) and cardio-ankle vascular index scores (–0.2±0.1 versus 0.1±0.1 for placebo; P<0.01), which is an indicator of arterial stiffness, in S-equol treated patients. Importantly, these effects were more prominent in female equol nonproducers than female equol producers and males.
A 12-month bone study involving 93 Japanese, postmenopausal women randomized to receive a placebo or 2, 6, or 10 mg/day S-equol. In comparison to the placebo, at study termination, urinary deoxypyridinoline was significantly decreased (−23.94% vs. −2.87, p=0.020) in the 10 mg/day S-equol group. In addition, treatment with 10 mg/day also prevented a decrease in bone mineral density in the entire body that was noted in the placebo group. 44
Finally, there is sufficient basis for speculation about the potential for S-equol to favorably impact skin health 45 since it is well recognized that ERβ is abundantly expressed in skin, and estrogen therapy is known to improve several skin parameters. 46 However, only limited data on S-equol in this regard are available. The only published trial to date was of 12 weeks duration and it evaluated the effects S-equol on skin aging as measured by crow's-feet wrinkles in non-equol-producing postmenopausal Japanese women. 47 In comparison to the placebo group (n=34) there was a statistically significant decrease (p<0.05) in wrinkle area in the women taking 10 mg/d (n=34) or 30 mg/d S-equol (n=33). There was also a significant difference in wrinkle depth between the placebo group and the 30 mg/day group (p<0.05) and other skin parameters were not significantly affected.
Safety
Although S-equol occurs only in minor amounts in a few foods, 13 –20 exposure to this isoflavone metabolite has occurred in many people through its normal intestinal synthesis following the consumption of traditional isoflavone-rich soyfoods, which have been an important part of Asian diet for centuries. Despite this long historical exposure, concerns have been expressed about the possible adverse effects of S-equol because it has affinity for the estrogen receptor. These concerns have, not surprisingly, focused primarily on estrogen-sensitive tissues, especially the breast. Although S-equol is chemically and physiologically different from soybean isoflavones and estradiol, there continues to be controversy about whether isoflavone exposure poses a risk for breast cancer or could be harmful to patients with breast cancer. 48 Clinical research published over the past 10 years now shows isoflavone exposure does not adversely affect markers of breast cancer risk, including mammographic density and breast cell proliferation. 49 Furthermore, prospective epidemiologic data, which includes over 11,000 breast cancer patients, now indicate that a soy diet containing isoflavones actually reduces the risk of recurrence and improves survival in patients with breast cancer. 50
It is also worth mentioning that while genistein stimulated the growth of a human breast cancer cell line that was transfected into the athymic mouse model of breast cancer, 51,52 findings that led to the concerns about the risk of soy and isoflavones to women with breast cancer, the same researchers later showed that S-equol in the same model had no effect on the growth of the very same tumors. 53 These findings are encouraging for the safety of S-equol.
Two U.S. studies, one involving women of Chinese ethnicity, found that equol production was associated with lower breast tissue density. 54,55 Breast tissue density is viewed as a marker of breast cancer risk. Finally, in the above mentioned skin study, mammography classification at before and after the study indicated that no subject had either category 4, suspicious abnormality, or 5, highly suggestive of malignancy, and most of them (>90%) showed category 1, negative, at 12 weeks. It was concluded that no subject had an abnormal image on mammography 47 (Table 1).
Since estrogen therapy increases endometrial cancer risk, the effects of S-equol on the uterus should be addressed. Two studies found no evidence for S-equol having a proliferative effect on the uterus. Both of these 12-week studies involved Japanese postmenopausal women, and specifically examined endometrial thickness. A study of 99 women who were randomized to receive a placebo or 2, 6, or 10 mg/day S-equol. 37 The endometrial thickness before and after interventions were, respectively, 3.9 and 3.6 mm for the placebo group, 4.1 and 4.0 mm for 2 mg/day treatment group, 3.9 and 3.8 mm in 6 mg/day treatment group, and 4.0 to 4.6 mm in 10 mg/day treatment group. None of these changes were significant (date not shown). In a second similar study of 101 women who were randomized to the placebo or to 10 or 30 mg/d S-equol, 47 the values for endometrial thickness at baseline and after 12 weeks of treatment, resepctively, were 0.1 and 0.0 mm in the placebo group, 0.2 and 0.4 mm in 10 mg S-equol group, and 0.2 and 0.1 mm in 30 mg S-equol group. Again, no significant differences were observed (Table 1).
Finally, vaginal cytology examined the degree of abnormal cells and placed them in five classes based on the Papanicolaou classification system. The baseline classifications of virginal cytology in all subjects were either class 1, absence of atypical or abnormal cells, or class 2, atypical cytology but no evidence of malignancy. At the end of the 12 weeks of intervention, no subject demonstrated an increase to class 3 cells 47 (Table 1).
Studies investigating the effect of S-equol on breast and endometrial/vaginal health addressed in this article are clearly limited and mostly of small sample sizes and short durations. What is needed are longer-term studies to evaluate the effects of S-equol on mammographic breast density and endometrial thickness. Nevertheless, epidemiological data of soy isoflavones lend indirect support for the safety of S-equol, since 25%–30% of Westerners and 50%–60% of Asians or Western vegetarians naturally produce S-equol when consuming soy foods. 12
Summary and Conclusions
The evidence, while limited, suggests that S-equol may present a viable nonhormonal agent for the alleviation of VMS. Future placebo-controlled trials will better enable the strength of these data from small trials of S-equol on VMS in Western women to be better evaluated. A secondary analysis of a trial involving U.S. women found that S-equol was more efficacious than isoflavones, which were used as the positive control for VMS. All of the published clinical intervention trials have used an S-equol-containing supplement, which contains multiple other potentially active components. Only after future studies with pure S-equol will it be possible to determine the exact role of S-equol on VMS. Nevertheless, the current data are tantalizing enough to suggest that there may for some women be benefits from considering the use of S-equol in menopause, not only for it potential for alleviating VMS but also because of possible other unrelated benefits, such as skin health. Given the apparent safety of S-equol it is reasonable for clinicians to discuss with their patients the use of S-equol as a treatment option for VMS, especially for those women not wanting to use pharmaceuticals.
Footnotes
Acknowledgment
We gratefully acknowledge Dr. Cynthia Stuenkel for providing useful advice.
Author Disclosure Statement
WU, KS, and MJ are members of the Menopausal Health Advisory Board of Pharmavite, LLC, (Northridge, CA). KS holds intellectual property in the form of inventorship on several patents related to S-(–)equol that are licensed by Cincinnati Children's Hospital Medical Center.