
Abstract
Many basic, mechanistic studies of how sex steroids alter vascular function proceeded from Dr. Bush's seminal epidemiologic observations that noncontraceptive use of estrogen reduced all-cause and cardiovascular mortality. However, translating findings from these basic science studies into clinical trials and clinical guidelines has been controversial. This commentary reviews the development of sex steroid vascular research, identifies mechanisms by which sex steroids affect vascular function, reviews findings from recent clinical hormone trials, and identifies challenges and the need for continued funding of such investigations.
Introduction
D
Historical Developments
Dr. Bush's initial evaluations of the relationship between noncontraceptive hormone use and all-cause mortality were published as preliminary results of the Lipid Research Clinics Program Follow-up Study 2 about the same time as the Nobel Prize–winning discovery by Robert F. Furchgott of the vasomotor regulatory role of the endothelium by endothelium-derived relaxing factor (EDRF), 4 which was subsequently identified to be nitric oxide. 5 These publications opened the possibility that some of the nonreproductive actions of sex steroids could be mediated through actions on the vascular endothelium.
One of the first attempts to address this question involved intramuscular estrogen treatment to ovariectomized rabbits. After 4 days, the femoral arteries were removed for evaluation of endothelium-dependent relaxations. A modest but significantly greater endothelium-dependent relaxation was observed in arteries derived from treated compared to untreated animals, providing proof of concept that estrogen could modulate vascular responses through the endothelium. 6 In addition to estrogenic modulation of the blood lipid profile, 7 these endothelium-dependent relaxations mediated through increased production and release of nitric oxide could contribute, in part, to reduced development of atherosclerosis in nonhuman primates 8 –10 and, perhaps, reduced cardiovascular mortality in humans using noncontraceptive estrogen products. 7
In the late 1980s into the early 1990s, political attention in the United States began to focus on women's health and inclusion, or lack thereof, of women in clinical trials. The National Institutes of Health (NIH) instituted a panel (1987), and congressional hearings were held (1990) on inclusion of women in clinical studies, resulting in the NIH Revitalization Act of 1993. Shortly thereafter, under the leadership of Dr. Bernadine Healy, the first woman director of NIH, two initiatives began that continue to influence research on cardiovascular effects of sex steroids hormones. One, the Women's Health Initiative (WHI, 1991), consisted of a prospective randomized clinical trial and an observational study to address the most common causes of death and disability (cardiovascular disease, cancer, and osteoporosis) in postmenopausal women. 11 The second was a request for application (RFA HL-93-05-H, 1992), “Effects of Sex Hormones on Coronary Artery Reactivity,” the goal of which was to develop insights into therapeutic approaches for reducing the higher incidence of coronary disease in men and postmenopausal women than in premenopausal women. As a result of that RFA, a plethora of investigators in the basic sciences focused their research efforts toward understanding the cellular mechanisms of actions of sex steroids. An explosion of discoveries followed, including identification of types of steroid receptors, definition of genomic and nongenomic actions of sex steroids, development of animals with modified steroid receptors, definition of intracellular mechanisms of action of the sex steroids (e.g., regulation of ion channels and posttranslational modification of enzyme, to name a few), pharmacologic development of selective estrogen receptor modulators, and studies of integrated actions of sex steroids in humans (for review, see 12 ). These discoveries paralleled enrollment and conduct of the WHI; thus, design of the WHI did not have the benefit of these discoveries from the basic sciences. 13
Sex Steroids and Vascular Function
Receptors for the sex steroids are expressed in the brain, heart, kidneys, vascular endothelium, and smooth muscle of females and males. Therefore, investigations of how the sex steroids modulate cardiovascular function in health and disease require an integrated approach.
Although most studies regarding effects of sex steroids have focused on the endothelium, vascular smooth muscle, and cardiomyocytes (see 12,14,15 ), it is important to remember that control of peripheral vascular tone reflects interaction of two regulatory systems: (1) the autonomic nervous system, representing a central command center signaled by chemo- and baroreceptors, and (2) the vascular endothelium, signaling changes in mechanical and chemical changes in the local environment. Most of what is known about regulation of peripheral vascular tone has been derived from studies performed on men and male animals. However, sex steroids regulate synthesis, uptake, and degradation of adrenergic transmitter (Fig. 1), as well as expression of receptors for adrenergic agonists. Thus, autonomic regulatory function will reflect, in part, the hormonal status of the individual. For example, total peripheral resistance is positively associated with muscle sympathetic nerve activity in young men but not in young women. However, a linear and positive relationship for total peripheral resistance and muscle sympathetic nerve activity is observed in young women following blockade of beta (β) adrenergic receptors, suggesting that perhaps hormonal (estrogen) status affects sensitivity or expression of these receptors. Supporting this conclusion, a positive relationship between total peripheral resistance and muscle sympathetic nerve activity is observed in postmenopausal women, and β adrenergic receptor blockade does not alter this relationship. 16 These results open the area for further investigation into how sex and hormonal status interact in development and expression of vascular pathologies having a female prevalence and autonomic component including “hot flashes” of menopause, Raynaud's disease, postural orthostatic tachycardia syndrome (POTS), microvascular angina, and migraine. Etiology of heart failure with preserved ejection fraction (HFpEF) may also have an autonomic component, given that this condition also has a female prevalence, with hypertension and atrial fibrillation being more commonly associated with this condition than myocardial ischemia. 17 In addition, the female-specific condition of hypertensive pregnancy disorders may reflect an underlying pathology, which then increases a woman's lifelong risk for developing cardiovascular disease. 18

Schematic of potential influence of sex and estrogen on synthesis and disposition of norepinephrine from the peripheral adrenergic nerve terminal. Estrogen may modulate synthesis of norepinephrine in the nerve terminal, uptake of transmitter into the nerve terminal and vascular smooth muscle, expression and sensitivity of beta-adrenergic receptors, and degradation of norepinephrine. Estrogen and metabolites also increase uptake of norepinephrine into the terminal but decrease degradation through inhibition of COMT. COMT, catechol-o-methyltransferase; DOPA, dihydroxyphenylalanine; NE, norepinephrine; NME, normetanephrine; +, activation; −, inhibition; X, transporter.
There is ongoing interest in discovery of “biomarkers” for evaluating risk, diagnosis, and prognosis of cardiovascular disease. Most studies have focused on soluble blood-borne factors (e.g., lipids, C-reactive protein, and other so-called inflammatory cytokines, such as the interleukins 19,20 ). However, sex steroids will regulate gene transcription and translation in cells of the vascular compartment, including platelets and leukocytes, which interact with each other and the vascular endothelium throughout development of vascular pathologies (Fig. 2). 21,22 Activated platelets, leukocytes, and endothelium release bioactive membrane-bound vesicles, which are <1 microns in diameter, called microvesicles. These microvesicles carry proteins defining their cellular origin (i.e., as proteins specific for platelets, leukocytes, and endothelial cells). 23 Thus, changes in relative proportions of microvesicles may provide information regarding cell-specific activation or the interaction of those cells with each other (platelet-leukocyte interactions, platelets and leukocytes interacting with the endothelium) during various pathologic processes. For example, numbers of endothelium-derived microvesicles are higher in the blood of recently menopausal women who had clinically significant coronary arterial calcification (Agatston score >50) compared to recently menopausal women who had no arterial calcification. 24 In addition, numbers of circulating microvesicles positive for tissue factor (TF) vary with estrogen status, 23 perhaps reflecting early stages of disease. These investigations into populations of microvesicles relative to hormonal status and cardiovascular risk represent exciting areas of ongoing research. However, specific populations of microvesicles need definition in apparently healthy persons across the life span in order to establish normative ranges before they can be used as markers for diagnosis and prognosis of disease.

Schematic of hormonal modulation of platelet activity. Estrogen and other sex steroids bind to their specific receptors in the megakaryocytes, the precursors of platelets, modulating gene transcription and thus the enzymes and secretory proteins carried by the platelets in the circulation. As platelets turn over about every 12 days, the characteristics of the circulating platelet pool will vary, depending upon the hormonal status (i.e., changes at puberty, pregnancy, and menopause). In addition to secretion of mitogenic and vasoactive factors, activated platelets provide a surface for the generation of thrombin and release membrane-bound microvesicles, which can exchange bioactive materials with other cells, including leukocytes and the vascular endothelium, resulting in vascular remodeling leading to changes in blood flow or microvascular permeability and damage to the end organ.
In addition to contributing to and reflecting ongoing vascular pathology in peripheral conduit arteries, microvesicles may contribute to microvascular alterations leading to end-organ damage. For example, in recently postmenopausal women, numbers of platelet-derived and prothrombogenic microvesicles correlated with increases in white-matter hyperintensities in the brain. White-matter hyperintensities are structural changes that precede cognitive decline. 25 Areas of current investigation are whether and how noncontraceptive use of sex steroids affects specific populations of microvesicles and how they might be related to progression of vascular-wall thickening, coronary arterial calcification, or microvascular disease.
Because a woman's cardiovascular system adapts to changing circulatory demands of pregnancy, it should be expected that there will be sex differences in cardiovascular regulatory mechanisms, and these sex differences require further in-depth investigation. Furthermore, many studies investigating actions of sex steroids have been designed to examine testosterone in males and estrogen in females. However, aromatization of testosterone to estrogen in males has cardiovascular consequences, 26 –31 and cardiovascular effects of testosterone and its aromatization in women have not been studied systematically. Additional investigation into mechanisms of action for both of these hormones in both sexes is needed, as hormonal supplementation continues to be used clinically.
Menopausal Hormones: Treatment vs. Prevention
Several observational, case-controlled, and epidemiological studies published about the same time as those of Dr. Bush also reported reduced risk of cardiac events and death in menopausal women using hormone products. 32 –36 Collectively, these studies included over 90,000 women from three countries with ages ranging from 35 to 79 years, with follow-up ranging from 2 to 16 years of hormone use. Because these studies were not randomized controlled trials, conclusions that menopausal hormone treatment reduced cardiovascular risk or prevented cardiovascular mortality were criticized as reflecting healthy-user bias, as women included in those studies most likely actively sought treatment to reduce menopausal symptoms. Thus, the WHI was designed to provide evidence from a randomized controlled prospective trial of whether menopausal hormone treatment reduced risk of cardiovascular disease.
The formulation of hormones selected for use in the WHI was based on that most frequently reported in the Nurses' Health Study (conjugated equine estrogen [CEE]; 0.625 mg/day) with medroxyprogesterone acetate (MPA, 2.5 mg/day) for women with a uterus and CEE alone for women without a uterus. Because outcomes for the WHI were cardiovascular events, enrollees were older (average age was 63 years) to ensure adequate event rate. At enrollment, cardiovascular health was by self-report; in order to blind investigators as to treatment assignment, most women did not have menopausal symptoms at the time of randomization. 11 Thus, women in the WHI were dissimilar from those of observational studies. Perhaps not surprisingly, results of the WHI were opposed to those of previous studies in that women randomized to CEE plus MPA showed increased risk for adverse cardiovascular events. 37 However, subsequent analysis, which stratified women in the WHI by age and time past menopause, suggested a reduction in adverse events in the CEE-plus-MPA group if women were within 10 years of menopause. 38 In women randomized to CEE alone, coronary calcification was lower when evaluated 1 year following cessation of treatment for 7 years. 39 In another analysis of WHI data, women who met criteria for metabolic syndrome at the time of randomization also had increased risk for adverse events if randomized to treatment. 40 Collectively, results from these subanalyses of the WHI begin to define a group of women who might be more representative of those defined as “healthy users” who initiate hormonal use in the perimenopausal or early postmenopausal period and who would benefit from treatment.
The Danish Osteoporosis Prevention Study (DOPS), which also began about the same time as the WHI, randomized women to menopausal hormone treatments such that the inclusion criteria more closely represented women who would be prescribed hormone treatments in clinical practice, that is, women ranging from 45 to 58 years of age and who were within 3–24 months of menopause. 41 Women with a uterus were randomized (open label) to 2 mg oral synthetic 17β-estradiol for 12 days, 2 mg 17β-estradiol plus 1 mg norethisterone acetate for 10 days, and1 mg 17β-estradiol for 6 days. Although the main outcomes of the study were bone health and fracture, after 10 years of treatment and an additional 6 years of follow-up, women randomized to treatment had significant reduction in mortality, heart failure, and myocardial infarction without increases in cancer or stroke. 42
A study that evaluated progression of vascular disease in healthy postmenopausal women rather than disease endpoints was the Estrogen in the Prevention of Atherosclerosis Trial (EPAT). EPAT was a randomized, double-blind, placebo-controlled trial designed to test whether unopposed oral micronized 17β-estradiol (1 mg/day) reduced progression of subclinical atherosclerosis defined by changes in carotid intima medial thickening measured by ultrasound. 43 This study enrolled women about the same age as those in the WHI (mean 62, range 46–80 years) with low-density lipoprotein cholesterol levels of 3.37 mmol/L or greater (>130mg/dL). Women were excluded if they reported hot flashes or were current smokers. After 2 years, the rate of progression of carotid intima medial thickening was significantly less in women who were randomized to treatment and not taking lipid-lowering medication compared to women randomized to placebo but not different from women assigned to placebo who were taking lipid-lowering medication. 43 Thus, the vascular benefit from estrogen treatment was probably associated with changes in blood lipid profile.
Building on elements of the WHI and EPAT studies, the Kronos Early Estrogen Prevention Study (KEEPS), which began in 2005, was a randomized, double-blinded, placebo-controlled clinical trial designed to test the hypothesis that initiation of hormone treatment near to menopause (within 1.2±0.6 years from women's last menses; 52.7±2.6 years of age) would slow atherosclerotic processes defined by changes in carotid intima medial thickness and coronary arterial calcification in healthy women. Inclusion criteria for KEEPS were rigorous, thus biasing the study toward individuals at low risk for cardiovascular disease (“healthy users”) based on conventional cardiovascular risk factors, including, unlike the EPAT study, low-density lipoprotein cholesterol levels <190 mg/dL and the absence of clinically significant coronary arterial calcification (Agatston score<50). 44 As clinical prescribing practices for noncontraceptive use of hormones (menopausal hormone therapy [MHT]) changed following the WHI, lower doses of CEE were used in KEEPS. In addition, as transdermal and oral products might differentially affect risk for thrombosis, 45,46 women in KEEPS were randomized to either oral CEE (0.45 mg/day), transdermal 17β-estradiol (50 μg/day), both with oral progesterone (200 mg/day for the first 12 days of month), or placebo pills and patch for 4 years.
After 4 years of treatment, there were no significant differences in either carotid intima medial thickness or coronary arterial calcification. Changes in conventional cardiovascular risk factors included increases in high-density lipoprotein cholesterol, triglycerides, sex hormone binding globulin, and high-sensitivity C-reactive protein with concomitant decreases in low-density lipoprotein cholesterol in the CEE group compared to either the transdermal 17β-estradiol or placebo groups. 47 Only total cholesterol and insulin resistance decreased in the transdermal group compared to the other two groups. 47 In addition to changes in blood parameters, bone mineral density was maintained, 48 and vasomotor symptoms were reduced in the treated groups compared to the placebo group. 47
There are several possible reasons why outcomes of these studies differed. First, KEEPS enrolled women with an average age about 10 years younger than in either WHI or EPAT and who were at low risk for cardiovascular disease. Second, the duration of KEEPS may have been insufficient relative to the natural progression of disease in this age group, 49 although the EPAT study did observe differences among treatment groups after just 2 years. Changes in lipid profile, as well as more subtle change in platelet functions, 50 could possibly contribute to different progression of disease with longer use, as might be suggested from the cardiovascular outcomes of DOPS. Indeed, although most women in KEEPS did not accumulate calcium in the coronary arteries, there was a trend for fewer women to do so if randomized to active treatments compared to placebo (21%, 18.9%, and 17.4% in the placebo, transdermal, and oral groups, respectively). 47 In the WHI, there was less accumulation of coronary arterial calcium in women randomized to CEE only, which was significant after 8 years of follow-up.
Finally, the formulations and doses of hormones, while sufficient to maintain bone-mineral density and reduce hot flashes, may have been too low to affect the threshold for vascular processes, including those mediated by the vascular endothelium 43,51 –55 (Table 1). Although serum levels of 17β-estradiol, estrone, and their sulfonated products in the treated groups differed from the placebo group (Fig. 3), levels of 17β-estradiol in the oral CEE were significantly less than in the transdermal group and did not exceed those levels used to define menopause for inclusion into KEEPS. The dose of transdermal 17β-estradiol used in KEEPS is considered comparable to the 0.625 mg/day dose of CEE used in the WHI.

Serum levels of 17β-estradiol, estrone, and their sulfonated products in a subset of women participating in KEEPS at Mayo Clinic. Data are shown as mean±SD. KEEPS, Kronos Early Estrogen Prevention Study; PL, placebo; oCEE (n=27), oral conjugated equine estrogen (0.45 mg/day, n=20), tE2, transdermal 17β-estradiol (50 μ/day, n=22); SD, standard deviation.
Estrone and estrone sulfate also differed among groups, and these products not only have biological activity but also undergo conversion to 17β-estradiol, thus serving as a storage depot for local production of estradiol. The hormonal profile that was associated with the least carotid intima medial thickening in EPAT was one in which free 17β-estradiol increased concomitant with decreases in free testosterone. In EPAT, serum 17β-estradiol averaged 68.2±16.2 pg/mL. 56 Therefore, additional analysis of the KEEPS outcomes relative to various ratios of free 17β-estradiol to free testosterone might be warranted.
Taken together, these studies, including KEEPS, provide evidence to support the current treatment guidelines for the noncontraceptive use of hormones for treatment of menopausal symptoms in postmenopausal women and not for prevention of cardiovascular disease. 57,58 The exception would be women who have undergone oophorectomy prior to the age of natural menopause, as in these women, hormonal supplementation slows progression of cardiovascular disease and reduces all-cause and cardiovascular mortality. 59 –62 Although current guidelines are for use of these products for the shortest period of time, the WHI, EPAT, and KEEPS studies do not provide data to support use for a specified time period. For women without ovaries, epidemiology data suggest use at least until the time of natural menopause. 63 However, DOPS provides evidence that longer use, up to 10 years, may be appropriate for prevention of cardiovascular disease 42 without increasing breast cancer risk. Both EPAT and KEEPS were of insufficient duration to measure breast cancer outcomes.
Future Considerations
Basic and clinical investigations into mechanisms and noncontraceptive actions of sex steroids progressed rapidly in the 1990s. With the termination of the WHI, federal funding for hormone research in the United States dropped significantly, and funding for other long-term hormone treatment trials is unlikely in the future. Indeed, the KEEPS trial was funded by a not-for-profit foundation, and attempts to obtain federal grants for further analysis of stored samples have been unsuccessful. These trends are unfortunate, given the continued clinical use of hormone products—for example, increased use of testosterone among men and so- called bioidentical products in women, neither of which has solid basic or clinical data sets upon which to guide clinical decisions.
Follow-up and analysis of data from the WHI are likely to continue. Such analyses will provide insight into aging processes in women following hormone use. However, relating data from the WHI to women who are currently using hormonal products may not be relevant, given the changes in clinical prescribing practice toward lower doses of CEE and other hormone formulations and delivery modalities since the cessation of the WHI. Additional epidemiological assessments may be warranted, as population demographics have changed since the early 1990s, with increases in prevalence of obesity, which influences endogenous estrogen, 64 use of lipid-lowering medications, and consumption of soy products and other food additives. Furthermore, exposure to environmental estrogen receptor modulators may interact or compete with endogenous sex steroid hormones, with collective effects showing different geographic distributions, depending upon use of such products in urban compared to rural environments. Consumption of probiotics that modulate the gut microbiome may influence metabolism of soy products to bioactive estrogen receptor modulators that, when absorbed into the hepatic circulation, could have systemic effects. 65 These variables will need to be considered in the design of future studies.
Metabolism of sex steroids is complicated. 66 The interactions among the various sex steroids need to be investigated in both women and men; in addition, as the field of pharmacogenomics matures, variation in the multiple synthetic and catabolic enzymes associated with estrogen metabolism should be considered not only according to specific single-nucleotide polymorphisms but also in allele frequency within the study population. 67 For example, the gene for SULTA1, an enzyme involved in the sulfonation of estrone and 17β-estradiol, has multiple copy numbers (Fig. 4). Genetic variations associated with SULTA1 may relate to a woman's response to hormonal therapy, including hormone-associated risk for cancer. Consideration of allele frequency—reflecting in essence a “gene dose” (single-nucleotide polymorphism times allele frequency)—may provide new insights into genetic variation when analysis of a single- nucleotide polymorphism has failed to translate into clinical relevance. Genetic analysis such as this, together with other genes associated with mechanisms of vascular remodeling, could be used to develop an algorithm to estimate benefits and risks associated with use of hormonal treatment in the future.
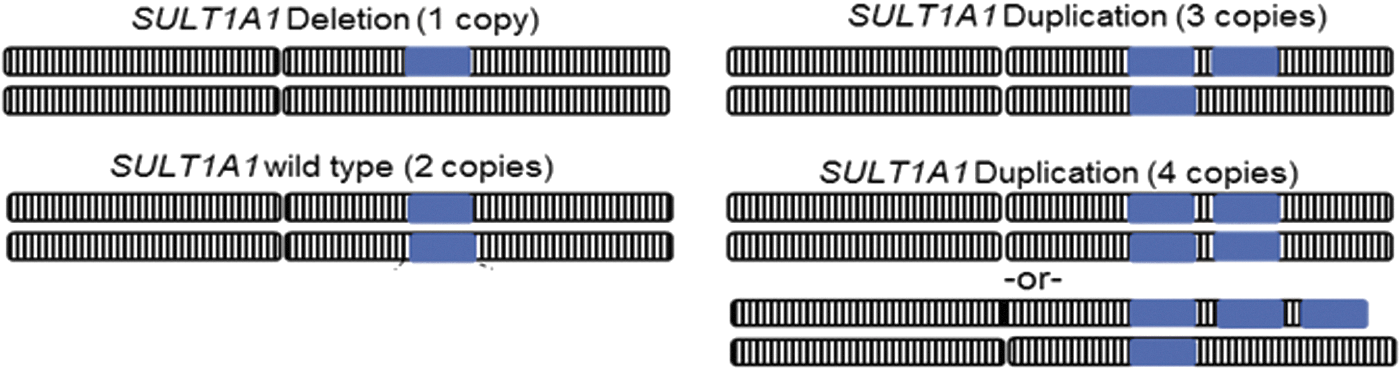
Schematic of copy number variance in the gene for SULTA1, an enzyme involved in the sulfonation of estrone and 17β-estradiol. This gene may have more than one copy number. Therefore, a single-nucleotide polymorphism (SNP) may be present on multiple alleles. The effect of a particular SNP would be magnified, depending upon the number of copies of the allele, giving a “gene dose” effect.
In spite of these challenges, additional funding for investigations into basic and clinical mechanisms of sex steroids and their modulation of life-long cardiovascular risk is essential as hormone products continue to be used by women and men. As Dr. Bush summarized so well in her Elizabeth Blackwell Lecture at Mayo Clinic in 2000, “Truth exists and waits to be sampled. No one study has all the truth”. 68 Additional studies will provide additional truth.
Footnotes
Acknowledgments
The author gratefully acknowledges and thanks her Mayo Clinic colleagues, who have provided their insight into clinical challenges and expert technical and intellectual support; her KEEPS trial collaborators, who continually challenge existing paradigms and seek evidence upon which to base medical practice; and to all the women who participate in clinical trials for the benefit of future generations. Dr. Miller's research is funded by grants from the National Institutes of Health AG44170, HD65987 and HL90639 and the Mayo Foundation. The Mayo site for the KEEPS was funded by a grant from the Aurora Foundation to the Kronos Longevity Research Institute.
Author Disclosure Statement
No competing financial interests exist.